This article has been
cited by other articles in ScienceCentral.
Abstract
Objectives
We conducted multi-directional language development tests as a part of the Research on Sensory and Communicative Disorders (RSVD) in Japan. This report discusses findings as well as factors that led to better results in children with severe-profound hearing loss.
Methods
We evaluated multiple language development tests in 33 Japanese children with cochlear implants (32 patients) and hearing aid (1 patient), including 1) Test for question and answer interaction development, 2) Word fluency test, 3) Japanese version of the Peabody picture vocabulary test-revised, 4) The standardized comprehension test of abstract words, 5) The screening test of reading and writing for Japanese primary school children, 6) The syntactic processing test of aphasia, 7) Criterion-referenced testing (CRT) for Japanese language and mathematics, 8) Pervasive development disorders ASJ rating scales, and 9) Raven's colored progressive matrices. Furthermore, we investigated the factors believed to account for the better performances in these tests. The first group, group A, consisted of 14 children with higher scores in all tests than the national average for children with hearing difficulty. The second group, group B, included 19 children that scored below the national average in any of the tests.
Results
Overall, the results show that 76.2% of the scores obtained by the children in these tests exceeded the national average scores of children with hearing difficulty. The children who finished above average on all tests had undergone a longer period of regular habilitation in our rehabilitation center, had their implants earlier in life, were exposed to more auditory verbal/oral communication in their education at affiliated institutions, and were more likely to have been integrated in a regular kindergarten before moving on to elementary school.
Conclusion
In this study, we suggest that taking the above four factors into consideration will have an affect on the language development of children with severe-profound hearing loss.
Keywords: Cochlear implant, Children, Research on sensory and communicative disorders, Language development, Japan
INTRODUCTION
Cochlear implantation (CI) is a highly specialized medical procedure for severe-to-profound hearing loss in patients all over the world. Newborn hearing screening (NHS) makes early detection and thus early intervention possible. NHS has allowed us to test 95% of newborns in Nagasaki over the last 4 years. With the rapid increase in use of pediatric CI, there is a need to develop more intensive, longitudinal, and standardized tests for auditory, speech, and communication skills and language development. There are very few packages that include multiple language development in the world.
As a part of the Research on Sensory and Communicative Disorders (RSCD) project in Japan, we examined various language development tests for children fitted with cochlear implants. This report discusses findings as well as factors that led to better results in children with severe-profound hearing loss.
METHODS AND RESULTS
Subjects
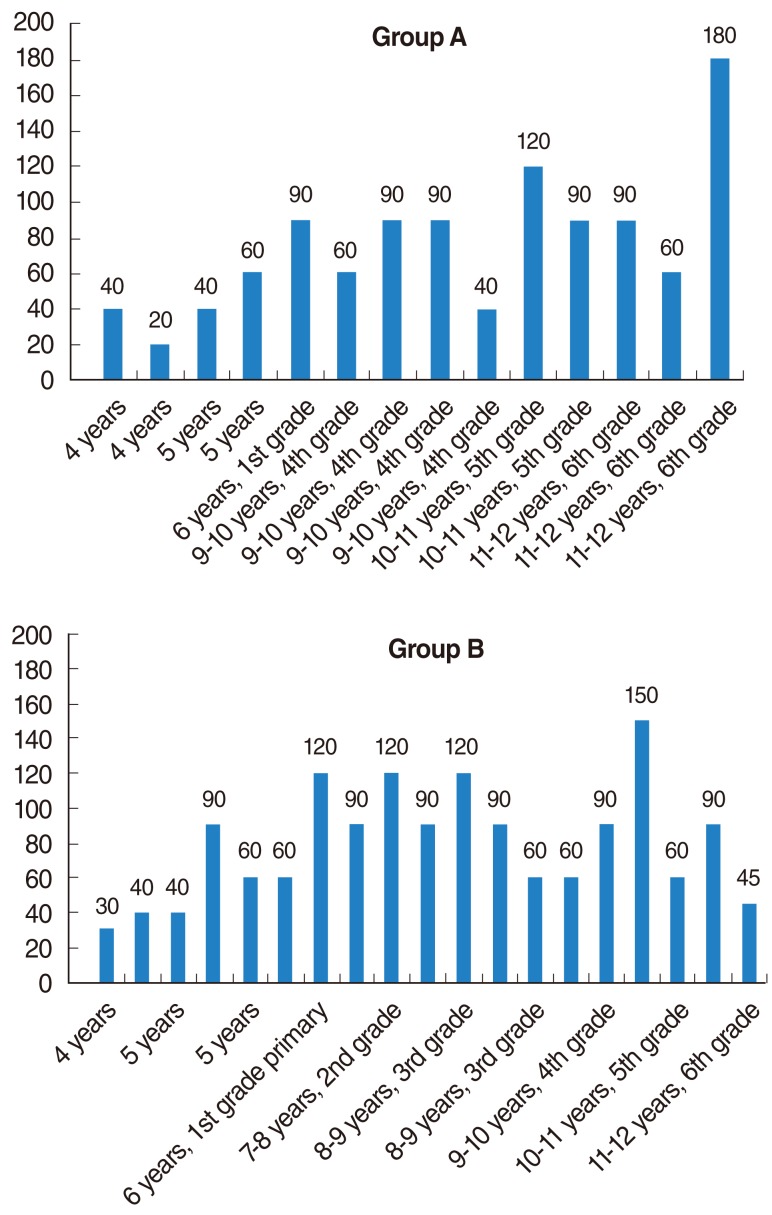
We examined 33 Japanese children (32 cochlear-implant patients and 1 hearing-aid patient) in our hearing center for the RSCD project. Children were selected according to the following criteria: 1) aged between 48 to 155 months and 2) congenital hearing impairment with a hearing level >70 dB (average over multiple frequency bands). Children unable to complete these tests because of further disabilities were not included. A consent form was provided in 2009. The age distribution was as follows: 4 years of age (4); 5 years (5); 6 years, i.e., 1st grade in primary school (4); 7-8 years, 2nd grade (2); 8-9 years, 3rd grade (4); 9-10 years, 4th grade (6); 10-11 years, 5th grade (4); and 11-12 years, 6th grade (4). Only one patient used hearing aids in both ears, and the remaining 32 children wore cochlear implants. Ten children had gone through the NHS process, while the other 23 had not. The age at fitting of hearing aids varied from 4 months to 5 years 4 months, and the age of cochlear implant surgery varied from 1 year 6 months to 6 years 3 months.
The tests were conducted between April 2009 and March 2010.
Methods 1
We asked the children to perform the following tests:
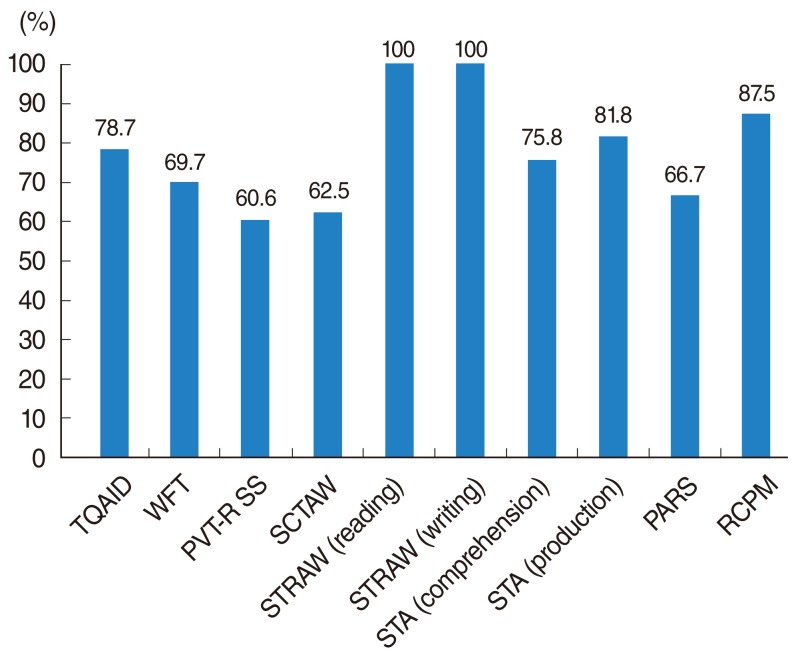
Test for question and answer interaction development (TQAID): This test aims to evaluate interpersonal communication skills (IPCS) with 57 questions divided into 10 categories.
Word fluency test (WFT): This test was conducted as a productive vocabulary task. Children were asked to generate as many words as possible from a given category in 60 seconds.
Japanese version of the Peabody picture vocabulary test-revised (PVTR).
The standardized comprehension test of abstract words (SCTAW): This test was conducted as comprehensive vocabulary tasks, and these consist of 32 or 45 abstract words selected from Japanese textbooks.
The screening test of reading and writing for Japanese primary school children (STRAW): This test was also conducted to examine the children's reading and writing abilities. Since preschool children have not yet learned Katakana or Kanji characters, the test for these children only included Hiragana characters.
The syntactic processing test of aphasia (STA): The STA, a syntax test that is like the test for the reception of grammar (TROG) for Japanese language users, is a test that evaluates the comprehension and production ability of syntactic structures.
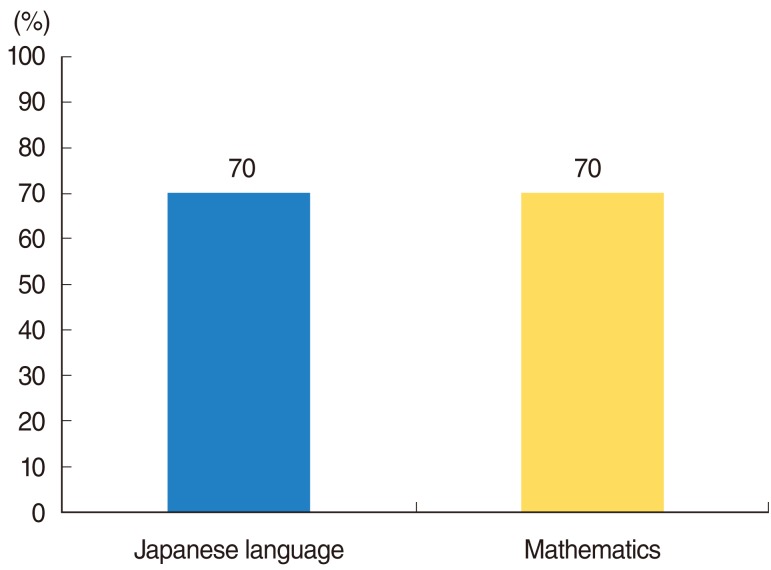
Criterion-referenced testing (CRT) for Japanese language and mathematics.
Pervasive development disorders ASJ rating scales (PARS) to determine autistic tendency.
Raven's colored progressive matrices (RCPM).
Results 1
The results showed that children suffering from hearing loss exceeded the national average of all children with hearing difficulties by at least 60.6% and up to 100% (
Fig. 1). A total of 76.2% of all scores exceeded the national average of children with hearing difficulties. On the CRT for Japanese language and mathematics, 70.0% of all scores exceeded the national average of scores obtained by normal-hearing children (
Fig. 2). We investigated the factors believed to account for the better performances in these tests.
Methods 2
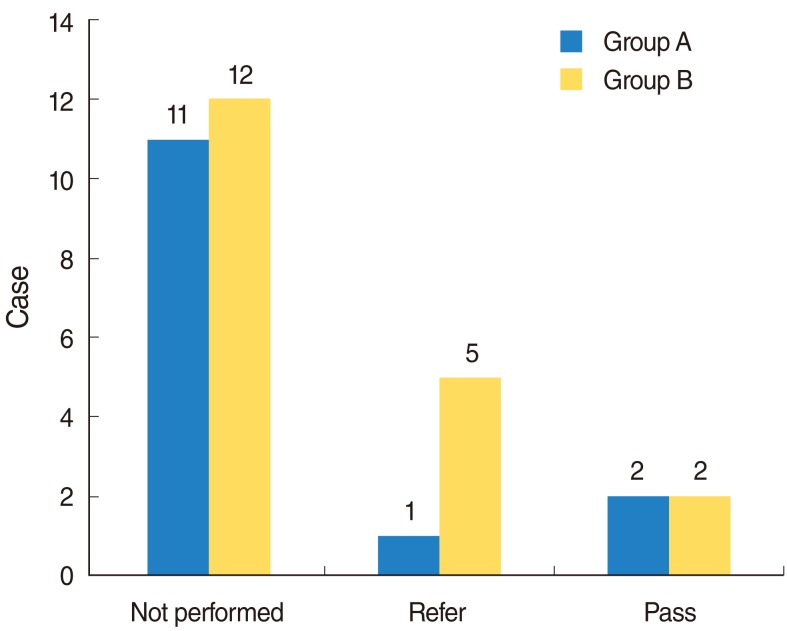
To determine the factors that allowed the children reported under Results 1 to have better results, we divided the children into two groups. The first group, group A, consisted of 14 children with higher scores in all tests than the national average for children with hearing difficulty. The second group, group B, included 19 children that scored below the national average in any of the tests.
Determining criteria within each group were as follows: 1) whether the child had gone through NHS, 2) the cause for the hearing loss, 3) the age at which the child began to wear hearing aids, 4) the age at which the child received CI, 5) number of visits to our hearing center since initial examination, 6) the amount of time since CI, 7) current average hearing level, 8) current average wearing threshold, 9) whether the child has any siblings, 10) amount of time spent studying at home on a daily basis, 11) educational method (school), 12) the period of integration and the period of auditory verbal/oral education, 13) educational institution child attended before entering primary school.
Results 2
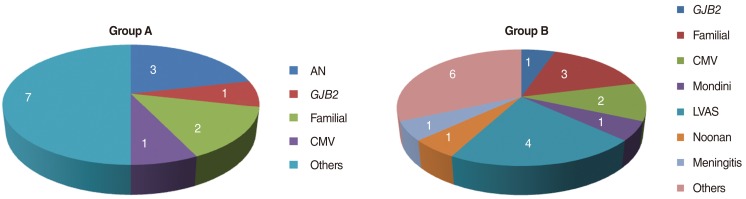
Quite a few children underwent NHS (
Fig. 3). Causes for deafness are shown in
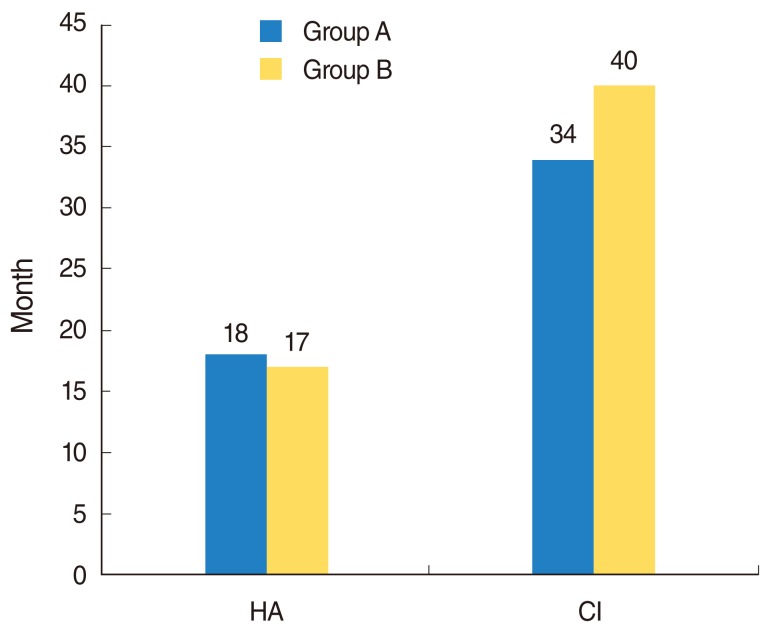
Fig. 4. There were many cases of inner ear and cochlear nerve anomaly and developmental disabilities in group B. There were no significant differences between the two groups in terms of the mean age for children to start wearing a hearing aid or the mean age for CI (
Fig. 5).
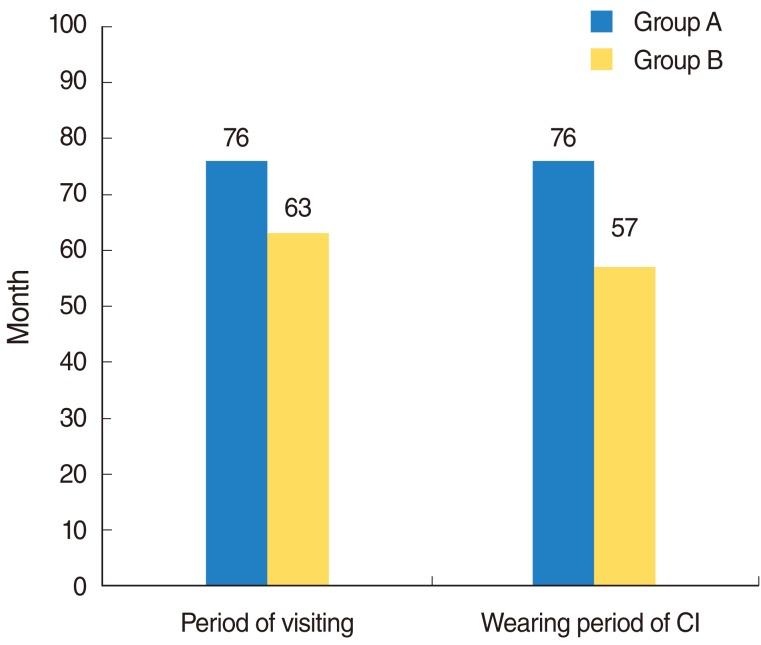
The mean period of the visit at our hearing center was significantly longer in group A than in group B (
P=0.049 <0.05
*) (
Fig. 6). The mean wearing period for the cochlear implant was significantly longer in group A than in group B (
P=0.02
*) (
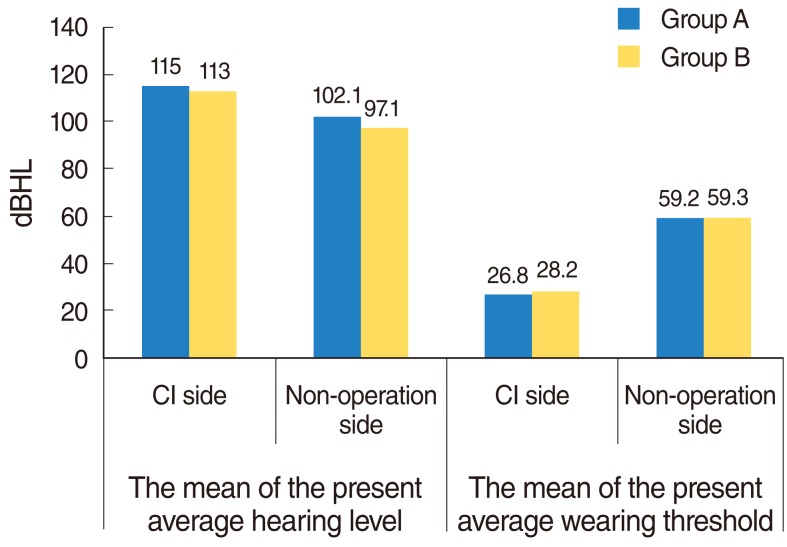
Fig. 6). The mean of the current average hearing level on their CI side was 115 dBHL for group A and 113 dBHL for group B on their CI side. On the non-operation side, it was 102.1 dBHL for group A and 97.1 dBHL for group B. The mean of the present average wearing threshold was 26.8 dBHL for group A and 28.2 dBHL for group B on their CI side. On the non-operation side, it was 59.2 dBHL for group A and 59.3 dBHL for group B. There were no significant differences in these results between the two groups (
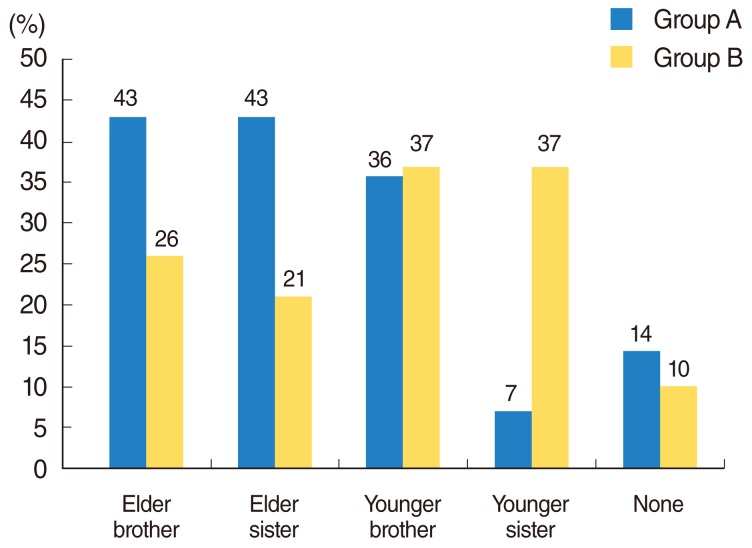
Fig. 7). Children in group A were more likely to have older siblings; however, there was no significant difference between groups A and B (
Fig. 8). The mean amount of time spent studying at home on a daily basis was 76.4 minutes for group A and 79.2 minutes for group B; these times were not significantly different (
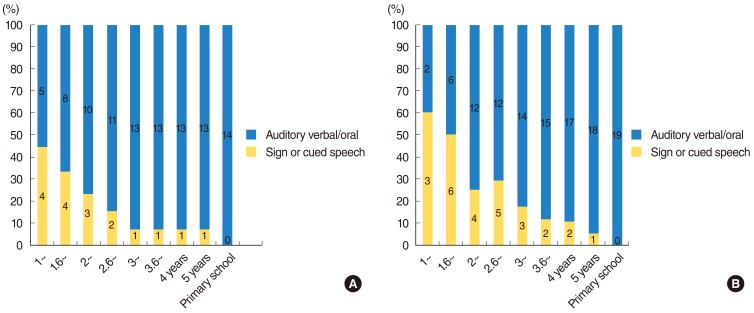
Fig. 9). From the age of 1 year to the end of preschool, the education for group A concentrated on auditory verbal and/or oral methods, while that for group B was geared towards sign or cued speech type education; there were significant differences between groups A and B (
P=0.003 <0.01
**) (
Fig. 10).
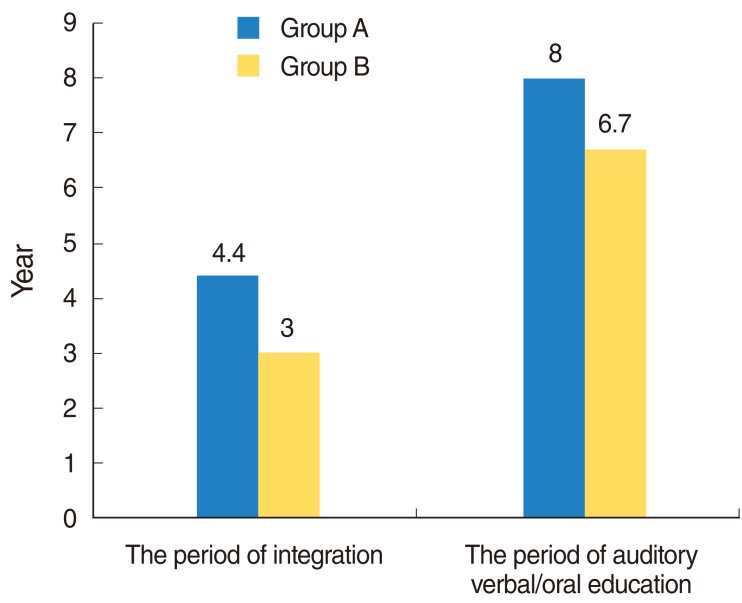
Children in group A attended regular school for 4.4 years, and those in group B attended for 3 years. Auditory verbal/oral education was 8 years for group A and 6.7 years for group B. While group A's education was longer than that of group B, there were no significant differences between the two groups (
Fig. 11).
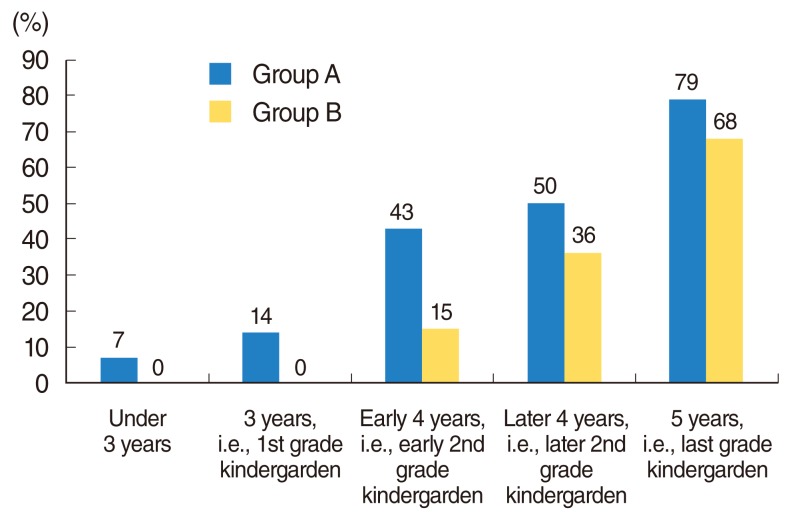
Fig. 12 shows the percentage of children who were integrated into regular kindergarten and nursery school before attending elementary school; there were significant differences between groups A and B (
P=0.01
*).
DISCUSSION
What factors are associated with good performance in language development in children with cochlear implants? It is very important to gauge the effectiveness of the appropriate intervention for hard-of-hearing infants. Research and evaluation of language development for children with cochlear implants have been conducted and should continue. However, there are very few packages that include multiple language development in the world (
1-
8).
In 2010, Fukushima et al. planned to assess the current status of hearing impaired children in Japan using the RSCD project, and many tests were used as a part of this nationwide research project. The study included 638 hearing-impaired children throughout Japan. To enroll hearing-impaired children, the RSCD project set up an open-invitation to various institutions, including schools for the deaf, schools for the hard-of-hearing, mainstream schools, and hospital training rooms.
We conducted multi-directional language development tests as a part of the RSVD in Japan. Overall, the results show that 76.2% of the scores obtained by the children in these tests exceeded the national average scores of children with hearing difficulty. The children that finished above average on all tests: 1). had undergone a longer period of regular habilitation in the rehabilitation center; 2) had their implants earlier in life; 3) were exposed to more auditory verbal/oral communication in their education at affiliated institutions; and 4) were more likely to have been integrated in a regular kindergarten before moving on to elementary school.
In the former report (
9), age at diagnosis of hearing loss was not a significant predictor of speech-language outcomes. The children who received auditory-based rehabilitation services during the preschool years demonstrated the potential to develop spoken language communication skills (
9). Our findings were similar. The lack of development of spoken language may induce restriction in learning and literacy, substantially compromising educational achievement and employment opportunities later on in life (
10). There is a report that the first and second years have a lasting positive impact on language, at least until kindergarten, and the probability that a child would reach normal language levels by kindergarten increased significantly with early intervention and cochlear implant use (
11). Niparko et al. (
12) reported that younger age at CI was associated with significantly steeper rate increases in comprehension (1.1; 95% confidence interval, 0.5 to 1.7 points per year younger) and expression (1.0; 95% confidence interval, 0.6 to 1.5 points per year younger). Our results were similar. In this study, we suggest that taking the above four factors into consideration will have an affect on the language development of children with severe-profound hearing loss.


 PDF
PDF Citation
Citation Print
Print


 XML Download
XML Download