

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stroke is the most prevalent cause of ambulatory disability and impaired activities of daily living (ADL) [1] Although neurological symptoms after stroke vary according to the location and extent of the brain lesion, motor weakness and sensory and cognitive impairments are the symptoms reported most frequently [2]. Balance control is the ability to maintain body movement within the base of support without falling. It requires integrating sensory input with movement strategies, appropriate latencies of postural responses, and the ability to plan and execute movement patterns necessary for controlling the center of body mass [1,3,4]. As such, balance control is influenced by cognitive factors, such as attention, motivation, and intent. Impaired postural control is caused by a complex interplay of motor, sensory, and cognitive impairments, and is a key characteristic of mobility problems in patients with stroke [5].
The dual-task paradigm provides information on the automaticity, hemispheric locus, and structural independence of processes hypothesized to underlie the production of skilled performance [6]. This experimental approach involves two tasks performed simultaneously (dual task). The dual task is divided into primary and secondary tasks. The performance of the primary task is maintained at the baseline (single task) level during the dual-task condition. If performance of the secondary task is reduced from the baseline level under the dualtask condition, this reflects high attentional demands of the primary task and suggests insufficient reserve capacity to perform the secondary task at the baseline level [7]. For example, mobility in daily life may require walking while talking with a friend or drinking coffee, and gait speed and balance control decrease during this dual task relative to walking without talking or drinking. Although healthy control subjects have no difficulty maintaining walking speed while simultaneously performing another task, elderly individuals and individuals with a brain lesion or a degenerative movement disease, such as Parkinson disease, have impaired balance control. The dualtask paradigm is the primary approach used to study interactions between cognitive processing and motor behavior [8].
Many studies have reported that a dual task affects gait or interactions between cognitive tasks and gait or balance. However, most studies have focused on the effect of a cognitive task on gait or locomotion [7,8,9,10,11,12,13,14]. Only one study has reported that a dual-task intervention improved walking ability in subjects with chronic stroke [15], and no studies are available on the interactions between balance and cognitive tasks after dual-task training in patients with a subacute stroke. Therefore, this study was undertaken to investigate the effectiveness of dual-taskbased rehabilitation on balance and cognition in patients with subacute stroke.
MATERIALS AND METHODS
Participants
patients (12 males and eight females; average age, 59.7±12.1 years) with subacute (i.e., within 3 months) stroke participated in this study The patients were recruited following attendance at the Department of Physical Medicine and Rehabilitation in our hospital between July 2012 and July 2013 for a first-ever cerebral stroke involving the cortical or subcortical area. Their diagnosis was confirmed clinically through computed tomography scans or magnetic resonance imaging. Inclusion criteria were the ability to stand for at least 1 minute without assistance and the ability to understand simple oral instructions given by a physical therapist. Exclusion criteria were the presence of a previous symptomatic stroke, visual field defect, hemispatial neglect, severe cognitive impairment or aphasia (determined by a clinical evaluation with a physiatrist), psychological disorder, and uncontrolled medical disease or significant orthopedic pain or pain that limited participation in balance testing. This protocol was reviewed and approved by the Institutional Review Board, and all participants provided written informed consent before the selection procedure.
Interventions
This was a single-blind study, and participants were randomly allocated to the dual-task group (n=10) or the control group (n=10). Both groups received one session of conventional physical therapy for 30 minutes per day, 5 days per week, for 4 weeks. Additionally, the dual-task group received dual-task training using BioRescue (RM Ingenierie, Rodez, France), and the control group received balance training using a balance board for 30 minutes per day, 5 days per week. Both interventions were delivered five times per week for 4 weeks. Thus, all participants were treated with conventional physical therapy and balance training of the same amount and duration. A subset of participants also received computer-based cognitive therapy (CBT) twice per week for 4 weeks (n=4 participants in the dual-task group and n=5 participants in the control group). No significant difference was observed between the groups in the number of participants who received CBT.
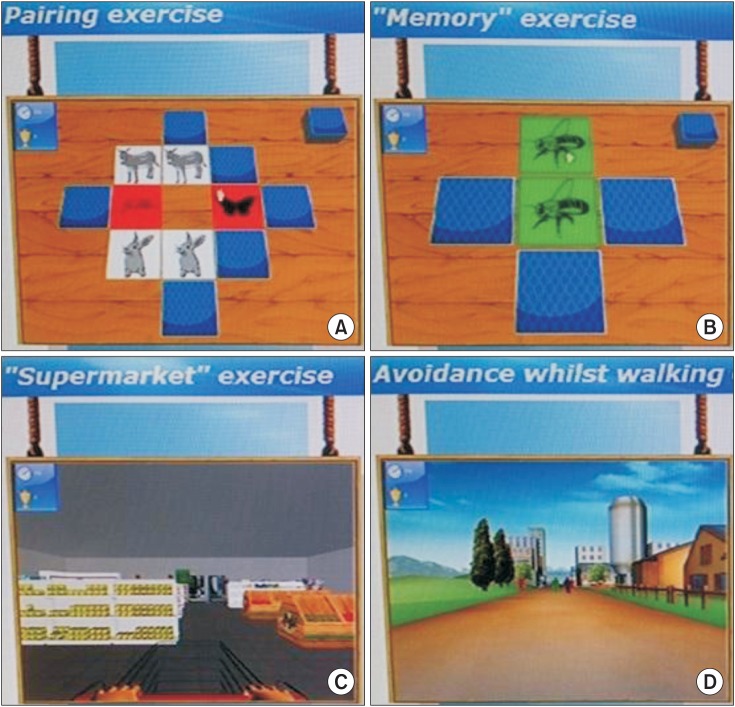
Dual-task training and conventional balance training were offered by one physical therapist. Participants involved in the dual-task training using BioRescue stood on a platform located 1.0-1.5 m away from a monitor. Balance tasks were presented on the monitor, and the system monitored the motion of the participant using sensors connected to the platform. Four tasks were used pairs, memory, supermarket, and avoidance while walking (Fig. 1A-D). The pairs task required the participant to match the same two cards on reversed cards by moving a cursor on the monitor using body weight shifts on the platform. At the beginning of the training, six pairs of cards were shown on the monitor. This number was progressively increased to 24 pairs of cards. The memory task required the participant to identify the card on the center of the monitor among the four different side (anterior, posterior, left, right) cards after it appeared and disappeared for 8 seconds. Participants were required to identify the card shown by moving a cursor on the monitor using body weight shifts. Participants involved in the supermarket task memorized a grocery shopping list and shifted their body weight to choose goods and place them in a basket. Participant involved in the avoidance while walking task were required to walk through a street without touching barriers. All four tasks were used in each dual-task training session and were correctly set up depending on the patient's condition. Each task was performed for 6 minutes, and the participant rested 2 minutes between tasks. The control group received balance training with a balance board.
Outcome measures
Balance, cognitive function, motor function, and functional status for ADL were evaluated at baseline and after the 4-week intervention.
Balance
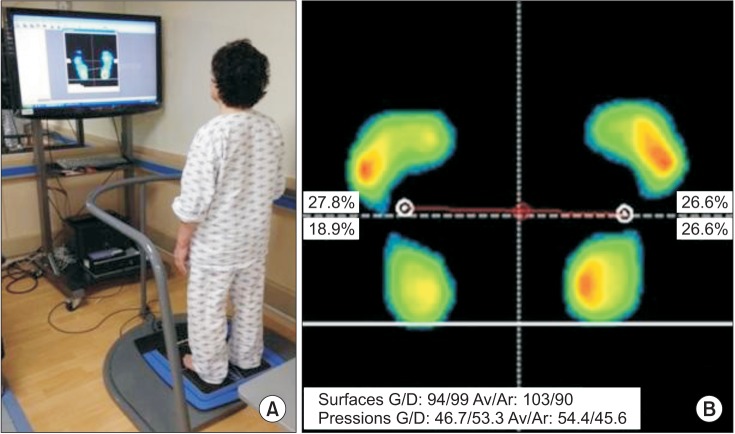
Balance was assessed using BioRescue static posturography and the Berg Balance Scale (BBS). BioRescue includes a platform (610×580×10 mm3) equipped with 1,600 pressure sensors that measure vertical pressure fluctuations in both feet. The force movements of the foot reflect fluctuations in the foot center of pressure (COP). For all balance tests, participants stood barefoot on the platform without holding the support bar, and the data were checked, amplified, and filtered before analysis (Fig. 2A, B).
Balance was quantified using weight distribution indices (WDI) and stability indices. The WDI quantified were weight distribution index-surface area (WDI-Sa) and weight distribution index-pressure (WDI-Pr). Participants were instructed to stand without assistance for 30 seconds, and the WDI were quantified. These parameters quantified the ratio of weight distribution on the hemiparetic and intact sides. A ratio of 1.00 indicates equal weight placed on each side and is considered ideal. Most patients who have suffered a stroke have reduced loading on the paretic side [5], resulting in WDI <1.00. A WDI closer to 1.00 indicates better balance. WDI were evaluated while participants stood under eyes-open (EO) and eyes-closed (EC) conditions.
The stability indices quantified were the static stability index and the dynamic stability index. The static stability indices quantified were stability index-surface area (SI-Sa) and stability index-length (SI-L). Participants were instructed to stand in the reference position, with their gaze fixed in the normal plane of vision for 30 seconds. The COP under each foot was measured continuously for 30 seconds. SI-Sa and SI-L indicate horizontal and vertical sway of the COP and were evaluated while participants stood with EO and EC. The higher the index score, the more unstable the posture. Participants assessed for the dynamic stability index were instructed to move an arrow on the monitor by shifting their body weight and to stabilize themselves as far as possible from their original position and remain in that position for as long as the arrow remained on the screen. When the arrow disappeared, the participant was instructed to return to the original position. The limit of stability (LOS) was measured and expressed as surface area per side (LOS-Sa) and the area ratio (LOS-Ar). LOS-Sa was quantified in four directions (left, right, forward, and back), and LOS-Ar was quantified for left/right and front/back. LOS-Sa left and LOS-Sa right were expressed as LOS-Sa hemiparetic and LOS-Sa intact, as appropriate, and LOS-Ar left/right was expressed as LOS-Ar hemiparetic/intact. A LOS-Sa of 1.00 indicated that the dynamic balance was equal on both sides, and a LOS-Sa close to 1.00 indicated improved dynamic balance. Balance was also evaluated using the BBS, which is a validated and widely used clinical test of static and dynamic balance [16]. Participants performed 14 functional tasks and received a score of 0-4 points for each task. Therefore, a total score was 0-56 points, with higher scores indicating greater balance and functional independence with respect to the activities tested. The Korean version of the BBS has been validated [17].
Cognitive function
Cognitive function was evaluated using the Korean version of the Mini-Mental State Examination (K-MMSE) [18] and a computerized neuropsychological test (CNT; MaxMedica Inc., Seoul, Korea) [19]. Visual and auditory continuous performance tests were used to evaluate continuous concentration on visual and auditory stimuli, the word-color test was used to evaluate selective attention, and the forward and backward digit span test and the verbal learning test were used to evaluate verbal memory. Participants involved in the verbal learning test listened to 15 target words through a speaker and were scored on the number of words they first recalled, the number of words they recalled after repeating the same target word five times, the number of words they recalled after 20 minutes, and the number of words they found after presenting a list of 30 words containing the previous 15 words on the screen. Forward and backward visual span tests and visual learning tests were performed for the spatial memory test. Participants involved in the visual learning test were shown 15 different target figures, and were then shown 30 figures (the 15 target figures and 15 non-target figures) and asked to identify the target figures. We scored the number of presented figures they first identified, the number of figures they identified after being shown the target figures five times, the number of figures they identified after 20 minutes, and the number of figures they identified after being shown all 30 figures on the screen. For the visual motor coordination test (Trail Making Test-type A), we evaluated the time taken to draw lines connecting 25 small circles on the screen. The circles contained the numbers 1-25, and participants were required to connect the circles in numerical order.
Motor function
Motor function was evaluated using the Fugl-Meyer Assessment (FMA). The FMA is a stroke-specific, performance-based impairment index designed to assess motor function, balance, sensation, joint function, and pain in patients with post-stroke hemiplegia. It consists of 155 items, and each item is rated on a 3-point ordinal scale (0, cannot perform; 1, can perform partially; and 2, can perform fully). The motor domain includes items that assess movement, coordination, and reflexes and is divided into 66 points for the upper extremities and 34 points for the lower extremities. In this study, we used the lower-extremity hemiparetic side FMA score to evaluate motor function.
Functional status for ADL
Functional status for ADL was evaluated using the Korean version of the Modified Barthel Index (MBI) [20]. The MBI is a reliable and valid instrument for measuring the functional status of patients with stroke and shows the degree of independence of a patient from any assistance.
Statistical analysis
All statistical analyses were performed using SPSS for Windows ver. 20.0 (IBM SPSS Inc., Armonk, NY, USA). Baseline demographic and clinical characteristics were compared between the dual-task and control groups using independent sample t-tests for continuous data and chi-square tests for categorical data. The change in a variable from pre- to post-training was evaluated in each group using the Wilcoxon signed-rank test. Changes preto post-training were compared between the groups using the Mann-Whitney test. A p-value<0.05 was considered significant.
RESULTS
Demographic and clinical characteristics
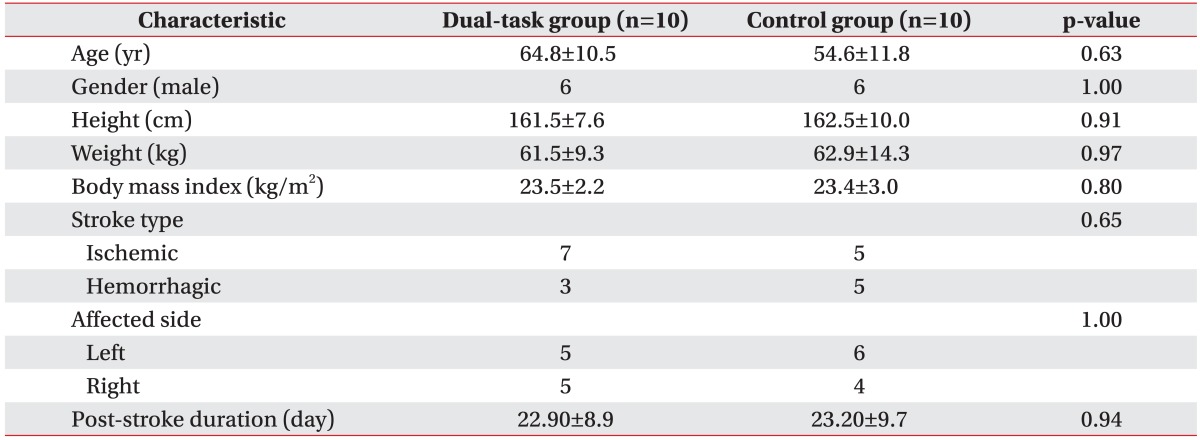
Baseline demographic characteristics and stroke-related data are presented in Table 1. Twenty-one eligible participants were recruited. One participant dropped out because of another medical condition. Thus, 20 participants (12 males and eight females) completed this study. The average ages in the dual-task and control groups were 64.8±10.5 years and 54.6±11.8 years, respectively. The average durations from stroke onset to the time of the first evaluation were 22.90±8.9 days and 23.20±9.7 days, respectively. Demographic characteristics including sex, age, body mass index, stroke type (ischemic or hemorrhagic), affected side (right or left), and the duration from stroke to the first evaluation were not different between the groups. No participant in either group experienced a serious adverse event during the study period.
Comparison of balance ability, cognitive, motor, and ADL functions within each group
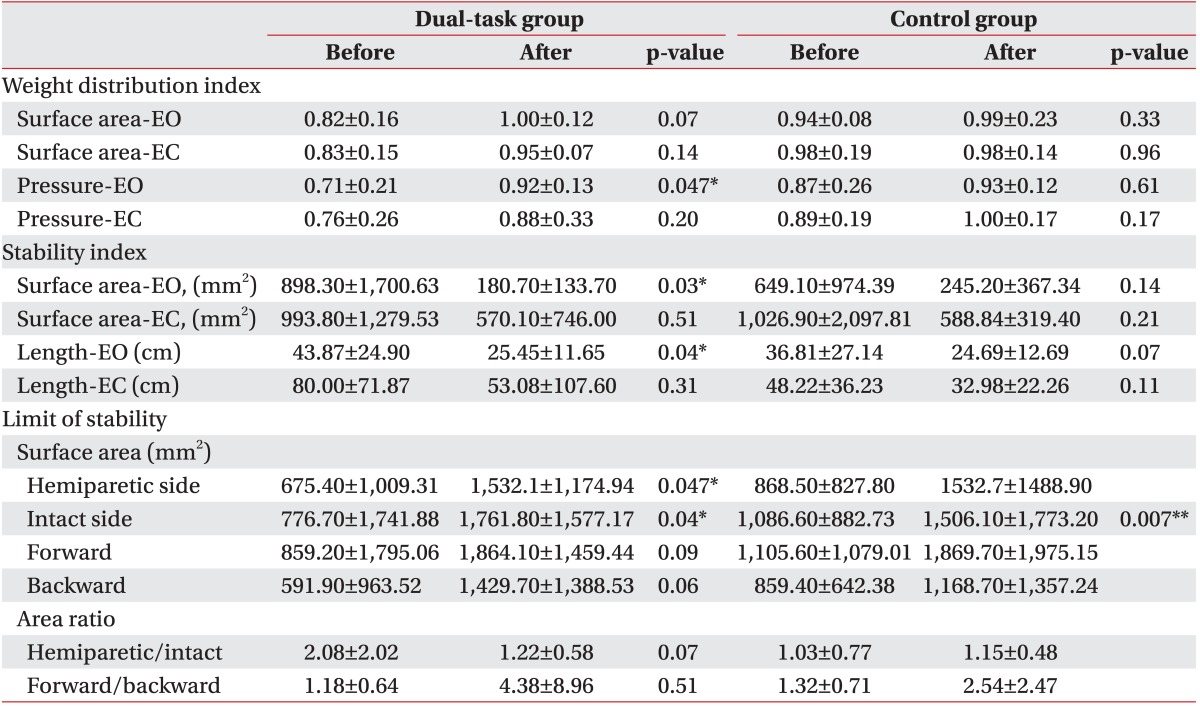
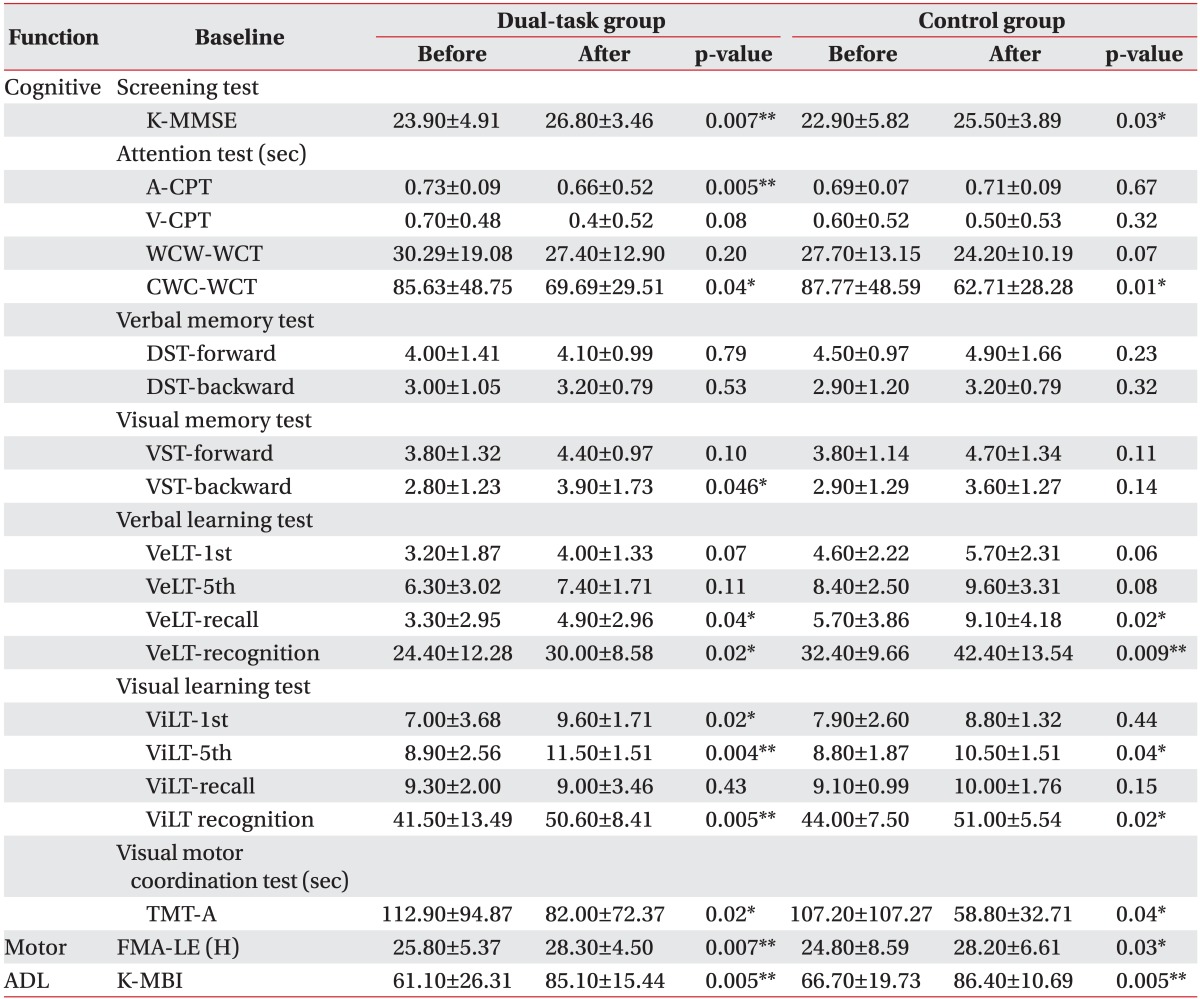
The dual-task group showed significant improvements in balance ability on the WDI-Pr during EO (from 0.71±0.21 to 0.92±0.13; p=0.047), LOS-Sa on the hemiparetic (from 675.40±1,009.31 to 1,532.1±1,174.94 mm2; p=0.047) and intact (from 776.70±1,741.88 to 1,761.80±1,577.17 mm2; p=0.04) sides, and SI-Sa (from 898.30±1,700.63 to 180.7±133.70 mm2; p=0.03) and SI-L (from 43.87±24.90 to 25.45±11.65 cm; p=0.04) during EO. The parameters of cognitive function, such as auditory CPT (from 0.73±0.09 to 0.66±0.52 seconds; p=0.005) and backward VST (from 2.80±1.23 to 3.90±1.73; p=0.046), improved significantly in the dual-task group after treatment compared with those before treatment. The BBS, verbal and visual learning tests, WCT, TMT-A, K-MMSE, FMA, and K-MBI improved significantly in both groups after treatment (Tables 2, 3).
Comparison of changes in balance ability and cognitive, motor, ADL functions between the dual-task and control groups
WDI-Pr (0.21±0.27 vs. 0.06±0.24; p=0.05) and LOS-Ar (hemiparetic/intact) (-0.86±1.89 vs. 0.12±0.75; p=0.09) during EO tended to improve more in the dual-task group than those in the control group. However, no significant differences in the changes in balance ability, cognitive, and motor function were observed between the groups. No difference was observed in functional independence between the groups.
DISCUSSION
In this study, we showed that dual-task training focusing on balance and cognitive tasks may improve balance and cognitive functions compared with those after conventional balance training in patients with subacute stroke.
The improved WDI-Pr during EO from pre- to post-training indicates more equal weight distribution on the two sides of the body. Improvements in the WDI-Pr and dynamic stability parameters, such as LOS-Sa for the hemiparetic and intact sides, were observed only in the dual-task group. This result indicates that patients in the dual-task group improved their ability to displace COP, whereas control patients did not. The ability to voluntarily move COP to positions within the LOS is fundamental to mobility tasks, such as reaching for objects, transitioning from a seated to a standing position, and walking. These results suggest that patients in the dual-task group reduced their risk of falling or becoming unstable during activities that required weight shifts. In addition, significant decreases in SI-Sa and SI-L during EO were observed only in the dual-task group. Sway area and sway length are generally assessed as the amount of COP displaced during steady standing and represent steadiness and postural control [21,22].
Our results suggest that dual-task training focusing on balance and cognitive tasks positively affected dynamic and static balance.
There are several possible explanations for our findings. The dual-task training included visual feedback of balance control. Lee et al. [23] reported that visual feedback training improves sitting balance and visual perception in patients with chronic stroke. In addition, the dualtask training we provided was task oriented and of high intensity. A Cochrane review reported that repetitive task training improves lower limb function [24]; however, there is a lack of evidence for improved balance control after task-oriented repetitive training [25]. Our interventions differed from those in the abovementioned studies, as they focused on balance and repetitive task-oriented training, whereas the other studies focused on just taskoriented training [24,25]. Bensoussan et al. [26] and Marshall et al. [27] reported that attention deficits cause postural instability. A dual-task paradigm involves interactions between cognitive function and motor behaviors, so an improvement in attention with training could affect balance. Previous studies have included participants with a relatively high BBS score at baseline, which may have prevented any improvement in balance from being detected using the BBS. Our results demonstrate that balance evaluated using posturography and the BBS was not different between the groups. However, some measures of static and dynamic balance obtained from posturography improved significantly from pre- to post-training in the dual-task group but not in the control group. The WDI-Pr during EO and LOS-Ar (hemiparetic/intact) showed a tendency to improve in the dual-task group but not in the control group, suggesting that the posturography measures were more sensitive to changes in balance than those of the BBS.
We found that auditory attention and short-term visuospatial memory improved significantly from pre- to posttraining in the dual-task group but not in the control group. Ben-Yishay et al. [28] reported that intact attention is required for effective use of higher cognitive functions, and if the ability to pay attention and concentrate is impaired, there may be associated impairments in memory, problem solving, and producing appropriate actions. In our study, participants were placed under the abovementioned conditions, so the improvement in auditory attention after training was remarkable. Other parameters improved with similar patterns after the interventions. A possible explanation for these findings is that the dual task required a high degree of attention. Participants were required to control their balance simultaneously while performing other non-balance-related tasks and needed to pay continuous attention to both tasks. Lee et al. [29] reported that performing a dual task decreases postural stability and attention. However, the authors did not examine the effect of training using a dual task, and only tested performance at one time point. Thus, the surroundings requiring attention is an essential element of dual-task training. Community-dwelling patients with stroke are at higher risk for falls than those in the general population [30], and attention deficits are common among these patients [31,32].
Therefore, cognitive therapy is important to reduce fall risk. Although patients with stroke have complex impairments involving cognitive, sensory, and motor functions, they receive therapies focused on a single aspect at a time. For example, a physical therapist provides treatment for motor impairments or poor balance control, whereas an occupational therapist provides cognitive oriented therapy. However, many tasks in a community setting require an interplay of motor, sensory, and cognitive functions. The interventions that we provided to the dual-task group in this study helped patients with stroke adapt to the real-world environment. Therefore, our findings that dual-task training focusing on balance control and cognitive function improved balance and cognitive function have important clinical implications and suggest that this type of dual-task training might be helpful for reducing fall risk and helping patients with stroke adapt to new surroundings.
There are some limitations to our study. First, the sample size in each group was small. Future studies with more participants are warranted to confirm our findings and reveal differences between the two interventions. Second, intervention duration was short, and we did not observe long-term follow-up; therefore, we cannot comment on the long-term effect of the dual-task training on balance and cognition.
In conclusion, we demonstrated that 4 weeks of dualtask training had modest effects on balance and cognitive function compared with 4 weeks of conventional balance training in patients with subacute stroke. These findings suggest that dual-task training could be as effective as conventional balance training for improving balance and cognition in subacute post-stroke patients.
 XML Download
XML Download