

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atopic dermatitis (AD) in children increases the risk of food allergies, asthma, allergic rhinitis, and other immune-mediated inflammatory diseases, as well as mental health disorders, and impairs not only the patients’ but also their family members’ quality of life.1234
AD usually begins in infancy and often improves before school age, but may persist or recur after school age. AD is increasingly considered a lifelong illness presented by waxing and waning symptoms. Currently, there has been increase in prevalence of late onset AD. Moreover, recent epidemiological evidences suggest that the prevalence of AD in school-aged children has exceeded that in preschool children.56 AD is known as a heterogeneous disease that differs in age of onset, disease course, clinical symptoms, symptom severity, and risk of comorbidity.
Since AD has no disease-specific diagnostic test, it can be diagnosed when various clinical findings satisfy diagnostic criteria. However, AD shows different clinical findings according to age, ethnicity, and region. The most widely accepted diagnostic criteria by Hanifin and Rajka,7 which consists of 4 major and 23 minor criteria, is quite complex and has limitations of not reflecting the different characteristics of each country. Although there are some studies on AD in infants and preschool children,18 little is known about the clinical characteristics of AD in children and adolescents in Korea. Furthermore, there are few studies on differences in clinical characteristics according to onset age in children with AD. Therefore, in order to prepare a diagnostic guideline representing the phenotype of AD in children and adolescents in Korea, it is necessary to investigate on the characteristics of AD. In addition, there were few data on the characteristics of moderate to severe AD in school-aged children and adolescents, which are expected to differ from those of mild AD.
This multicenter study aimed to investigate the phenotype and clinical characteristics according to the onset age and severity of AD in school-aged children and adolescents in Korea.
METHODS
Study participants
The study population consisted of children with AD aged 6–18 years who presented to the pediatric allergy clinics of 18 secondary and tertiary hospitals nationwide. Hanifin and Rajka’s diagnostic criteria7 were used for the diagnosis of AD. Patients who consented to the use of their data, including detailed medical history, clinical features, severity assessments, and allergy test results, were included in the study.
Case report forms
All interview contents, examination findings, and laboratory test results were recorded in case report forms. Data on birth history, breastfeeding history, accompanying allergic diseases, family history of allergic diseases, age of AD onset, exacerbating factors, skin care status, and treatment history including systemic antibiotics, steroids or immunosuppressants were collected. Pediatric allergy specialists examined the patients, evaluated the symptoms that met Hanifin and Rajka’s minor criteria, investigated the AD lesion sites, and determined the disease severity using both the SCORing Atopic Dermatitis (SCORAD) tool and the Eczema Area and Severity Index (EASI). Numerical Rating Scale (NRS) scores for itching and sleep disturbance were recorded separately. The Children’s Dermatology Life Quality Index (CDLQI) was also used. The CDLQI is rated on a scale from 0 to 30, with higher scores indicating poorer quality of life.9 Moreover, sleep durations were queried.
Allergen sensitization was evaluated using a skin prick test or serum specific immunoglobulin E (ImmunoCAP; ThermoFisher, Uppsala, Sweden) for common allergens (Dermatophagoides pteronyssinus [Der p], Dermatophagoides farinae [Der f], birch, alder, oak, mugwort, ragweed, Japanese hop, Bermuda grass, timothy grass, dog epithelium, cat epithelium, Alternaria spp., and Aspergillus spp.).
Grouping according to onset age and severity
The patients were classified into three groups according to AD onset age. Patients whose symptoms developed under the age of 2 years were assigned to an infancy-onset group. Patients with symptoms appearing between the ages of two and five years were included in a preschool-onset group. Patients whose symptoms first occurred after the age of six years were assigned to a childhood-onset group.
The patients were also divided into groups according to disease severity. Patients with a SCORAD of less than 25 were included in a mild AD group. Patients with a score between 25 and 50 were assigned to a moderate AD group. Patients with a higher score than 50 were included in a severe AD group.
Statistical analysis
To describe the basic characteristics of the patients, continuous variables were summarized as means and standard deviations, and categorical variables were expressed as frequencies and percentages. ANOVA or linear-by-linear association was used to compare severity, presence or absence of other allergic diseases, family history of allergic diseases, and test findings between the groups. A P value of < 0.05 was considered statistically significant. All analyses were performed using SPSS version 26.0 (IBM, Armonk, NY, USA).
RESULTS
Patients’ demographic characteristics and onset age
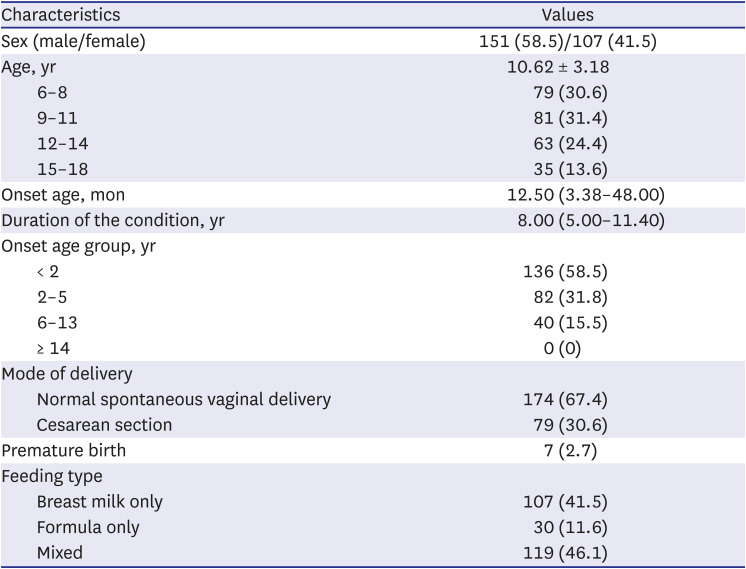
A total of 258 patients with a mean age of 10.6 years were included in the study. Children aged 6-11 years accounted for 62% (160/258), and adolescents aged 12 years or older accounted for 38% (98/258). The median age of AD onset was 12.5 months, and the median duration of the disease was 8 years. The infancy-onset group accounted for 58.5%, the preschool-onset group accounted for 31.8%, and the childhood-onset group accounted for 15.5% (Table 1). Among all patients, 87.6% were breastfed, and 59.7% were breastfed for more than six months. Of all patients, 39.1% were weaned late, after six months of age.
Table 1
Demographic characteristics of the study population (N = 258)
Comorbid allergic diseases and family history of allergic diseases
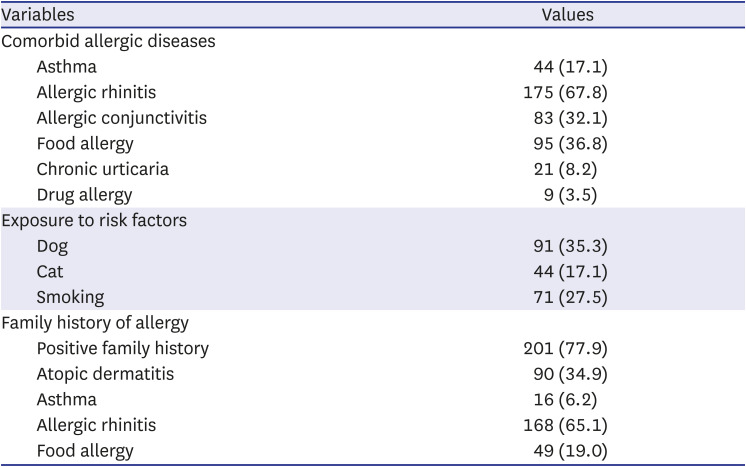
Among the concomitant allergic diseases, allergic rhinitis was the most common (67.8%), followed by food allergy (36.8%). Thirty-five percent of the patients were exposed to dogs, 17% to cats, and 27% indirectly to smoking. Seventy-eight percent of the patients had a family history of at least one allergic disease; allergic rhinitis was the most common (65.1%), followed by AD (35%) (Table 2).
Table 2
Clinical characteristics of the study population (N = 258)
Disease severity
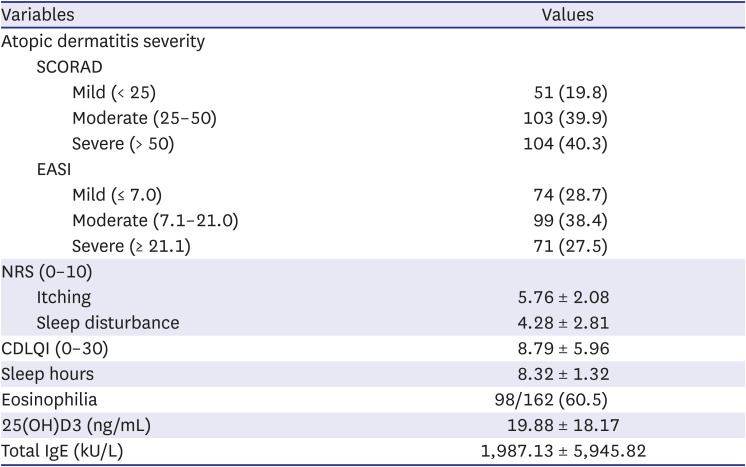
Severe AD group accounted for 40.3% according to SCORAD and 27.5% according to the EASI. The mean subjective NRS scores were 5.8 for itching and 4.3 for sleep disturbance. The average CDLQI score was 8.8, and the mean sleep duration was 8.3 hours (Table 3).
Table 3
Disease severity and laboratory findings of the study population (N = 258)
Comparison of patients according to onset age
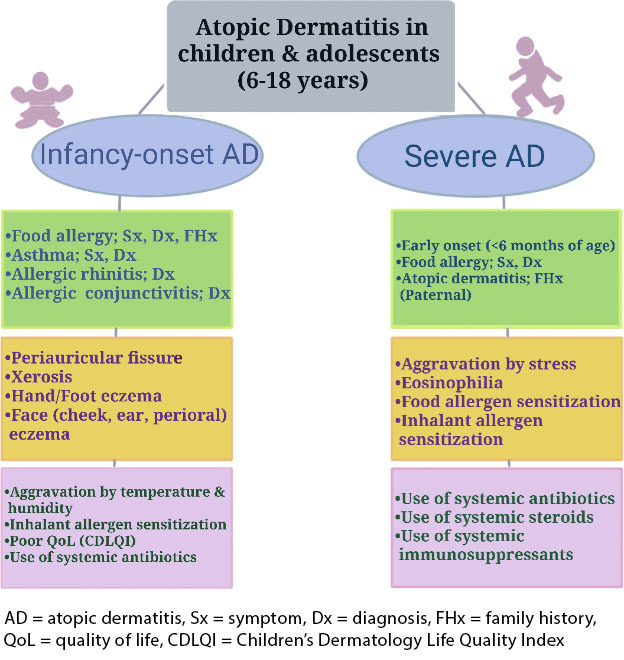
Severe AD with SCORAD of 50 or more was 44.9% in the infancy-onset group and 32.5% in the childhood-onset group. When the severity was divided by EASI, it was 28.7% in the infancy-onset group and 22.5% in the childhood-onset group. The SCORAD and EASI scores tended to be higher in the earlier onset groups than in the late onset group. However, the differences between the groups were not statistically significant (P = 0.054, and P = 0.073, respectively). Food allergy symptoms reported by parents were significantly more common in the infancy-onset group (58.1%) than in the preschool-onset (36.6%) and childhood-onset groups (17.5%; P < 0.001). Symptoms of asthma were also significantly more common in the infancy-onset group (34.6%) than in preschool-onset (18.3%) and childhood-onset groups (5.0%; P < 0.001). Doctor confirmed food allergy, asthma, allergic rhinitis, and allergic conjunctivitis diagnoses were also significantly more common in the infancy-onset group (food allergy, asthma, allergic rhinitis: P < 0.001; allergic conjunctivitis: P = 0.020). In groups with younger onset age, there was a tendency to have a family history of food allergies. (P = 0.036).
Among Hanifin and Rajka’s minor criteria, xerosis was significantly more frequent in the infancy-onset group than in the other two groups. The earlier the onset age group, the more frequent the facial lesions, including periorbital, cheek, and ear lesions (P = 0.027, P = 0.007, and P = 0.037, respectively). Periauricular fissures were also very frequent in the infancy-onset group. In many children in the infancy-onset group, AD was aggravated by changes in temperature and humidity.
The rates of Der f sensitization were 72.8% in the infancy-onset group, 67.1% in the preschool-onset group, and 60.0% in the childhood-onset group. The rate of house dust mite sensitization was higher at younger ages (P = 0.004). Although there were lacking in data because not all patients were tested for all allergens, birch, oak, and weed pollen sensitization showed higher rates in the younger onset age groups. The rates of sensitization to one or more inhalant allergens were statistically significant; 82.4% in the infancy-onset group, 78.0% in the preschool-onset group, and 70.0% in the childhood-onset group (P = 0.012).
In terms of quality of life, the lower the onset age, the higher the CDLQI score and, therefore, the poorer the quality of life (P = 0.038). The use of systemic antibiotics due to AD was also most common (22.1%) in the infancy-onset group (P = 0.048). Table 4 summarizes the comparison of the characteristics of AD between the three onset age groups.
Table 4
Comparison of patient characteristics according to onset age
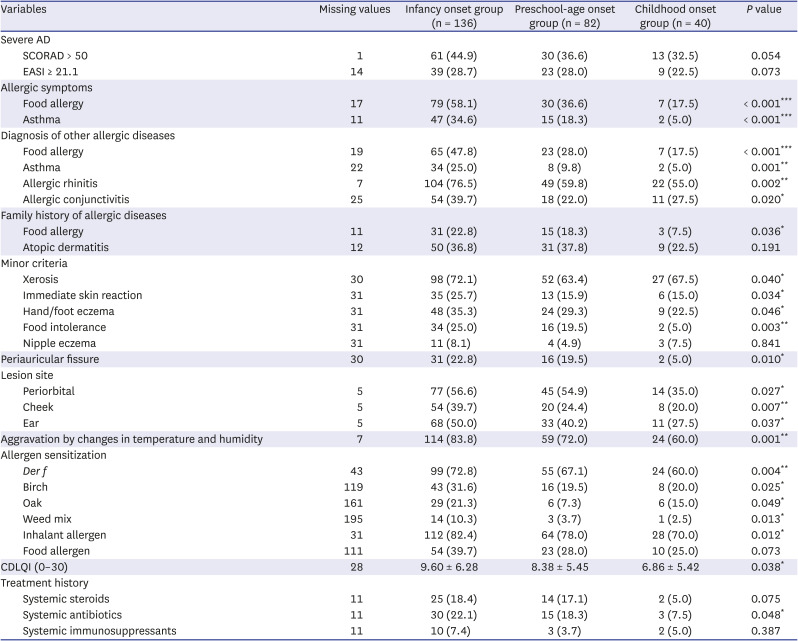
Values are presented as number (%), except for CDLQI (mean ± SD).
Some frequencies do not add up to the total number of cases because of missing values.
Statistically significant difference (*P < 0.05, **P < 0.01, ***P < 0.001).
AD = atopic dermatitis, SCORAD = SCORing Atopic Dermatitis, EASI = Eczema Area and Severity Index, Der f = Dermatophagoides farinae, CDLQI = Children’s Dermatology Life Quality Index.
Comparison of patients according to disease severity
According to SCORAD, patients aged 12 years or older tended to have more severe AD than patients aged 6–11 years. Over 50% of patients aged 12 years or older had severe AD.
The severity of AD did not differ significantly between patients with an onset under the age of two years, patients with an onset between the ages of two and five years, and patients with an onset after the age of six years. However, the difference was statistically significant when the onset age was divided into four groups: less than six months, between six months and one year, between two and five years, and six and over six years. The earlier the onset age, the more severe the condition (P = 0.018). Food allergy symptoms and diagnoses were significantly more common in severe AD patients (P = 0.005 and P = 0.003, respectively). Severe AD was significantly associated with a family history of AD (P = 0.048), especially a paternal history (P = 0.004). Moreover, severe AD was significantly exacerbated by stress or emotional changes (P < 0.001). The severity of the condition also significantly correlated with eosinophilia (P = 0.048).
The rates of Der p, dog epithelium, cat epithelium, Japanese hop, and weed mix sensitization were significantly higher in the severe AD group than in the mild and moderate AD groups (P = 0.017, P = 0.000, P = 0.038, P = 0.030, and P = 0.022, respectively). Overall, AD severity significantly correlated with inhalant allergen sensitization (P = 0.024). Food allergen sensitization was also significantly more common in the severe AD group (P = 0.041). Patients with severe AD used more systemic steroids, immunosuppressants, and antibiotics. As shown in Fig. 1, systemic antibiotics were used by 29.8%, systemic steroids were used by 22.1%, and systemic immunosuppressants were used by 9.6% of severe AD patients. The patient characteristics according to AD severity are summarized in Table 5.
Fig. 1
Systemic treatments used for severe atopic dermatitis in Korean school-aged children and adolescents.
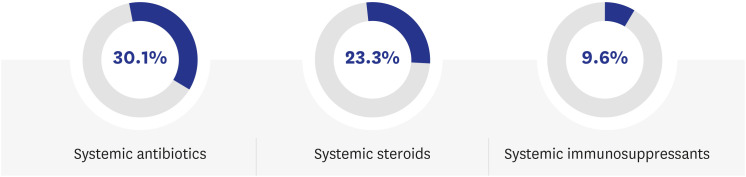
Table 5
Comparison of patient characteristics according to severity
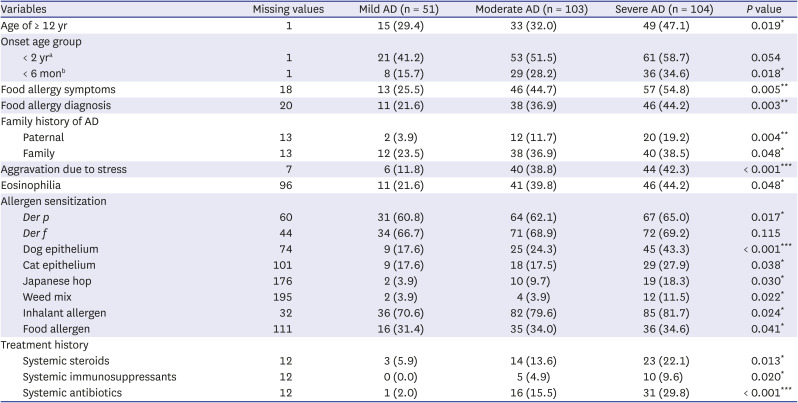
Values are presented as number (%), except for CDLQI (mean ± SD). Some frequencies do not add up to the total number of cases because of missing values.
Mild AD: SCORAD < 25; Moderate AD: SCORAD 25–50; Severe AD: SCORAD > 50.
AD = atopic dermatitis, SCORAD = SCORing Atopic Dermatitis, Der p = Dermatophagoides pteronyssinus, Der f = Dermatophagoides farinae, CDLQI = Children’s Dermatology Life Quality Index.
aOnset age group divided into < 2 years, 2–5 years, and ≥ 6 years; bonset age group divided into < 6 months, 6 months–1 years, 2–5 years, and ≥ 6 years.
Statistically significant difference (*P < 0.05, **P < 0.01, ***P < 0.001).
DISCUSSION
This is the first nationwide multicenter study to investigate phenotypes and characteristics of AD according to onset of age and severity in school-aged children and adolescents in Korea. This study is meaningful in that it analyzed the characteristics of patients who persisted AD until childhood or adolescent or who developed AD at a later age, rather than transient cases who improved AD before the age of 6 years. The limitation of this study is that there may be a selection bias in enrolling more severe patients because patients who visited secondary or tertiary hospitals were registered. However, the main goal of this study was not to analyze the characteristics and phenotype of all pediatric AD patients, but to analyze the characteristics and treatment status of early-onset group and severe group among school-aged children and adolescents with AD after the age of 6.
This study demonstrated that the infancy-onset AD is more likely to have food allergies, asthma symptoms and other allergic diseases, simultaneously. Since this was a cross-sectional study, it cannot explain a direct causal relationship, however, it suggests that the infancy-onset AD is a phenotype associated with an allergic march. In addition, the patients with infancy-onset AD had a higher family history of food allergies than those in other onset AD groups.
Depending on the age of onset, the AD phenotype can be classified into very early onset, occurring between the ages of 3 months and 2 years; early onset, between the ages of 2 and 6 years; childhood onset, between the ages of 6 and 14 years; adolescent onset, between the ages of 14 and 18 years; adult onset, between the ages of 20 and 60 years; and very late onset, after the age of 60 years. Very early onset accounts for 60–80% of all AD cases, and about 60% of them disappear by age of 2 years and 40% continue beyond age of 2 years, leading to an allergic march associated with allergic rhinitis and/or asthma. Early-onset AD is thought to be a risk factor for chronic diseases. Childhood-onset (6–14 years of age) and adolescent-onset (14–18 years of age) AD has been less studied.10
Birth cohort studies have demonstrated a link between early-onset AD and school-age asthma and allergic rhinitis.1112 In a cohort study following more than 3,000 infants for 5 years, children with eczema were 3.07 times more likely to develop asthma than children without eczema. The probability of developing asthma and allergic rhinitis increased with moderate to severe eczema (aOR 3.56 and 3.87, respectively), early-onset eczema (aOR 3.44 and 4.05, respectively), and persistent eczema (aOR 5.16 and 4.00, respectively). Another study showed that a family history of allergic diseases increased the risk of respiratory allergy in AD patients.12 In our study, a family history of food allergies was associated with infancy-onset AD, and a family history of AD was associated with severe AD. A 7-year follow-up study found that early-onset and persistent AD was associated with an increased risk of other atopic diseases and food allergen and aeroallergen sensitization.13 Another study on the relationship between allergen sensitization and allergic march in AD patients reported that AD without sensitization was not associated with an increased risk of asthma after the age of 3 (RR 0.46), whereas AD with sensitization increased the risk of asthma by more than 7 times (RR 7.04).1415 That study suggested that in AD, sensitization occurs through the skin, resulting in food allergies, which can lead to an allergic march that develops into respiratory allergies, such as asthma and allergic rhinitis. There is growing evidence of the importance of allergic sensitization through the skin.16 In children with AD, not only food allergens but also inhalant allergens can be sensitized through the skin, suggesting a link to allergic march.1617181920 In our study, food allergen sensitization was associated with more severe but not earlier onset AD, whereas inhalant allergen sensitization was significantly associated with both ADs. This is consistent with a study on children from the Copenhagen Prospective Studies on Asthma in Childhood, which found that early-onset AD and severity were associated with the development of aeroallergen sensitization during childhood.21 In a previous study, patients with early-onset and persistent AD often had high SCORAD scores at baseline, food allergen sensitization, and a family history of asthma, while FLG mutations were irrelevant.22 Recent evidence suggests that early-onset AD is a significant risk factor for the transition to other allergic diseases and that clinical characteristics such as onset age, severity, and family history may be more important for prognosis than genetic tests.810112324
In current study, 87.6% of children with AD had been breastfed, and 59.7% of them had been breastfed for more than six months. Breastfeeding has not shown a significant correlation with a high or low risk of AD, while it has shown a moderate correlation with a lower risk of asthma.25 Late introduction (after six months of age) of solid foods in children of our study was common (39.1%). This may be due to parents’ concerns over food allergies in infants with AD.
We investigated the common symptoms according to Hanifin and Rajka’s minor criteria and compared the common sites of skin lesions between the onset age groups. Food intolerance, immediate skin reaction, xerosis, and hand/foot eczema were significantly more common in the infancy-onset group. The earlier the onset, the higher the prevalence of lesions in the facial area, including the cheek, ear and periorbital area. In a study analyzing the differences in AD phenotype according to the age of onset, childhood-onset AD was associated with significantly higher rates of involvement of the anterior neck fold, scalp, face, eyelids, Dennie-Morgan folds, hands, feet, and nipples, higher incidence rates of conjunctivitis, cheilitis, pityriasis alba, keratosis pilaris/palmar hyperlinearity/ichthyosis, worsening clinical courses due to emotional or environmental factors, pruritus when sweating, and a stronger tendency toward cutaneous infections compared with adult-onset AD.26 The only characteristic that childhood-onset AD had in common with adult-onset AD was nummular eczema.26 A meta-analysis of age-related AD features found that the pediatric studies reported higher rates of dermatitis in the eyelids, auricular area, and ventral aspect of the wrists, exudative eczema, and seborrheic dermatitis-like features compared to the adult studies.27 In an American study on adults, patients over the age of 60 were often affected in the face and scalp, as well as in the buttocks or genitalia. The same study found no differences in lesion distribution according to age of onset (childhood or adulthood).28 However, in a study of adults in Korea, it was found that the flexor surface of arms and legs was more involved in the pre-adult-onset (age < 18 years) group than in the adult-onset group.29 It is noteworthy that in our study, periauricular fissures were particularly common (22.8%) in the infancy onset group and significantly more common than in the childhood onset group (5.0%; P = 0.010). Auricular involvement is known to be common in East Asian populations.27 The prevalence of periauricular eczema in Korean children has been reported to be up to 64.5% and to be associated with Staphylococcus aureus infection.30
AD occurring in the early stages of life is thought to significantly reduce quality of life. In our study, the mean value of CDLQI score in the infancy-onset group (9.60) was significantly higher than that in the childhood-onset group (6.86; P = 0.038). In a Korean study, CDLQI is correlated with AD severity scores as estimated by the SCORAD.31 A recent study reported that previous treatment with systemic immunosuppressants, more severe depressive symptoms, itch, impaired sleep, and perceived severity of dermatological symptoms were significant predictors of poor quality of life.32 Patients with AD have been found to exhibit inferior social functioning and mental health scores compared with the general population. Greater disease severity is associated with poorer quality of life and health-related quality of life, especially in children.33
In terms of systemic treatments, immunosuppressants were used by only 9.6% of the patients in the severe AD group, indicating that systemic immunosuppressants are not commonly used even in children with severe AD in Korea. A recent study found that AD treatment approaches differed considerably between Korean allergy specialists, pediatric allergy specialists, and dermatologists. Pediatric allergy specialists preferred wet wrap therapy and used few systemic immunosuppressants other than cyclosporin.34 This may be because the side effects of these drugs are more worrisome in children. Nevertheless, it is a fact that there are not many treatment options for severe AD in childhood. However, with the recent development of new drugs, the scope of treatment is expected to expand.
Although the present study was not a cohort study, we analyzed the clinical characteristics of AD in detail in children and adolescents aged 6 years and older, for whom there have been few data. Recently, clinical trials and approval of new AD drugs (e.g., dupilumab) have expanded to pediatric patients. Our study makes a significant contribution by analyzing the phenotypes and clinical features and demonstrating the phenotypic differences according to onset age and severity in Korean children and adolescents with AD. The results of current study can be used as important basic data for personalized treatments. This study found that the patients with early-onset AD group were more severe and had more other allergic diseases, highlighting the early management of AD in infants and young children. This study has a 5-year follow-up plan. New treatment plans for each AD phenotype should be developed by further tracking and analyzing the disease courses of these patients.
 XML Download
XML Download