

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since the pronator teres (PT) muscle is innervated by the median nerve from the lateral cords of the brachial plexus, originating from the ventral roots of C6 and C7, needle electromyography of this muscle is useful for evaluating brachial plexopathy, cervical radiculopathy, median neuropathy, or anterior interosseous nerve syndrome.
The identification of an optimal needle electrode insertion point is important for obtaining optimal motor unit action potentials and minimizing patient discomfort and complications. The commonly used method of needle electrode insertion is inserting the needle two fingerbreadths distal to the mid-point between the biceps tendon and medial epicondyle with the forearm supinated [1,2].
Electrodiagnostic procedures are generally well tolerated and rarely thought to be associated with any significant complications. However, there can be iatrogenic complications, including bleeding, infection, and nerve damage from the procedure [3]. Needle insertion for needle electromyography of the PT muscle requires more caution because the median nerve and brachial or ulnar artery are close to the PT muscle. In addition, if the needle is inserted too medially, it may reach other muscles such as the flexor carpi radialis [4]. Thus, a reliable and safe technique for inserting a needle electrode into the PT muscle has to be explored in order to prevent serious neurovascular complications. The aim of this study is to provide an accurate and safe approach to needle insertion through identifying the anatomical relationship between the common needle electrode insertion site of the PT muscle and the neurovascular bundle using ultrasonography, and to suggest an optimal needle insertion location.
MATERIALS AND METHODS
The study group was composed of 13 men and 12 women, with a mean (±standard deviation) age of 31.7 (±10.0) years. The 25 volunteers had no history of neuromuscular disease, exhibited normative findings in a neurologic examination, and were currently not taking any medication. Assessments were taken on both forearms for all subjects, thus, there were 50 forearms were measured in total. This study protocol was approved by the Institutional Review Board. All subject participated voluntarily in this study and consent forms were signed by each of them.
Height, weight, and circumference and length of both forearms were measured. The forearm circumference was measured at 3.5 cm distal to the elbow crease. The length of the forearm was defined as the distance from the ulnar styloid process to the olecranon with the forearm supinated and the elbow at 90° in a supine position.
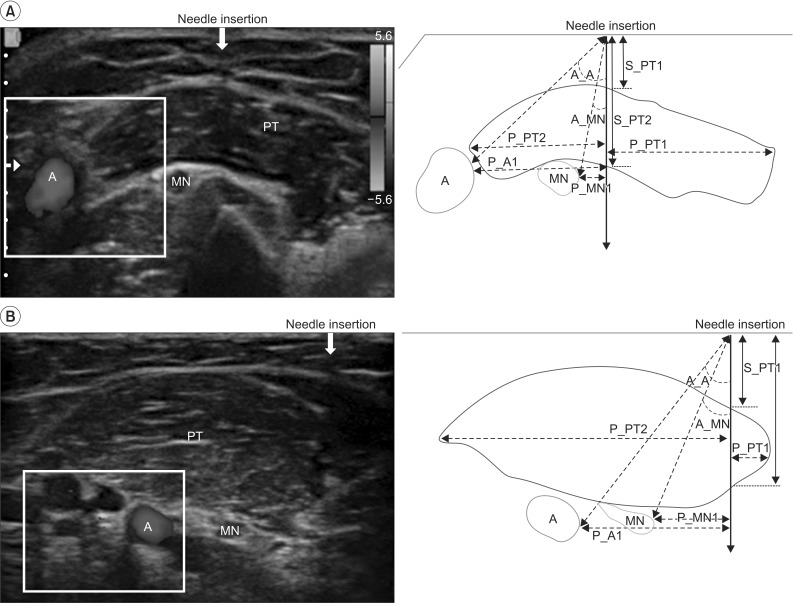
The mid-point between the biceps tendon and medial epicondyle at the elbow crease was marked with a pen. For the landmark of ultrasonographic evaluation, an epidural needle (22-guage, 80 mm long) with the needle-tip broken off was placed to the marked point parallel to the medial side of forearm (Fig. 1).
Ultrasonographic scanning was done at four points-the marked point in the elbow crease (point 0), 2 cm distal to point 0 (point 1), 3.5 cm distal to point 0 (point 2), and 5 cm distal to point 0 (point 3). Although one finger breadth is defined as 3/4 inch, which is about 1.9 cm [5], we assumed two fingerbreadths to be 3.5 cm. A high-resolution, real-time ultrasonography was performed by an expert physiatrist using the Accuvix V20 system (Samsung Medison, Seoul, Korea) interfaced with a 5-13 MHz linear array transducer. Ultrasonographic examinations of the PT muscle were performed in a transverse view with subjects in a supine position with their elbows fully extended and forearms supinated.
At each point of scanning, the distance between each point and upper margin of PT (S_PT1), the distance between each point and lower margin of PT (S_PT2), the distance between vertical line of each point and medial margin of PT and lateral margin of PT (P_PT1 and P_PT2, respectively), the distance between vertical line of each point and medial margin of brachial or ulnar artery and median nerve (P_A and P_MN, respectively), and the angle between the vertical line of the each point and medial border of ulnar or brachial artery and median nerve (A_ A and A_MN) were measured. If the medial end of the PT was located lateral to the vertical line of each point, the P_PT1 was recorded as a negative value (-) (Fig. 2). We assumed that the thickness of the PT at each point and the horizontal distances from the vertical line of each point to the medial margin of PT were significant parameters for deciding the ideal needle insertion point by ultrasonography.
All statistical analyses were performed with the SPSS ver. 20.0 (IBM SPSS Inc., Armonk, NY, USA). The independent t-test was performed to compare the height, weight, circumference and length of forearms between men and women. The measured distance and angle of artery and nerve at points 0, 1, 2, and 3 were compared using an analysis of variance for repeated measurements and Bonferroni adjustment. In order to test whether the sphericity assumption was accurate, we also ran a Mauchly sphericity test. If the sphericity assumption was violated (p<0.05), the Greenhouse-Geisser correction was performed to estimate the p-value. Also, if it was not violated, we used the exact p-values. The p-values under 0.05 were considered as statistically significant.
RESULTS
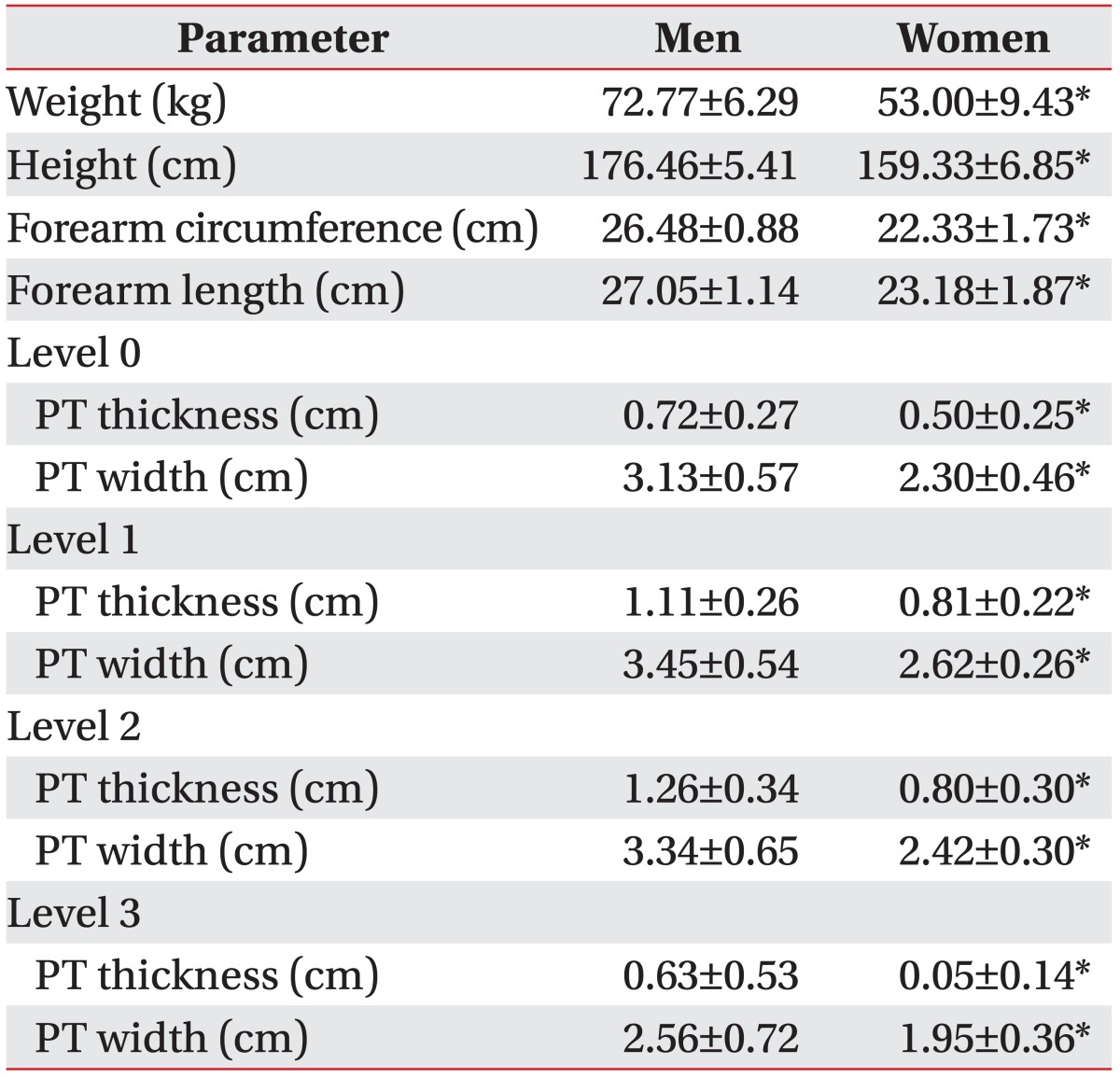
The mean±standard deviation of weight, height, and circumference and length of the forearm were 63.28± 12.78 kg, 168.24±10.61 cm, 24.53±2.49 cm, and 25.19±2.49 cm, respectively. There was a significant difference between the results obtained from men and women (Table 1).
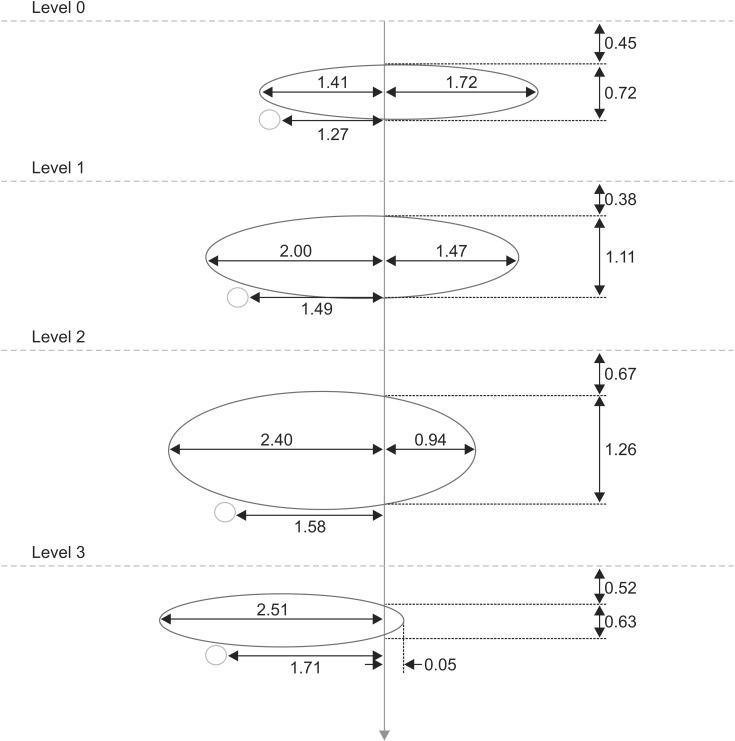
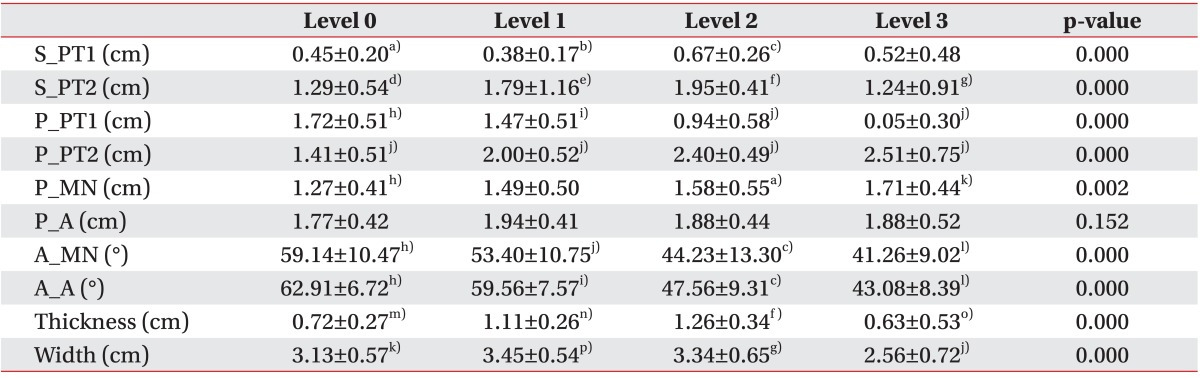
In men, the muscle was thickest at point 2 and showed a statistically significant difference with points 0 and 3 but not with point 1. The distance between the vertical line from each point and medial margin of PT was longest at point 1 and showed a significant difference with points 2 and 3. The minimum value of P_PT1 was 0.96 cm at point 1 and 0.36 cm at point 2 (Table 2, Fig. 3). P_MN was longer at point 2 than at point 1, and P_A was longer at point 1 than at point 2. However, P_MN and P_A at point 1 did not show any statistically significant difference with point 2. P_A was longer than P_MN at all points.
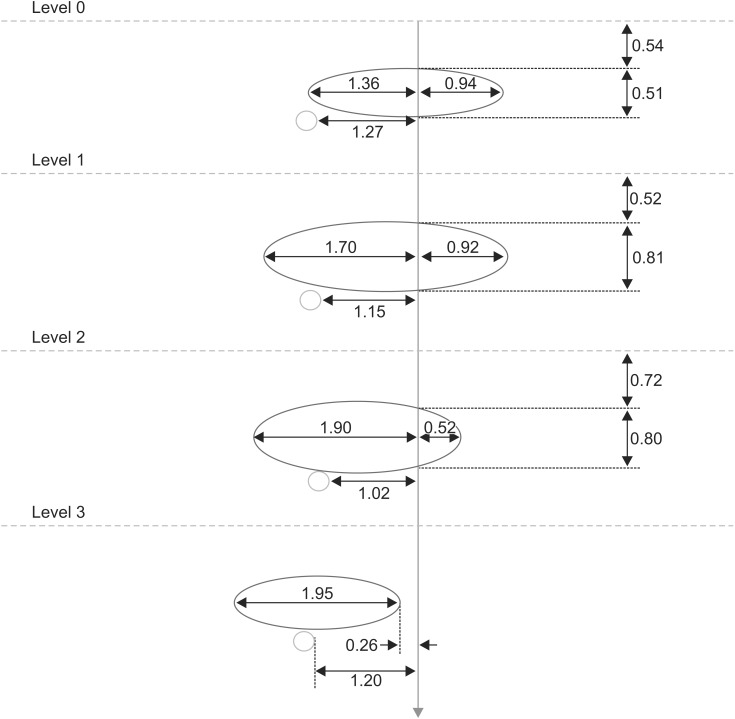
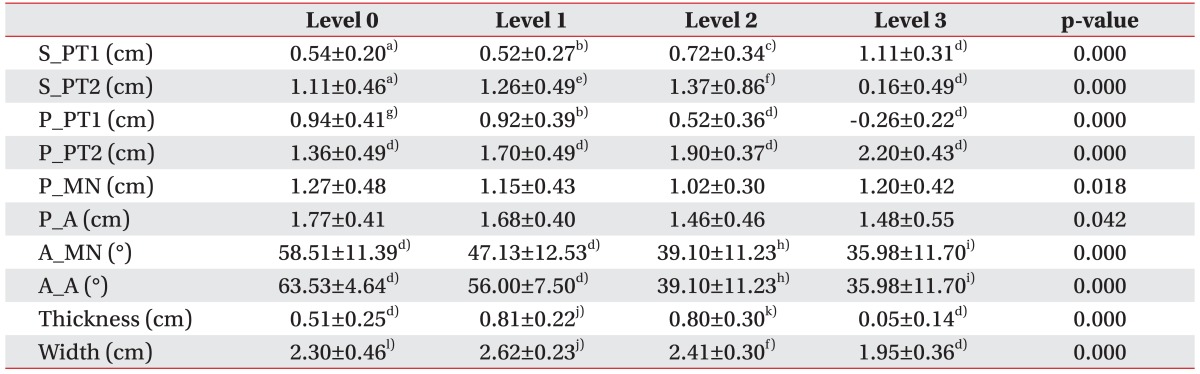
In women, the muscle was thickest at point 1 and showed a statistically significant difference with points 0 and 3 but not with point 2. The distance between a vertical line from each point and the medial margin of the PT muscle was longest at point 1, which was significantly different from points 2 and 3. The minimum value of P_PT1 was 0.53 cm at point 1 and 0.16 cm at point 2. At point 3, the P_PT1 was measured to be a negative value since the vertical line and the PT muscle did not overlap (Table 3, Fig. 4). P_MN and P_A at point 1 were longer than at point 2. P_MN and P_A at point 1 did not have a statistically significant difference with point 2. Also, as in men, the P_A was longer than P_MN at all points. Therefore, a vertical line was closer to the median nerve than the ulnar artery.
DISCUSSION
Despite variations in the muscular branches of the median nerve [6], the nerve usually arises from the cubital fossa and gives off a branch to PT muscle before entering between the two heads of the PT muscle. There are also variations in the course of the brachial or ulnar artery [7]. In general, the brachial artery divides into the radial and ulnar arteries proximal to the PT muscle, and ulnar artery passes obliquely downward, seated deeply, and covered by the PT [8].
Through the development of ultrasound resolution, the relative anatomical position of the neurovascular structures (the median nerve and brachial or ulnar arteries) to the PT has become identifiable.
There have been several articles regarding the evaluation of needle electrode insertion sites using ultrasonography [9,10,11]. However, there have been no studies regarding an insertion site for the PT. To our knowledge, this is the first study to establish an accurate and safe approach to needle electromyography of the PT muscle using ultrasonographic study.
In order to avoid the median nerve and brachial or ulnar artery, it is safest to insert the needle medial to the vertical line and where the muscle is thick enough. Thus, the level with the longest distance between a vertical line and medial margin of PT and the thickness of the muscle were considered to be the optimal level.
In the case of men, there was no significant difference between muscle thickness at points 1 and 2. The muscle was thickest at point 2 and the distance from the muscle to the median nerve was 1 cm at its shortest, which could lead to possible nerve injury when the needle is inserted laterally. The distance between the expected needle insertion line and the medial margin of the muscle was longest at point 1, and this was significantly different from point 2. In women, on the other hand, the muscle was thickest at point 1 but the difference between it and point 2 was only 0.01 cm on average, which was not significant. The distance between the needle insertion line and the medial margin of the muscle was the longest at point 1, which was same as in men, and this was significantly different from point 2. At point 3, the needle did not meet the muscle in women. The difference between men and women seems to be due to difference in the length of their respective forearms.
According to this study's results, both men and women had neurovascular bundles located lateral to the needle insertion line. Among the bundle, the medial placement of median nerve compared to the artery was prominent, which indicates higher risk of injury to the nerve than the vessels when the needle in inserted laterally.
Therefore, in order to prevent nerve injury, it is recommended that the needle be inserted 2-3.5 cm distal to the mid-point between the biceps tendon and medial epicondyle in the elbow crease, and the needle should be advanced in the direction distal 2 cm toward the elbow crease and medially, within 1 cm in men and 0.5 cm in women, to prevent from inserting into inappropriate muscle. The direction for needle exploration is a concordant result to a previous cadaver study [12]. Widely used methods for the electromyography of PT muscle were insertion of a needle electrode two fingerbreadths distal to the midpoint of the medial epicondyle and the tendon of biceps brachii muscle [1,2] or 2.5 cm distal to the elbow crease in the same direction as the PT muscle [13], or 5 cm distal to the midpoint of the elbow crease [14], irrespective of the gender. This study provides not only the safe needle insertion point for the PT muscle, but also different range for needle exploration in each gender.
This study has several potential limitations. The first limitation is the quantity of subjects. Second, in the ultrasound image, we assumed the posterior acoustic shadowing of a broken needle on the skin as a needle insertion line instead of inserting a real needle. Third, because the linear probe has difficulty conforming to the curvature of the forearm without compression, such irregular compression of a probe can induce measurement errors. In order to reduce such errors, many trials such as using a water tank to use water as a transmission medium to free the probe from compression have been done [9]. In this study, the use of a water tank was limited due to the position of the arm, which was in full extension. Instead, we used abundant amount of gel in order to minimize probe compression and thus minimize the migration or change to the inner structures. Lastly, only healthy people were included in this study. Patients with C7 radiculopathy or other diseases, such as median neuropathy, will have different results due to muscle atrophy. Thus, further study needs to be done including such patients.
In conclusion, for needle electrode insertion into the PT, ultrasound imaging allows a more accurate and safe approach. The results of this study prove that the most appropriate and safe needle insertion site to the PT is distal 2-3.5 cm to the mid-point between the biceps tendon and medial epicondyle in the elbow crease. Once the needle is inserted perpendicular to the skin's surface at the above site until the needle reaches the PT, the needle must be advanced to the proximal and medial side within 1 cm in men and 0.5 cm in women, to avoid median nerve or ulnar artery injury.

 XML Download
XML Download