

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) has been widely used for treatment of benign or malignant obstruction of the biliary and pancreatic ducts as well as biliary leaks.1,2 Cannulation of the bile duct remains the most important and often rate-limiting step for a successful ERCP. The success of biliary cannulation depends on several factors including skill and experience of the endoscopist, patient anatomy, presence of ampullary or pancreatic tumors, and availability of specialized accessories.3,4 Even in the hands of experienced endoscopists, deep biliary cannulation is achieved by the conventional way only in approximately 90% of the cases.5 In the remaining cases, precut sphincterotomy is commonly used, achieving an additional success rate of 77% to 91%.6,7 Desilets and Howell8 classified precut techniques into two broad types: needle knife sphincterotomy (NKS) and non-needle-knife types. Needle-knife precut sphincterotomy is the most commonly used technique to date.
Needle-knife precut papillotomy is a complex procedure and should be performed by experts with reasonable experience with ERCP9 because the control over direction, length, and depth is often not optimum. The presumed risks and morbidity associated with NKS include bleeding, perforation and increased risk of post-ERCP pancreatitis.7,10,11 Sometimes during bowing of the sphincterotome/cannula and the use of a guide wire to facilitate cannulation, inadvertent formation of a false passage occurs in the direction of 10 to 11 o'clock. This is generally considered an undesirable event. Burdick et al.12 for the first time used this false tract formation as an opportunity to achieve selective biliary cannulation by applying an intramucosal incision technique. In this review, we discuss this non-needle technique of precut sphincterotomy and also share our experience using "Burdick's technique."
INTRAMUCOSAL INCISION (BURDICK'S TECHNIQUE)
In 2002, Burdick et al.12 published a small series of six patients, in which they described the intramural incision technique as safe and effective in performing selective biliary cannulation. Since then two additional studies have also shown the usefulness of this technique.13,14
Technique
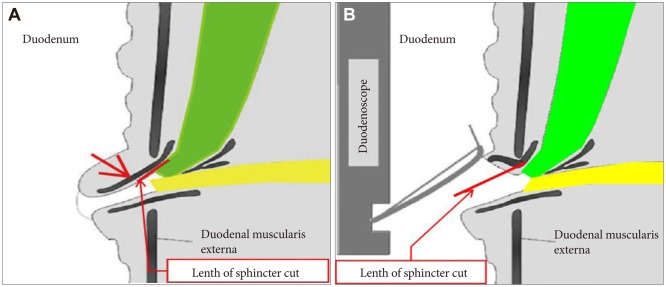
After engaging the papilla, the papillotome tip is usually positioned in the 10 to 11 o'clock orientation and the position is often confirmed fluoroscopically. The papillotome is bowed and a hydrophilic guide wire is gently advanced under fluoroscopic guidance in the direction of the 10 to 11 o'clock position. Instead of entering the bile duct, the guide wire sometime exits the papilla at the 10 to 11 o'clock position, creating an intramural false passage (Fig. 1A). After confirming the position of guide wire below the horizontal fold in order to avoid duodenal perforation, the papillotome is then relaxed and passed over the guide wire which is visible across the ampulla. The papillotome wire is then flexed and the intramural segment incised by using a pure cutting electrosurgical current (Fig. 1B). Only the mucosal bridge of tissue proximal to the papilla is divided and that for only 1 to 2 cm above the sphincteric orifice, with the aim of exposing the submucosal structures. After this, the biliary and pancreatic orifices become clearly visible (Supplementary Video 1 [available online at http://www.e-ce.org/]). The transmural incision is completed and the bile duct is selectively cannulated in the conventional way (Fig. 1C).
Fig. 2 show the schematic diagram of the anatomy of mucosal bridge formation due to a false tract and its consequent incision, leading to shortening of the sphincter segment of the ampulla and facilitating selective biliary cannulation.
Modification of Burdick's technique
Misra and Dwivedi13 and Thomas et al.14 have applied this technique with some modifications. First, this technique has been applied only when there is a spontaneous formation of a false tract in the desired direction of 10 to 11 o'clock by the guidewire or sphincterotome and not done intentionally, as was the case in the original Burdick's technique. However, in some patients in whom a false tract was formed during ERCP but the tip of the papillotome did not pierce the intramural part of the papilla through and through, attempts were made to deliberately puncture the intramural part of the papillary mucosa either by forceful angulations of sphincterotome, creating a "dog-leg" bend in the ampullary segment, or with a zebra guide wire (Boston Scientific, Marlborough, MA, USA) with a bowed papillotome.
Second, in Burdick's technique, fluoroscopy was used for positioning the guide wire, whereas Misra and Dwivedi13 and Thomas et al.14 used direct vision to achieve the same objective. According to their opinion, fluoroscopic images may not be very accurate in the area of the papilla, and visualization of the tip of the guide wire may not be precise. Instead, direct visualization of the sphincterotome abutting the mucosa of the intramural part of the papilla at around the 10 to 11 o'clock position is more reliable.
Third, as opposed to a hydrophilic guide wire used by Burdick et al.,12 these studies used a zebra guide wire (Boston Scientific) to puncture the intramural part of the papilla. The reason for this is that the hydrophilic tip of the guide wire is too soft compared with the tip of the zebra guide wire for puncturing the mucosa of the intramural part of the papilla.
ADVANTAGES AND LIMITATIONS OF BURDICK'S TECHNIQUE
The advantage of the incision in Burdick's technique over that in a conventional NKS is that, in the Burdick's technique, the incision is well-controlled because the sphincterotome with the guide wire is inside the tissue in a stable position, and cutting is done without much up-and-down movement as is required with needle knife. Moreover, in contrast to NKS, the length of the incision is not an issue since only the intramural part of the papilla below the horizontal fold is incised, and therefore the technique can be safe not only for the usual anatomy but also in patients with a short segment of the papillary roof and an angulated ampulla. These aspects reduce the risk of duodenal perforation. On the other hand, with NKS, the site, length, and depth of incision are not fully controlled, leading to a significant complication rate. This technique can also be used to access the pancreatic duct system because both the duct openings are very clearly visible after the procedure has been completed.
The limitation of Burdick's technique is that it can be applied safely only when there is a false tract formation and the sphincterotome pierces the mucosa in the desired direction. However, the technique can also be deliberately attempted if the tip of the sphincterotome is visible as a bulge abutting the intramural segment of the papilla. The mucosa is pierced by sharply angulating the sphincterotome. This may not, however, succeed in all attempts.
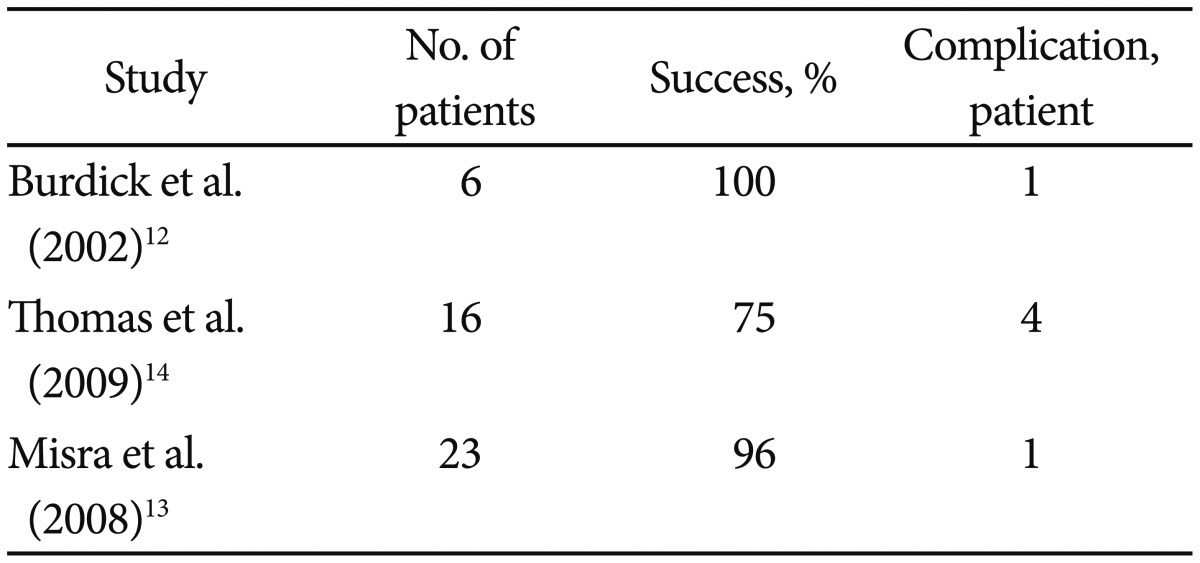
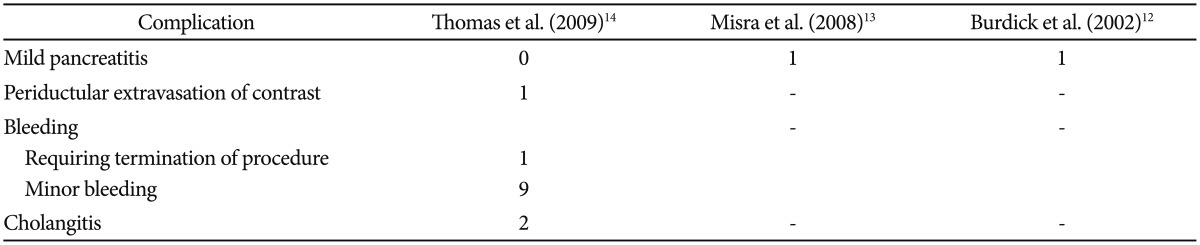
STUDIES EMPLOYING BURDICK'S TECHNIQUE
There are three small published studies,12,13,14 including Burdick's original description, employing the intramucosal incision technique of the precut method as shown in Tables 1, 2. Besides these studies, Deng et al.15 have also mentioned this technique in a few of their patients as a form of the precut method but details were not available. The success rate of this technique varies from 75% to 100% in the first attempt and almost 100% in the second attempt, which is usually done after 1 to 4 weeks. The complication rates are very low, approximately 4.5%, as compared to 8.5% in the needle knife precut technique. These studies thus advocate the safety and efficacy of Burdick's technique as a form of non-needle-knife precut sphincterotomy for selective biliary cannulation.
We have been using this technique at our center for more than 5 years. We have compared the safety and efficacy of Burdick's technique with that of needle-knife precut sphincterotomy. In our study (unpublished), an analysis was done on data from 2,952 patients who underwent ERCP for biliary between January 2009 and April 2014 where bile duct access were desired (Table 3). The intramucosal incision technique was performed in 34 (1.1%) of these 2,952 patients. Success rates were 94.1% (32 out of 34 patients) after the first ERCP and 97% (33 out of 34 patients) after the second attempt at ERCP 1 week later.
The failure of the procedure in the first case was caused by tissue edema due to contrast extravagation, leading to poor visualization of the papilla, and in the second case due to bleeding. During the same period, the needle-knife precut procedure was performed in 94 patients (3.18%) and was successful in 86 patients (91.5%). In Burdick's group, only one patient (2.9%) developed complications in the form of postsphincterotomy bleeding, which was successfully controlled with balloon tamponade. In the needle-knife group, four patients (4.2%) developed complications in the form of bleeding (n=1), pancreatitis (n=2), and perforation (n=1). All these four patients were managed conservatively without fatalities or need for surgery. Hence our study also advocates the safety and feasibility of Burdick's technique as a salvage procedure in difficult biliary cannulation. We attempt this technique only when the false tract is formed in the desired direction of bile duct cannulation.
CONCLUSIONS
The intramucosal incision technique (Burdick's technique) appears to be safe and effective and can be used as a non-needle-knife precut technique in difficult biliary cannulation if a partial or complete false tract has formed in the desired direction. Use of this technique is an example of using an undesired event to our advantage. Additional data are however required to assess whether this technique can be used as a planned procedure rather than a salvage method.


 XML Download
XML Download