

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stroke is a leading cause of serious long-term disabilities like hemiparesis, cognitive impairment, and speech disorder. Among those, hemiparesis is the most frequent and the most disabling problem which leads to an incomplete recovery in the most of cases [1]. Therefore, an accurate measurement of motor functions is very important to provide useful information about the current status and for the optimization of rehabilitation interventions. Many studies were already conducted for an outcome prediction of motor weakness using various objective tools, including radiologic [2], electrophysiological [3,4], and functional neuroimaging methods [5,6].
The motor evoked potential (MEP) is the standard measure of motor response to the transcranial magnetic stimulation (TMS). This test provides in a safe and painless way information about the physiologic integrity of the corticospinal pathway from the primary motor cortex to the spinal motor neurons and also to the electrical potential in individual muscles [7]. In many previous studies where MEP was used a better functional recovery prognosis was shown for those patients with a present MEP than for those patients with an absent MEP [4,8-10]. Some studies have also shown the amplitude of MEP could be an effective parameter [11,12]. However, in other studies the inconsistency of amplitude value which varies across individuals and environments was emphasized [13,14]. Therefore, the use of an amplitude ratio by comparing MEP amplitudes obtained from both hemispheres may be more helpful. Also the amplitude ratio showed a significant correlation with the hand function in a previous study [15]. However, there is only a small number of studies yet where the role of amplitude ratio in the motor function assessment was highlighted. So further studies are needed to confirm those suggested correlations.
The diffusion tensor tractography (DTT), derived from the diffusion tensor imaging (DTI), is a newly developed magnetic resonance imaging (MRI) technique. DTT provides the visualization and evaluation of the corticospinal tract (CST) orientation and integrity [16-18]. The predictive value of DTT for the motor outcome in stroke patients was proved in several studies [19-22]. The combined tests of TMS and DTT also showed their usefulness in the prediction of motor outcome in stroke patients [23,24]. However, further studies involving more parameters for MEP and DTT are needed to increase the predictability for motor and functional outcomes.
In the current study, the primary purpose was to investigate the factors affecting the MEP responsiveness and parameters. The secondary purpose was to find the correlation between upper the extremity function and the combination of MEP with DTT.
MATERIALS AND METHODS
Subjects
A retrospective study design was used by analyzing the medical records of patients who had cerebrovascular disorders and received MEP tests in our clinic between June 2011 and March 2013. Among 121 patients, a total of 70 patients with 35 males and 35 females and a mean age of 62.59±12.38 years was included according to the following criteria: 1) first stroke ever, 2) unilateral hemispheric lesion, 3) supratentorial lesion, and 4) within 3 months after stroke onset. Patients with a previous history of stroke, bilateral hemispheric or infratentorial lesion and subarachnoid hemorrhage were excluded. The study protocol was approved by the Institutional Review Board of the university hospital.
Motor evoked potential
Patients were seated on a comfortable chair and the surface electromyography of the abductor pollicis brevis (APB) muscle was recorded. TMS was applied through a figure-of-eight coil (model C-B60) using MagPro X100 magnetic stimulators (Medtronic, Skovlunde, Denmark). MEPs were obtained from both APB muscles in a resting state. The resting motor threshold (RMT) was defined as the minimum stimulus intensity to obtain an MEP response greater than 50 µV in 5 of 10 trials. Three stimulations were performed each time with intensity set at 120% of RMT, and the MEP with mid-latency and mid-amplitude was adopted. MEP tests were performed within 5 days after admission to the rehabilitation department in most of the patients. The mean duration time from stroke onset until the test date was 29.75±14.64 days (range, 7-84 days). The patients were subdivided according to the presence or absence of MEP response on the affected APB (MEP-P group vs. MEP-N group). The ratio of latency and amplitude was calculated in MEP-P group, using a formula dividing unaffected value by affected value.
Diffusion tensor tractography
DTI were acquired using a 3.0-T Philips Gyroscan Intera MRI scanner (Philips Healthcare, Best, The Netherlands) with a six-channel phased array sensitivity encoding (SENSE) head coil. Images were obtained based on the single-shot echo-planar image sequence. The DTI data parameters were as follows: field of view 224×224 mm2; matrix 112×112; repetition time (TR)=9,131 ms; echo time (TE)=85 ms; slice thickness=2 mm; SENSE factor=2; and b=1000 s/mm2. We obtained 70-75 gapless, contiguous transverse images with applying along each of 32 non-collinear diffusion-sensitizing gradients.
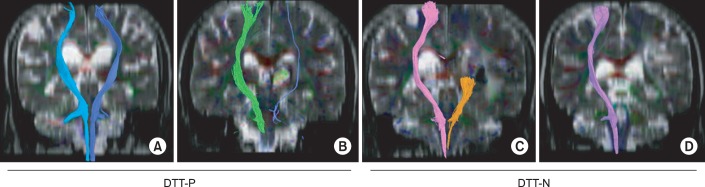
Fiber tracking was analyzed using the "FiberTrak" package included in the Extended MR Workspace R 2.6.3.1 software (Philips Healthcare). The termination criteria used were fractional anisotropy (FA) <0.2 and an angle change >30° according to the previous study for the optimal trackability threshold of FA [25]. Two regions of interests (ROI) were selected to reconstruct the CST. One ROI was placed on the CST portion of anterior lower pons level, and the other was placed on the CST portion of anterior mid pons level. Fiber tracts passing through both ROIs were designated as the final tract of interest. Patients were subdivided into four groups according to the study classification which was modified from a previous study of DTT in intracerebral hemorrhage [19]. The classification was as following: type A, CSTs are symmetrically preserved; type B, CSTs are preserved, but fiber numbers are asymmetric; type C, CSTs are interrupted at the lesion; and type D, CSTs are not constructed due to degeneration. Patients were categorized again into the DTT-P and as DTT-N group according to the CST integrity in the affected hemisphere. DTT-P group consisted of patients from type A and B groups, and the DTT-N group consisted of patients from type C and D groups (Fig. 1). Among the 70 patients which were enrolled in this study, a total 44 patients underwent the DTI tests. The DTI tests and likewise the MEP tests were performed in the most of patients within 5 days after admission to the rehabilitation department. The mean duration time from stroke onset was 31.52±16.09 days (range, 5-67 days). The mean time difference between MEP and DTI tests was 4.73±7.38 days (range, 0-34 days). Twenty-six of 44 patients belonged to the DTT-P group, and the other 18 patients belonged to the DTT-N group. The fiber number and FA value of affected hemisphere were obtained in the whole group. The ratio of fiber number and FA value (affected value divided by unaffected value) was calculated in the DTT-P group. While comparing DTT variables during analysis, 11 patients who belonged to type D of our DTT classification were excluded, because such variables were unobtainable due to degeneration of CST.
Clinical evaluation
Clinical variables including biographical (age, sex), neurological variables (time after onset of stroke, type of lesion, lesion location) and also functional variables were evaluated. Functional variables included the Brunnstrom stage of hand, the upper extremity subscore of Fugl-Meyer assessment (FMAU), the Manual Function Test (MFT), and the Korean version of the Modified Barthel Index (K-MBI).
The Fugl-Meyer assessment scale has a 100-point motor, where the point 66 regarded to the upper extremities. This scale is a measure tool for the stroke recovery [26]. The MFT was developed to assess the impairments in motor function of the affected upper extremity of stroke patients. It is composed of 32 items, which examine arm motions and manipulative activities (scores 0-32) [27]. In case of MFT and K-MBI, both admission and discharge scores of patients were obtained, but the admission scores only could be obtained for the Brunnstrom stage and FMAU.
Statistics
Statistical analysis was performed using SPSS ver. 18.0 software (SPSS Inc, Chicago, IL, USA). The chi-square test and independent t-test were used to analyze differences of biographical and neurological variables, such as lesion type, involved side and time post onset in the MEP-P and MEP-N groups. Depending on the presence or absence of the MEP, functional and DTT variables were compared using the independent t-test. Pearson correlation analysis was used to identify significant correlations between functional variables and MEP parameters. The Fisher exact test was used to show differences of DTT integrity in the MEP-P and MEP-N groups. The Mann-Whitney test and Kruskal-Wallis test were used to prove differences of functional and DTT variables in the combined group of MEP and DTT. Statistical significance was accepted for p-values of <0.05.
RESULTS
Comparison of variables ac cording to MEP responsiveness
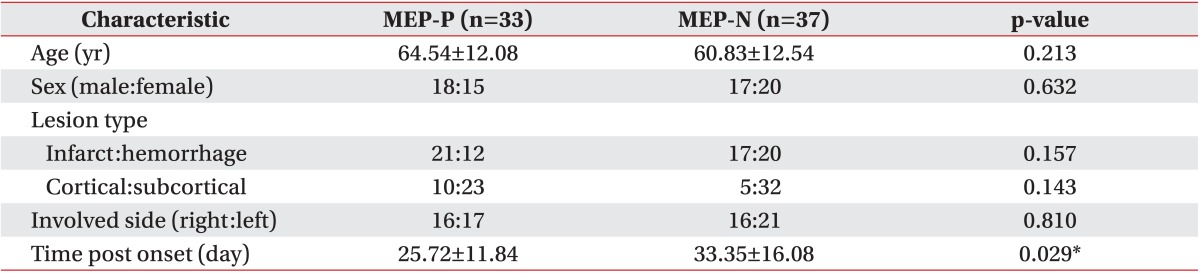
A total of 70 patients were included in this study, 35 women (50.0%) and 35 men (50.0%). Thirty-three patients were in the MEP-P group which showed a presence of MEP response, and 37 patients were in the MEP-N group with an absence of MEP response. Overall mean age was 62.59±12.38 years with no significant difference between the two groups. Also the lesion type and the involved side were not significantly different between the two groups. The duration from the onset of stroke to the MEP test was significantly different between the two groups (independent t-test; 25.72±11.84 in MEP-P group, 33.35±16.08 in MEP-N group; p=0.029) (Table 1), although an effect of the functional variables between both groups was not shown, was proved by analysis of covariance. Binary logistic regression analysis was also performed to estimate the possible biographical and neurological factors that could influence MEP responsiveness, and no significant influence was found.
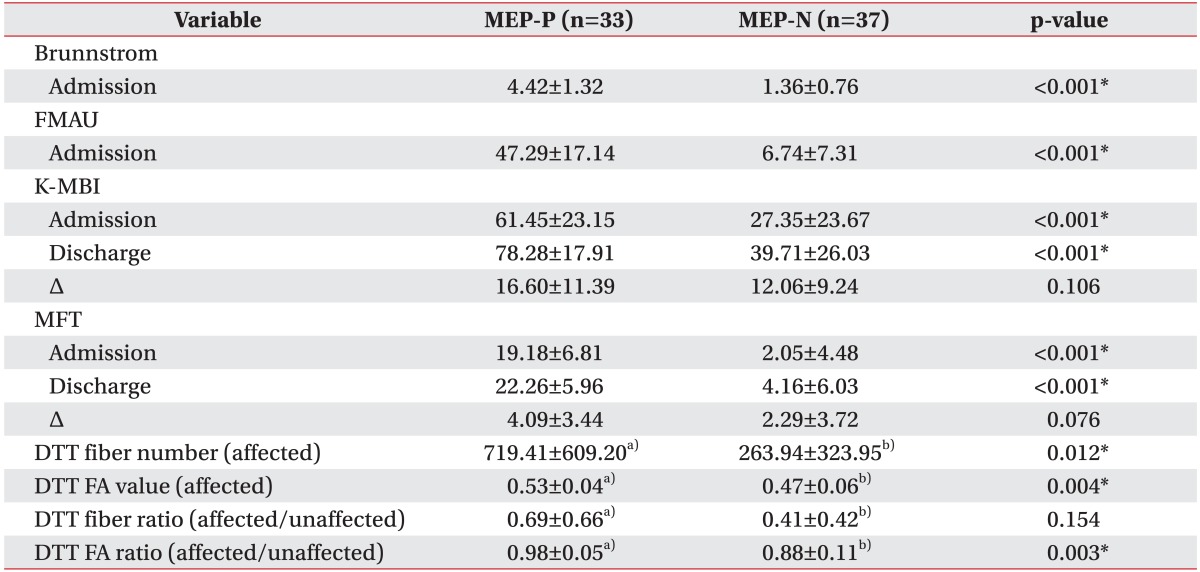
The Brunnstrom stage and the FMAU in patients on the admission time point to the physical medicine and rehabilitation department were significantly higher in the MEP-P group (p<0.001) (Table 2). The admission and discharge scores of MFT and K-MBI were significantly higher in the patients of MEP-P group (p<0.001). The differences between admission and discharge scores of MFT and K-MBI were obtained by subtracting discharge score by admission score, but the mean scores of differences were not significant (ΔMFT, p=0.076; ΔK-MBI, p=0.106; by independent t-test). Among DTT variables, the fiber number, FA value of affected side, and FA ratio (affected value/unaffected value) were significantly different between MEP-P and MEP-N groups, while fiber number ratio was not different (fiber number, p=0.012; FA value, p=0.004; fiber number ratio, p=0.154; FA ratio, p=0.003).
Relation of clinical variables and MEP parameters
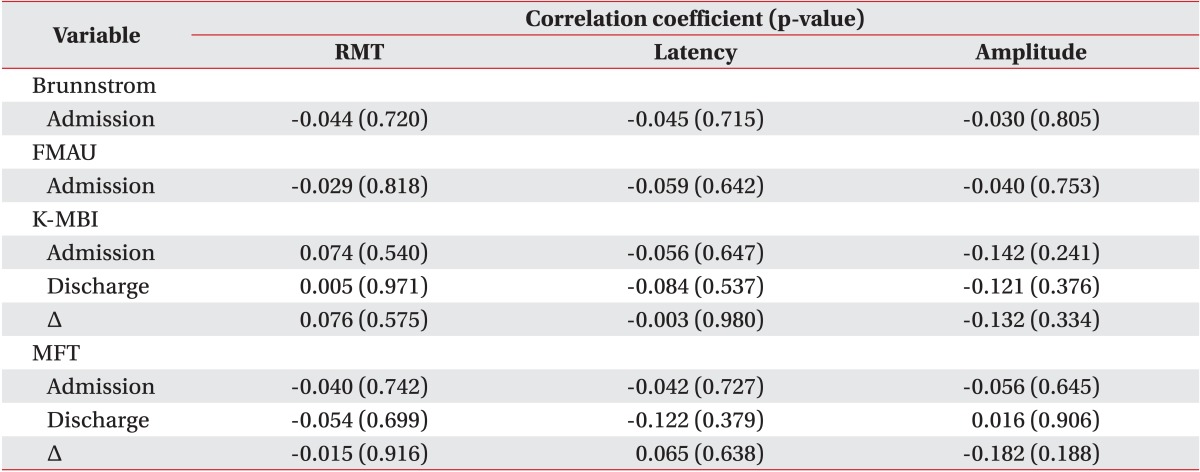
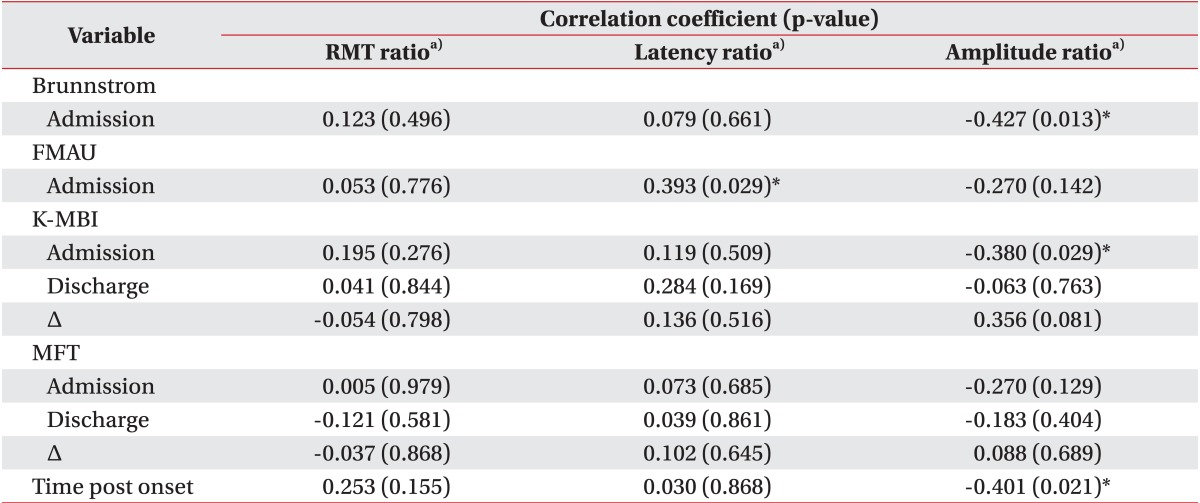
The MEP parameters of the unaffected hemisphere, such as RMT, latency, and amplitude, showed no significant correlation with clinical variables in the whole study patient group (Brunnstrom stage, FMAU, MFT, K-MBI; p>0.05 by Pearson correlation) (Table 3). For 33 subjects in the MEP-P group, correlations between ratio of RMT, latency, amplitude, and clinical variables were analyzed (Table 4). The amplitude ratio, which was calculated by dividing the unaffected value by the affected value, showed a significant negative correlation with the admission scores of Brunnstrom stage (r=-0.427, p=0.013) and K-MBI (r=-0.380, p=0.029), while no significant correlation was observed with admission scores of FMAU, MFT and discharge scores of K-MBI, MFT. The amplitude ratio showed a significant negative correlation with time post-onset (r=-0.401, p=0.021). This may indicate a tendency to return to normal amplitude ratio during the course of time. No significant relation between the RMT ratio and the latency ratio with the clinical variables was shown except the correlation between latency ratio and admission score of FMAU (r=0.393, p=0.029).
Combined study of MEP and DTT
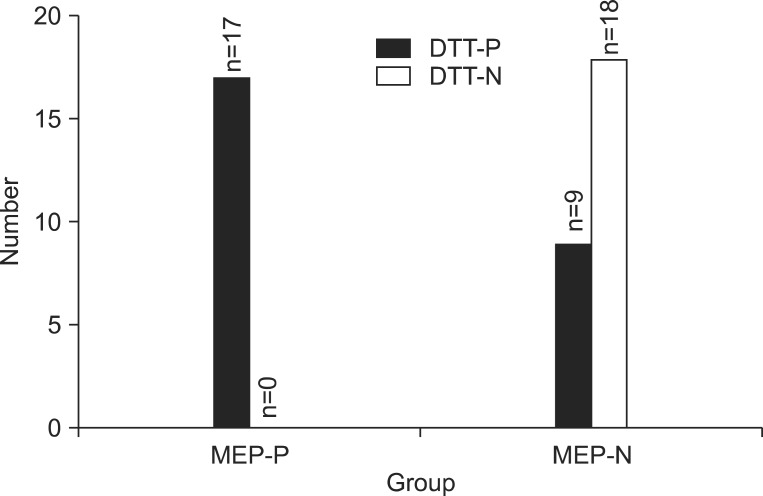
A total 44 patients who underwent both MEP and DTT were analyzed. All patients (n=17) who were included in MEP-P group belonged to the DTT-P group. Among the 27 patients in MEP-N group, 18 patients (66.7%) belonged to the DTT-N group, and the other 9 patients (33.3%) belonged to the DTT-P group. The distribution between groups were significantly distinct (p<0.001 by Fisher exact test) (Fig. 2).
According to the responsiveness of MEP and the integrity of DTT, patients were divided into three groups as both MEP-P and DTT-P group (n=17), either MEP-P or DTT-P group (n=9), and both MEP-N and DTT-N group (n=18) (Table 5). The Brunnstrom stage, FMAU, and MFT on admission showed significant differences between groups, which higher scores were reported in both MEP-P and DTT-P group than the other two groups (p<0.001 by Kruskal Wallis test).
DISCUSSION
The attempt of this study was to investigate the factors affecting the MEP responsiveness and parameters and it was also a study goal to find the correlation between the upper extremity function and the combined study of MEP with DTT. According to our results, upper extremity motor function, performance of activities of daily living (ADL) and the time post-onset are the factors which affect the MEP responsiveness and parameters, particularly the amplitude ratio. Also the combination of MEP with DTT is significantly correlated with the upper extremity motor function and the performance of ADL.
It was revealed in many previous studies the presence of MEP response had a prognostic value for motor recovery [4,8,28]. As a result of the present study, the Brunnstrom stage, FMAU on admission, and MFT on admission and discharge were significantly higher in the MEP-P group than those in the MEP-N group. The Brunnstrom stage and FMAU are used generally for the assessment of motor recovery after stroke, according to a movement with or without synergy. The MFT is also used in patients after stroke. It tests the motor function of upper extremity from moving in range of motion to manipulating a small object. Therefore, the presence of MEP response is associated with a better motor function of the upper extremity as well as with the motor strength. Moreover, K-MBI scores on patients' admission and discharge were also higher in the MEP-P group. In a previous study K-MBI had been reported to have a higher correlation with MFT [29]. The function of the upper limbs affects the degree of independence in ADL. Accordingly, the presence of a MEP response is also associated with an independent ADL performance. However, the differences between admission and discharge of MFT, K-MBI showed only borderline significances between the MEP-P and MEP-N groups. One possible reason for this insufficient result was the ceiling effect of MFT, K-MBI scores in the MEP-P group, as some of the patients reached almost the maximum scores for both tests. Another reason could be the small sample size for this study, not enough to reach a statistical significance. However, our findings are consistent with a previous study where the correlations between MEP and ADL in stroke patients were analyzed [30].
In this study the clinical factors which were correlated with MEP parameters were examined. The MEP amplitude has been known as not suitable for the neurophysiologic status assessment because of the wide variability. So the amplitude ratio can be used as an adequate measurement [11,12,15]. In the present study, the amplitude ratio showed a significant correlation with the Brunnstrom stage and the K-MBI score. Although it had only borderline significance, the amplitude ratio was related FMAU and MFT also. Son et al. [15] reported the amplitude ratio reflected the hand strength, but presented the general function of upper extremity and dextrity not well. However, this result suggests that the amplitude ratio reflect the general motor function of upper extremity and ADL performance.
The time post-onset showed a significant correlation with the amplitude ratio. To the best of our knowledge, there has been no study yet about the time influence on the MEP parameters, especially on the amplitude ratio. According to this study, the inter-hemispheric imbalance of amplitude tends to normalize during the course of time, while other MEP parameters, such as RMT and latency, were not significantly affected.
In 44 patients both MEP and DTT were performed, and an analysis between this two tests was conducted. Those 17 patients with a presence of MEP revealed an integrity of the CST on DTT, while 18 (66.7%) of 27 patients with a MEP absence showed a disruption of the CST on DTT. Both MEP and DTT evaluate the condition of the corticospinal pathway in each physiologic or neurostructural way. However, an absence of MEP could mean nerve cells are dead or have a very high motor threshold [31]. As MEP reflects a relatively long pathway from primary motor cortex to the recording hand muscle through the spinal cord, it might be more vulnerable to degeneration and disruption than DTT. According to the above results, DTT could be considered as a more sensitive tool to evaluate the corticospinal pathway than the MEP test in patients with MEP absence. The study result revealed that the DTT fiber number, FA value of affected side and the FA ratio were significantly higher in the MEP-P group. The DTT fiber number ratio was also higher in the MEP-P group but showed borderline significance only (p=0.154), caused probably due to the small sample size. The fiber number is determined by counting the number of voxels contained within a neural tract, and FA value indicates the directional integrity within the white matter [32]. Therefore, a decrease of the fiber number or FA value may estimate the degree of disruption on CST, and it is significantly associated with MEP responsiveness.
In this study, also the clinical variables related with the combination of MEP and DTT were investigated. The previous combined study of MEP and DTT had compared the abilities of MEP and DTT, and investigated the usefulness of the combined study to predict motor outcome [23,24]. In the present study, it was found that the group with MEP presence and integrity of CST on DTT showed a significantly higher Brunnstrom stage, FMAU, MFT, and K-MBI scores than the other two groups (either MEP-P or DTT-P group, both MEP-N and DTT-N groups). Through this study result, it may be suggested that the concurrent integrity of the MEP and DTT combination indicate a better upper extremity function and a better ADL also.
This study has a number of limitations. First, the sample size was relative small for the evaluation of various clinical factors. Even so, our analysis yielded many statistically significant findings. Second, those inherent to retrospective studies were also found in our study. Third, a follow up MEP test was not performed to identify the MEP parameter changes in relation to the improvement of clinical variables.
In conclusion, among the MEP parameters, the MEP responsiveness and amplitude ratio are significantly associated with clinical variables which indicate the upper extremity function and the performance of ADL. The inter-hemispheric imbalance of MEP amplitude tends to normalize during the course of time. The combined MEP and DTT tests provide useful informations in indicating the upper extremity function and performance of ADL, and further study involving larger sample size is needed.

 XML Download
XML Download