

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It is known that individuals with spinal cord injury (SCI) are prone to be overweight, diabetic, have cardiovascular disease, and be at an increased risk of infection [1,2,3,4]. As the average life expectancy is increasing, individuals with chronic spinal cord injuries are living longer [1,3].
However, not all the individuals with SCI live healthy lives. Many face challenges in their daily activities and are restricted by various complications and disease states. The overall well-being and fitness are, in addition to the medical and surgical disease statuses, of the utmost importance. While spasticity, skin breakdown, susceptibility to infection, and orthopedic problems all affect the quality of life of individuals with SCI, cardiopulmonary fitness is also an essential aspect in this regard.
Continuous endurance training is required to maintain healthy cardiopulmonary function, and data must be obtained from the individuals with SCI to set up the proper exercise plans. Among such data, maximal oxygen consumption (VO2max) has been widely used as an indicator of cardiopulmonary capacity. This requires evaluation and comparison of cardiopulmonary capacity between individuals. For this reason, a set of reference values for Koreans would be necessary to evaluate the cardiopulmonary ability of Korean individuals with spinal cord injuries.
In Korea, there is large-scale data for healthy adult subjects. The study was done to evaluate cardiovascular performance under maximal exercise stress that included 731 healthy adult subjects performed in 1993 [5]. In this study, the maximum heart rate and VO2max at maximal exercise intensity were measured and tested on healthy adult male and female Koreans. This study was carried out using the Bruce method and the results are used as the normal reference value for Koreans. However, there has been a lack of studies in Korea evaluating cardiopulmonary function of individuals with SCI.
In 2006, there was a study of cardiopulmonary function and serum plasma lipid profile of SCI subjects using a wheelchair treadmill [3]. They found out that higher neurologic injuries showed lower VO2max. However, the limitations were that there were no comparative analyses with regular exercise and the aging process. Also, the study compared their results to a study of Sutbeyaz et al. [6], but unfortunately the exercise methods could not be directly compared because an arm ergometer was not used.
In addition, a domestic pilot study using rowing ergometer for the aerobic exercise of paraplegic individuals was performed in 2011 [2]. While this study reported that rowing ergometer exercise effectively improves the cardiovascular function of patients with SCI, it was limited by differences in injury level and the small number of subjects.
Currently, as the life expectancies and survival rates of individuals with SCI improve, the need for a higher quality of life is also increasing. Also, participation in physical activities and recreational sports is increasing among those with SCI. However, there is the danger of cardiovascular complications if these physical activities and recreational sports are not done at the proper intensity. In addition, there are a few exercise methods and devices that could be used depending on the neurologic injury level. Most are limited to arm ergometer exercises and weight training [7]. Therefore, a study needs to be conducted regarding the relationship between physical activity and the cardiopulmonary state of these individuals regarding age and neurological injury level.
Thus, we evaluated the cardiopulmonary capacity of subjects with varying degrees of neurologic injury levels of the spinal cord, age, and a history of regular exercise in Korean males with SCI.
MATERIALS AND METHODS
Subjects
Forty male subjects with SCI were included in this study. All subjects were at or over 20 years old. We obtained informed consent from all participants, and the study was approved by the Institutional Review Board of Wonju Severance Christian Hospital.
The participants of this study were male Korean individuals with SCI who could understand and follow the instructions from the examiners. Also, individuals with adequate strength and motor functions were chosen for the arm ergometer protocol. Individuals with medical problems, such as arrhythmia, dyspnea, orthopedic problems, skin breakdown, and pressure ulcers, were excluded from this study. Also, individuals who could not sustain an upright position on a wheelchair for at least an hour were excluded.
Cardiopulmonary fitness measurements
We monitored the electrocardiograph (ECG) activity with the ECG monitoring system Q-STRESS v3.5 (Cardiac Science, Bothell, WA, USA) during the study. We obtained the maximal oxygen consumption data from a metabolic measurement system, TrueOne 2400 (Parvo Medics, Sandy, UT, USA) with an arm ergometer 917900 (Lode BV, Groningen, The Netherlands) (Fig. 1).
In case of emergency situations, a doctor and a nurse were always in attendance during all the procedures. Also, an emergency kit was always ready for quick first aid in the case of any unexpected situations. All subjects went through the procedures in their personal wheelchairs.
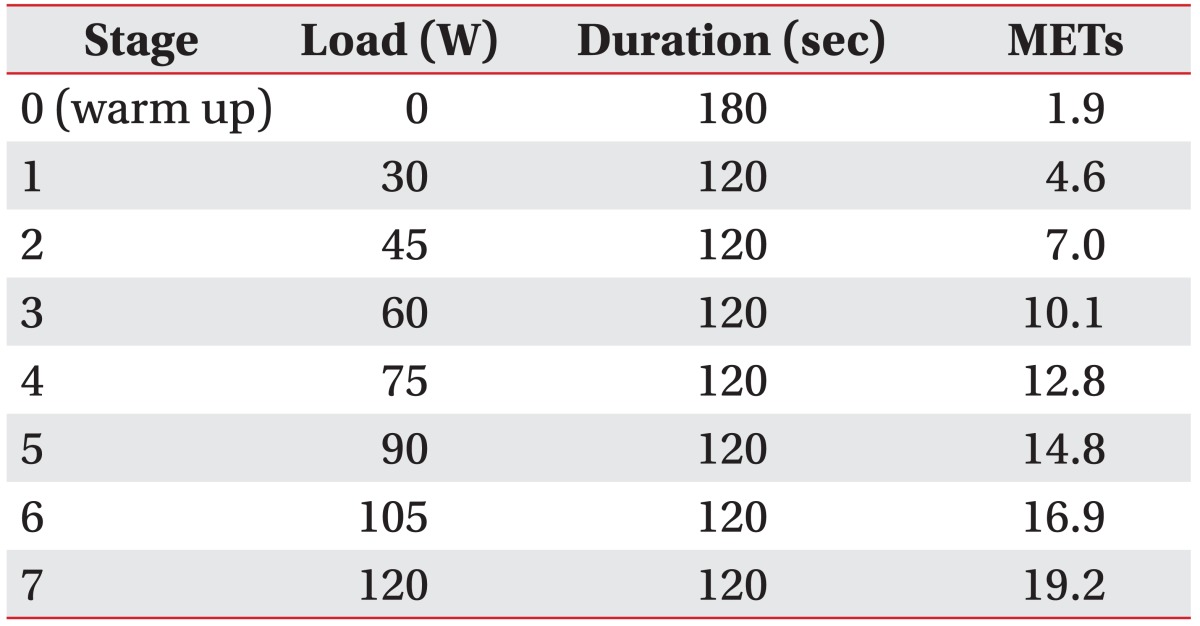
The study started with a warm-up exercise for three minutes, and the intensity was increased at two-minute intervals until exhaustion. The initial loading was 30 W and the speed was maintained at 60 revolutions per minute (rpm). The loading was increased by 15 W for each exercise stage and the protocol proceeded for 7 stages excluding the warm-up exercise (Table 1).
During the study, we checked the rating of perceived exertion (RPE) scores at each stage. The exercise was discontinued if VO2max reached a plateau or if the cycling rate dropped below 30 rpm. Also, we discontinued the exercise at any time if the subject experienced maximal exertion or wanted to stop.
Data analysis
The individuals were divided into groups based on their neurological injury levels. They were divided into cervical, thoracic, and lumbar groups. They were further divided into age groups of under 40, 40-49, and 50 and over. Also, the individuals were divided into two groups, an exercise group and a non-exercise group. Subjects in the exercise group were those that regularly participated in at least 3 sessions of one or more sports activity per week, and each session lasted at least 1 hour.
The VO2max of the subjects was compared considering their neurological levels, ages, and whether regular exercise was undertaken. The exercise group and the nonexercise group were compared under paraplegic subject parameters.
All data was analyzed using SPSS ver. 19.0 (IBM Inc., Armonk, NY, USA). Comparisons between the exercise group and the non-exercise group were performed using an independent t-test, while one-way ANOVA was used to compare the data obtained from the three groups divided according to age and the three groups divided according to neurologic injury level. Statistical significance was determined at p<0.05.
RESULTS
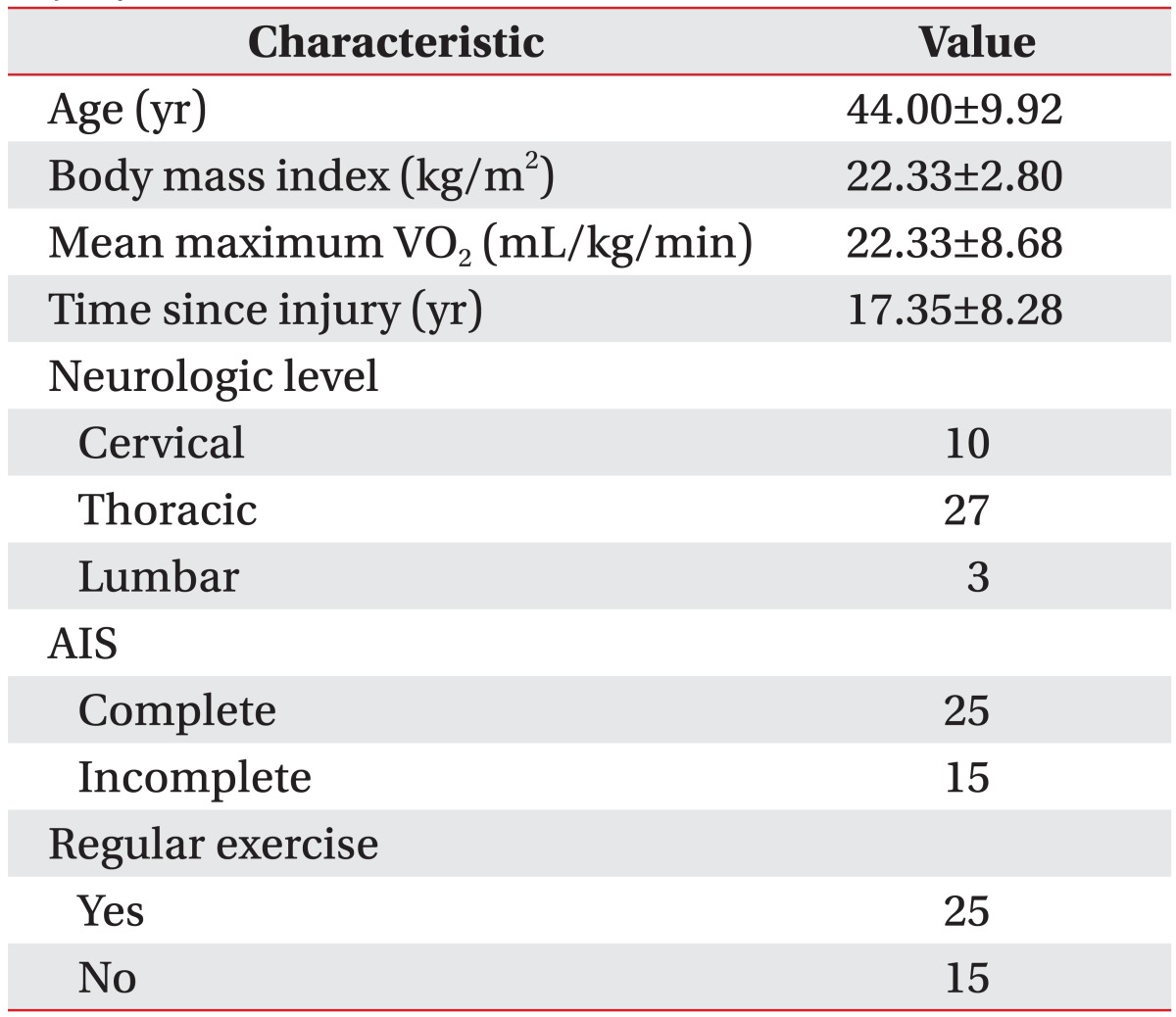
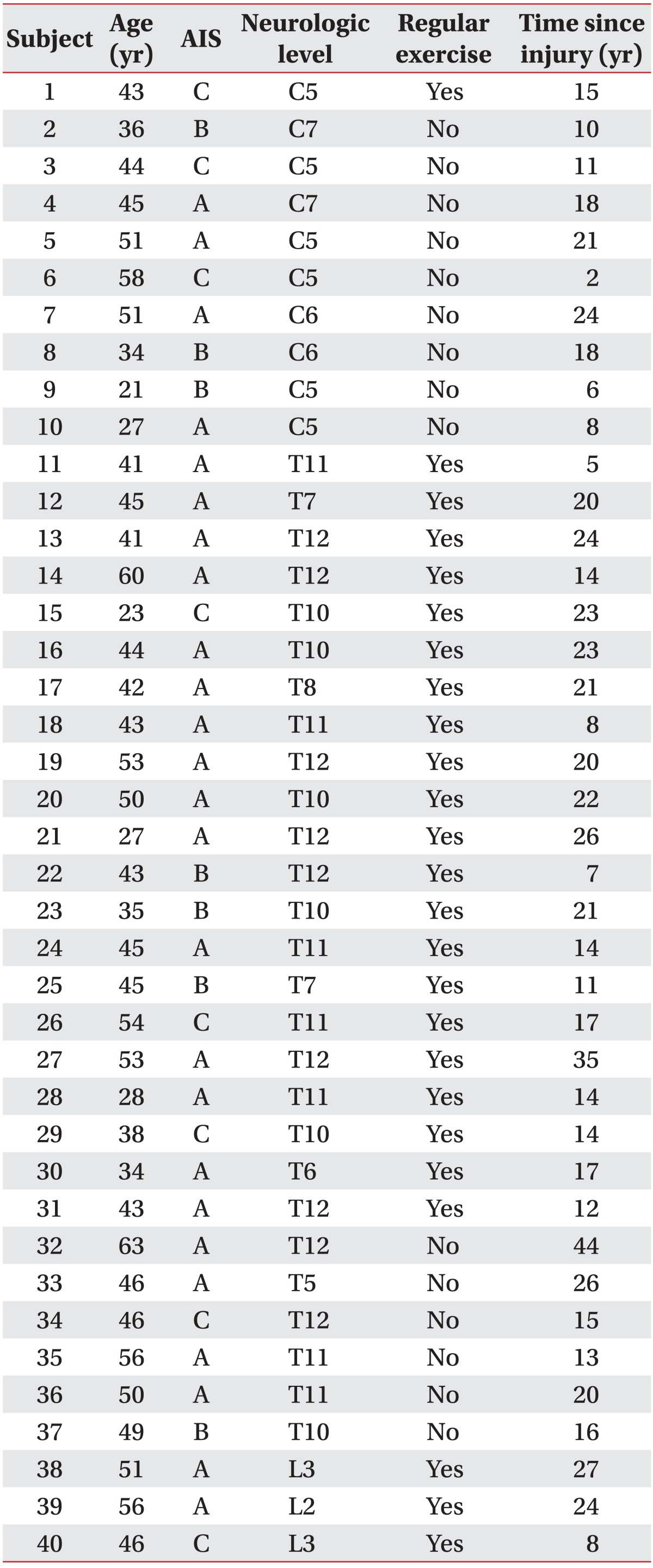
Forty male adults with SCI were chosen for the trials. The age range of the subjects was from 21 to 63 years and the average age was 44±9.92 years (Table 2). The neurologic levels of the subjects' injuries were 10 cervical, 27 thoracic, and 3 lumbar (Table 3). Among the 40 subjects, 10 subjects were under 39 years of age, 17 were 40-49 years old, and 13 were 50 years old or older.
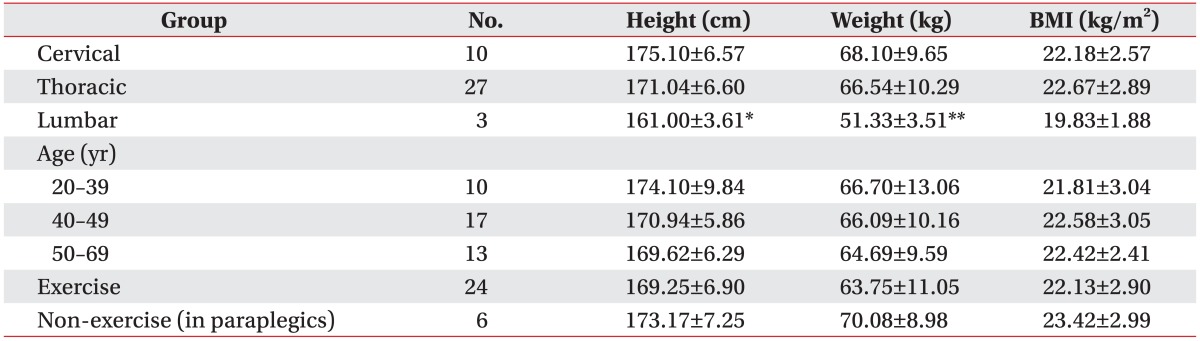
We examined the statistical differences in height, weight, and body mass index (BMI) within each group divided according to SCI level, age, and exercise. As a result, among the groups divided according to the SCI level, the only difference was that the height and weight of the lumbar cord injury group were lower than those of the cervical and thoracic cord injury groups. Otherwise, differences in height, weight, and BMI among the other group were found to have no statistical significance (Table 4).
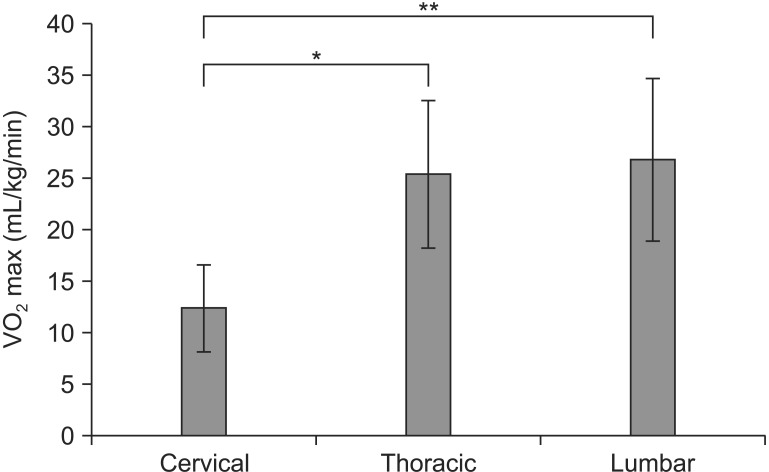
The mean VO2max of all subjects was 22.33±8.68 mL/kg/min. The mean VO2max of the cervical, thoracic and lumbar level injury subjects were 12.45±4.24, 25.47±7.18, and 26.90±7.95 mL/kg/min, respectively (Fig. 2). According to neurologic injury level, individuals with SCI at the thoracic and lumbar level had significantly higher mean VO2max than individuals with cervical SCI.
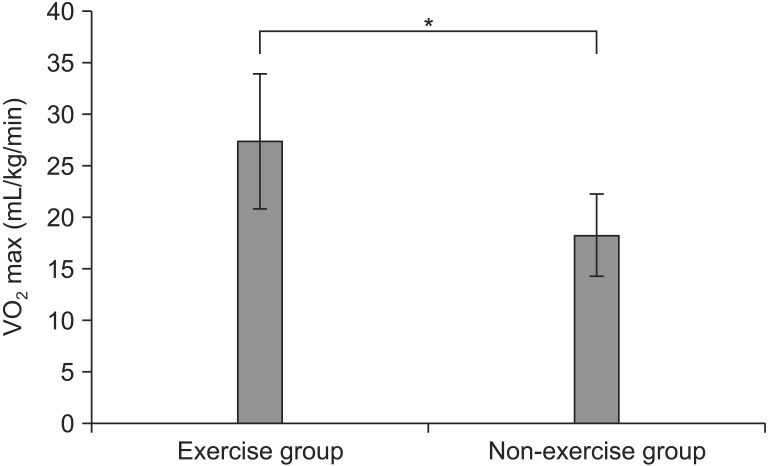
In addition, the mean VO2max of 24 paraplegic subjects who regularly exercised (27.43±6.60 mL/kg/min) was significantly greater than that of the six paraplegic subjects who did not regularly exercise (18.38±3.96 mL/kg/min) (p<0.05) (Fig. 3).
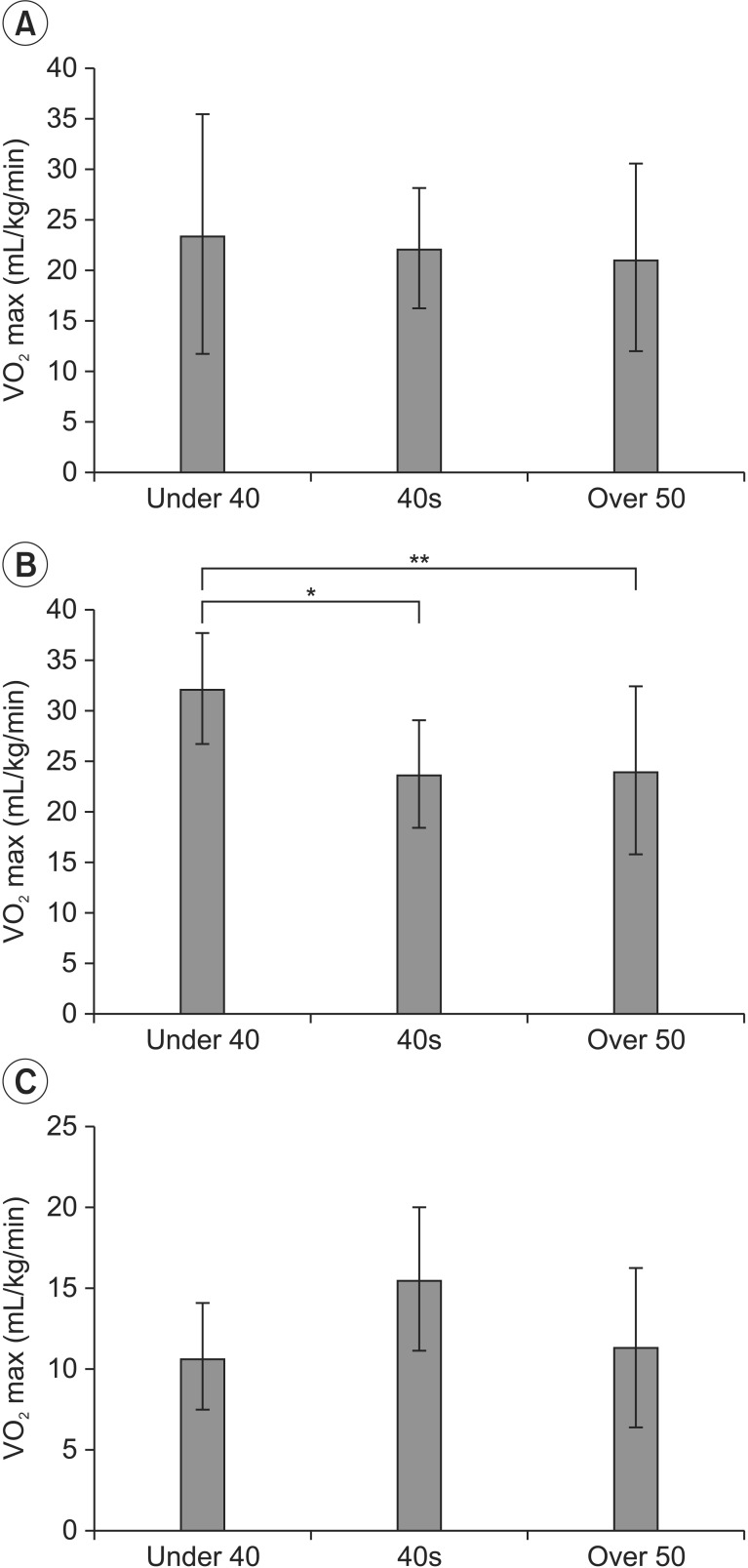
After subdividing the subjects into age groups of under 40, 40-49, and over 50 and disregarding their degree of neurologic damage, their mean VO2max levels were 23.69±11.95, 22.35±5.97, and 21.24±9.33 mL/kg/min, respectively (Fig. 4A).
When classifying the subjects as either tetraplegia or paraplegia depending on the degree of neurologic damage, paraplegic subjects demonstrated higher VO2max (25.62±7.13 mL/kg/min vs. 12.45±4.25 mL/kg/min) (p<0.05).
Meanwhile, the mean maximal oxygen consumption of paraplegic subjects in age groups of under 40, 40s, and 50 and over was 32.25±5.56, 23.79±5.32, and 24.19±8.29 mL/kg/min, respectively. Among the paraplegic subjects, the mean VO2max of those under 40 was higher than those in their 40s or over 50 with statistical significance (p<0.05) (Fig. 4B).
The mean VO2max of tetraplegic subjects in age groups of under 40, 40s, and 50 and over was 10.85±3.30, 15.63±4.37, and 11.40±4.88 mL/kg/min, respectively. In terms of age among the tetraplegics, the mean VO2max in the 40s was the highest compared with other age groups, but without statistical significance (p>0.05) (Fig. 4C).
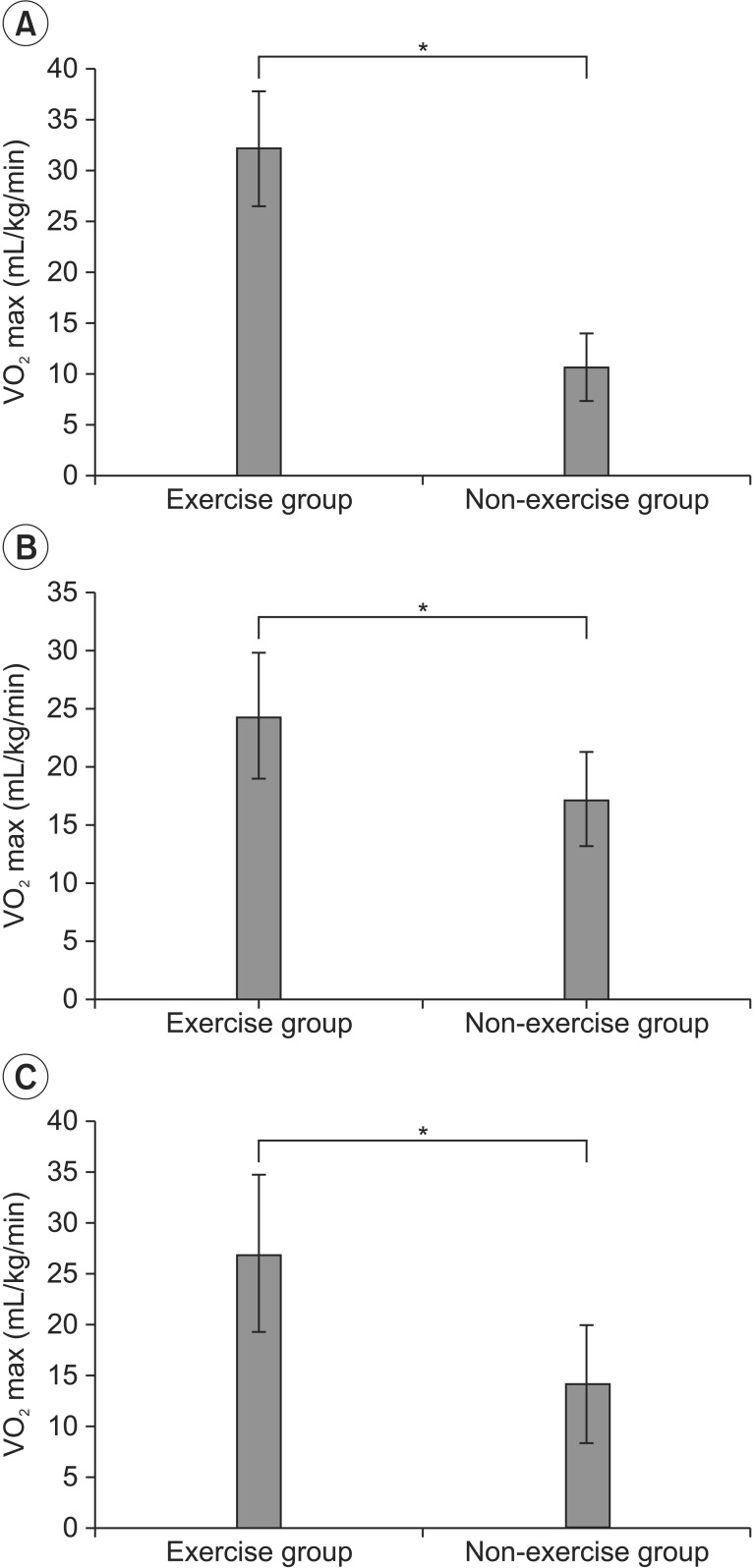
When each age group was further subdivided based on their history of regular exercise, subjects who exercised regularly showed higher VO2max compared to those in the same age group who did not exercise regularly (under 40: 32.25±5.56 mL/kg/min vs. 10.85±3.30 mL/kg/min; 40-49: 24.44±5.45 mL/kg/min vs. 17.34±4.07 mL/kg/min; 50 and over: 27.13±7.67 mL/kg/min vs. 14.37±5.74 mL/kg/min) (p<0.05) (Fig. 5).
DISCUSSION
Aerobic exercise is extremely important in individuals with SCI since it is known to play a major role in preventing a decreasing quality of life and increasing complications which result from a lack of physical activities. Devillard et al. [8] reported that regular exercise directly influences the muscles involved in inspiration of individuals with SCI, and Sutbeyaz et al. [6] demonstrated increased VO2max through regular exercise.
This study used an arm ergometer to directly compare VO2max of male subjects with SCI according to neurologic injury level, age, and history of regular exercise. As a result, this study shows that maximal oxygen consumption rises with lower SCI level and reduces with aging. Among the 40 participants, 25 subjects performed regular daily exercise. These 25 exercised subjects had higher maximal oxygen consumptions compared to the 15 subjects who did not exercise regularly (27.06±6.70 mL/kg/min vs. 14.42±5.05 mL/kg/min).
In this study, the exercise group included the subjects who had been doing regular exercise for at least 6 weeks. This was because, in a review of various studies concerning exercise training programs of individuals with SCI by Devillard et al. [8], 6-week-long training programs were the most common among various exercise durations, ranging from 4 to 36 weeks. Also, the programs were run in various lengths, ranging from 15 to 60 minutes, and therefore, we chose 1 hour as the maximum program length. Retrospectively, most of the subjects categorized as the regular exercise group in our study had been exercising longer than our criteria (for a minimum of 2 years, with each session lasting at least 1 hour).
Significant differences in VO2max were observed after subdividing the 40 subjects according to history of regular exercise; in addition, after subdividing the subjects according to age groups, subjects who exercised regularly showed higher mean VO2max values compared to age group-matched subjects who did not exercise. These findings demonstrate a close relationship between regular exercise and VO2max.
Comparison between paraplegic and tetraplegic subjects showed a significantly higher VO2max in paraplegic groups. This may be due to differences in exercise functional level, as well as due to the effect of cervical level injuries on inspiratory muscles. Among the paraplegic subjects, a general decrease in VO2max was observed in association with progressing age. However, paraplegic subjects under 40 who did not exercise regularly actually demonstrated lower VO2max levels compared to paraplegic subjects in their 50s and above who exercised, which strongly suggests the importance of regular exercise in the improvement of cardiovascular function.
Using our study results, we compared the VO2max between those who exercised and those who did not exercise only within the paraplegic group and not within the tetraplegic group because only one of the 10 tetraplegic subjects with SCI exercised.
The number of tetraplegic subjects was significantly smaller than that of paraplegic subjects in our study. Cardiopulmonary problems occur more frequently with rising neurologic level, leading to complications in the activities of daily living, and its effect on remaining motor function can make arm ergometer exercises difficult to perform in these subjects.
A lower degree of neurologic damage, younger age, and history of regular exercise resulted in higher VO2max levels. It should be noted that the subjects in the over 50s age group who exercised regularly showed higher VO2max compared to non-exercising subjects in the group under 40. This suggests that cardiopulmonary endurance may be maintained and improved with regular exercise, despite the aging process.
Furthermore, the VO2max of the one tetraplegic subject who exercised regularly (despite being a single case) was higher than that of subjects with cervical SCI and was similar to that of paraplegic subjects who did not exercise regularly. Maintaining regular exercise, rather than discontinuing it, may result in improved cardiopulmonary fitness, even in tetraplegic subjects.
The results of healthy male Korean adults in 1993 from the ages 20-29, 30-39, 40-49, and 50s were as follows: 58.4±8.55, 51.8±8.33, 49.0±7.29, and 46.3±7.41, respectively [5]. In our study, the level of mean VO2max for males (22.33±8.68 mL/kg/min) was found to be lower that of the male mean VO2max (51.33±8.77 mL/kg/min) found in a previous study. However, Claydon et al. [9] did a study where individuals with cervical and thoracic SCI had a mean VO2max levels of 14.9±1.1 and 25.2±2.6 mL/kg/min, respectively. These results were not much different compared with the results from our study, which were 12.45±4.24 and 25.47±7.18 mL/kg/min, respectively.
Also, this study shows that the mean VO2max of paraplegics in the exercise group was 27.43±6.60 mL/kg/min, which is the higher than the VO2max of 13.3±4.2 and 9.86±4.21 mL/kg/min shown by the non-exercising paraplegics in Kim and Shin [3] and Sutbeyaz et al. [6], respectively.
In our study, we measured each individual's maximum heart rate, resting blood pressure and heart rate, and blood pressure once every 1 minute over a period of 5 minutes after exercise. The relationship between heart rate max, resting heart rate and VO2max was made by Uth et al. [10]. This relationship was used in our study to predict the VO2max from maximum heart rate and resting heart rate but no correlation was found between the actual VO2max values. These results were probably due to the fact that Uth's equation was based on well-trained healthy subjects while our study was done on subjects with SCI. These differences imply that further studies are needed specifically for patients with SCI.
Meanwhile, although subjects who reported a history of regular exercise demonstrated higher VO2max compared to subjects with similar age or neurologic damage who did not exercise regularly, 'regular exercise' in this study included a wide range of sports activities, such as wheelchair table tennis, wheelchair basketball, ice hockey, weightlifting, badminton, skiing, and wheelchair dance sports. Such a wide range of sports activities led to difficulty in standardizing the degree of regular exercise according to intensity, exercise time, and duration.
Additional limitations of this study were that the number of subjects who exercised regularly was greater than that of those who did not exercise, and that only one of the subjects with a cervical spinal cord injury exercised, causing a significant difference between the groups. On this background, there were some weaknesses in subjects with no regular exercise compared to subjects who perform regular exercise. In further studies, it would be better to add more subjects so that there could be similar amounts of subjects in different groups. This would lead to more exact comparisons and analysis. In addition, it seems that further studies could be done to determine whether different types of physical activities have positive or negative effects on cardiovascular functions of individuals with SCI. Lastly, all subjects were male, and therefore, gender comparison could not be made; future studies should include comparison and analysis on this matter.

 XML Download
XML Download