

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Encountering postoperative complications is like inevitable fate of surgeons. Particularly, the incidence of complications after colorectal cancer surgery has been reported in up to 40% of the cases [12]. Postoperative complications can prolong patients' hospital stay and affect readmission, reoperation, and medical expense burden. In addition, previous studies have reported negative results in long-term oncologic outcomes of many malignancies by damaging the immune system and causing systemic inflammatory response [34]. Recently, there is a growing interest in reducing complications and improving the quality of medical care for postoperative complications of colorectal cancer surgery. To improve surgical outcomes and quality of care, various attempts such as the implementation of the Enhanced Recovery After Surgery (ERAS) protocol and prehabilitation are being conducted [567]. In order to validate these attempts, an accurate tool for postoperative outcome evaluation and surgical quality control is needed.
The Clavien-Dindo classification (CDC) is the most widely used method to evaluate complications after surgery [8]. This classification has the advantage of being simple, intuitive, and reproducible. However, it is based on the standard of the most serious complication, thus, it poses the disadvantage of not being able to accurately evaluate other minor complications. As an alternative, the comprehensive complication index (CCI) was introduced in 2013 [9]. In CCI, all complications are weighted according to the CDC grade and counted as a sum score ranging from 0 to 100. Therefore, it has the advantage of quantitatively evaluating complications, including all minor complications. Furthermore, it is possible to quantitatively compare the rate of complications by period, surgeries, and institutions.
There are several reports that implementing the ERAS protocol reduces perioperative complications and hospital stays [101112]. However, studies that quantitatively evaluate complications of colorectal cancer surgery using CCI after implementation of the ERAS protocol are lacking. In addition, due to the shortened length of stay, there are concerns about complications that occur after discharge. Therefore, it is important to predict the occurrence of complications. The primary outcome of this study was to analyze complications using CCI in colorectal cancer patients with implementation of the ERAS protocol. It can be used as the basic data for surgical quality control. The secondary outcome was to investigate the predictive factors associated with the high morbidity rate. It can serve as a safety net in determining the timing of discharge.
METHODS
Study population
Ethical approval for this study was obtained from the Institutional Review Board of Seoul St. Mary’s Hospital (No. KC20RASI0859). This study was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature. The colorectal cancer database of our institution was retrospectively reviewed. A total of 335 consecutive patients who underwent elective colorectal cancer surgery between January 2017 and December 2017 at Seoul St. Mary’s Hospital, a high-volume tertiary care center, were enrolled. We excluded emergency surgery, minor surgeries such as transanal excision and stoma surgery. All operations were performed by 4 experienced colorectal surgeons. The patients' basic characteristics and perioperative outcomes were collected. Comorbidities were classified as hypertension, diabetes, coronary artery disease, cerebrovascular disease, chronic obstructive pulmonary disease (COPD), and liver disease. Tumor location was defined as the right colon including the cecum, ascending colon, hepatic flexure, transverse colon, and left colon including the splenic flexure, descending colon, and sigmoid colon. The rectum was defined as a tumor below the peritoneal reflexion. Obstructive colorectal cancer was defined as adenocarcinoma located between the cecum and rectum, showing obstructive findings on CT, or the colonoscope cannot pass beyond the lesion [13]. On CT findings, bowel obstruction showed proximal colon dilation up to the occlusion site and the distal portion was collapsed [14]. Blood tests were performed preoperatively, on operation day, postoperative day (POD) 1–2, and POD 3–4. In our institution, routine laboratory tests are performed between 1st–2nd and 3rd–4th days after surgery. The neutrophil-lymphocyte ratio (NLR), CRP, modified Glasgow prognostic score (mGPS), and colon inflammatory index (CII), known as predictors of systemic inflammation, were also evaluated [1516].
Enhanced Recovery After Surgery protocol
Enhanced Recovery After Surgery (ERAS) protocol was implemented in the same way as described in our previous study [6]. Briefly, it includes preadmission patient education, oral carbohydrate drink 2 hours before surgery, restrictive fluid strategy, opioid-sparing multimodal pain control, early removal of drainage, early mobilization and early oral intake. In our institution, it applies the same way to all patients undergoing colorectal surgery, and some patients with obstructive cancer have omitted mechanical bowel preparation.
Definition of complication
All complications that occurred within 30 days after surgery were categorized and recorded using the CDC (Supplementary Tables 1, 2). We classified complications by wound complication, urinary retention, bleeding (intraperitoneal, intraluminal), anastomosis leakage, intraperitoneal abscess, ileus, cardiovascular disease (acute myocardial infarction, arrhythmia, pulmonary thromboembolism, and deep vein thrombosis), pulmonary disease (pneumonia and acute respiratory distress syndrome), other organ injuries, and other uncommon complications. Anastomosis leakage is defined as a clinical or radiologic finding of a defect of intestinal wall integrity at the site of anastomosis [17]. CCI was calculated in the same way as described in previous studies (formula for the CCI =  [918]. Also, it can be easily calculated by using the tool provided by the webpage (https://www.assessurgery.com). Severe complications (CDC IIIa or higher) require immediate intervention. Based on previous studies, we defined the cutoff value for high CCI as 26.2. This value corresponds to 1 CDC grade IIIa [19]. The groups were divided into high (CCI ≥ 26.2) and low (CCI < 26.2). The predictive factor analysis for the high CCI group was also performed.
[918]. Also, it can be easily calculated by using the tool provided by the webpage (https://www.assessurgery.com). Severe complications (CDC IIIa or higher) require immediate intervention. Based on previous studies, we defined the cutoff value for high CCI as 26.2. This value corresponds to 1 CDC grade IIIa [19]. The groups were divided into high (CCI ≥ 26.2) and low (CCI < 26.2). The predictive factor analysis for the high CCI group was also performed.
[918]. Also, it can be easily calculated by using the tool provided by the webpage (https://www.assessurgery.com). Severe complications (CDC IIIa or higher) require immediate intervention. Based on previous studies, we defined the cutoff value for high CCI as 26.2. This value corresponds to 1 CDC grade IIIa [19]. The groups were divided into high (CCI ≥ 26.2) and low (CCI < 26.2). The predictive factor analysis for the high CCI group was also performed.Statistical analyses
Categorical variables were compared using the chi-square or Fisher exact test and continuous variables were compared using the t-test or Mann-Whitney U-test. All analyses were based on available data. Univariate and multivariate analyses were performed by logistic regression analysis to identify predictive factors associated with the high CCI group. Variables with a P-value of <0.1 in the univariate analysis were introduced to the multivariable analysis by logistic regression. The optimal cutoff value of postoperative CRP was determined by receiver operating characteristic (ROC) curve analysis. Statistical analyses were performed using IBM SPSS Statistics ver. 24.0 (IBM Corp., Armonk, NY, USA). A P-value of <0.05 was considered statistically significant.
RESULTS
Patients' demographics
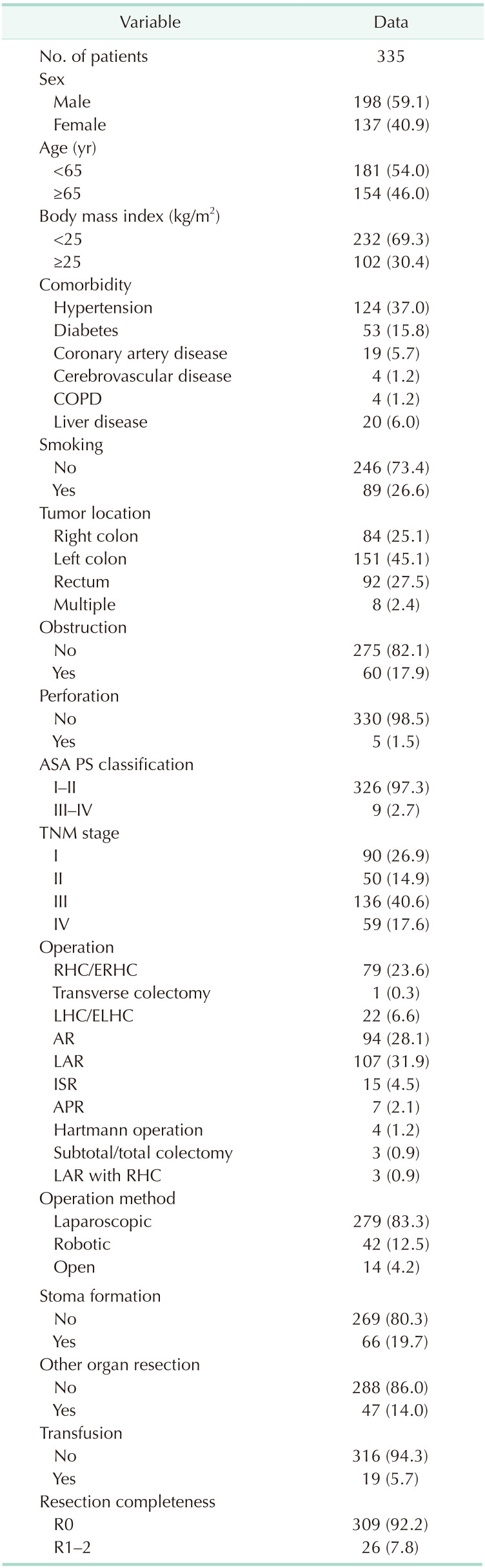
A total of 335 patients were included, with 198 male patients (59.1%) and 137 female patients (40.9%). Among the patients, 154 (46%) were ≥65 years of age and 102 (30.4%) had a body mass index (BMI) of ≥25 kg/m2. There were 124 patients (37.0%) with hypertension, 53 (15.8%) with diabetes, 19 (5.7%) with coronary artery disease, and 4 (1.2%) with COPD. According to tumor location, 84 patients (25.1%) had tumors in the right colon, 151 (45.1%) in the left colon, and 92 (27.5%) in the rectum. Colorectal cancer obstruction was observed in 60 patients (17.9%) and perforation in 5 patients (1.5%). According to surgical approach, 279 patients (83.3%) underwent laparoscopic surgery, 42 (12.5%) underwent robotic surgery, and 14 (4.2%) underwent open surgery (Table 1).
Postoperative complications
Among the 335 patients, 116 (34.6%) developed postoperative complications. Wound complications, including superficial surgical site infection and wound dehiscence, were the most common complications in 26 patients (7.8%). Postoperative ileus was the second most prevalent complication in 24 patients (7.2%). Additionally, 16 (4.8%) patients had urinary retention, 15 (4.5%) had anastomosis leakage, and 15 (4.5%) had intraperitoneal abscess (Supplementary Table 1).
Comparisons based on complications by surgery revealed that 18 patients (22.8%) had complications in right hemicolectomy (RHC), 8 (36.4%) in left hemicolectomy (LHC), 26 (27.7%) in anterior resection (AR), 43 (40.2%) in low anterior resection (LAR), 11 (73.3%) in intersphincteric resection (ISR), and 5 (71.4%) in abdominal perineal resection (APR). Wound complications occurred in 4 (5.1%) patients in RHC, 3 (3.2%) in AR, 8 (7.5%) in LAR, 4 (26.7%) in ISR, and 4 (57.1%) in APR. Urinary retention occurred in 1 (1.3%) patient in RHC, 2 (2.1%) in AR, 8 (7.5%) in LAR, 1 (6.7%) in ISR, and 3 (42.9%) in APR. Postoperative ileus occurred in 8 patients (10.1%) in RHC, 2 (2.1%) in AR, 6 (5.6%) in LAR, 2 (13.3%) in ISR, and 1 (14.3%) in APR (Supplementary Table 1). Of the 335 patients, 29 (8.7%) developed severe complications (CDC IIIa or higher). Among those cases, anastomosis leakage was the highest in 12 patients (3.6%). Anastomosis leakage occurred in 1 (1.3%) patient in RHC, 1 (1.1%) in AR, 9 (8.4%) in LAR, and 1 (6.7%) in ISR (Supplementary Table 2).
Comprehensive complication index score
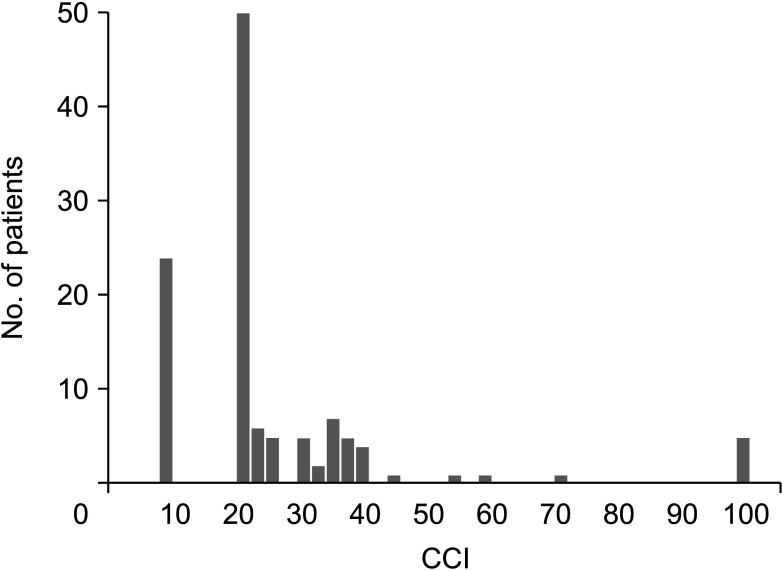
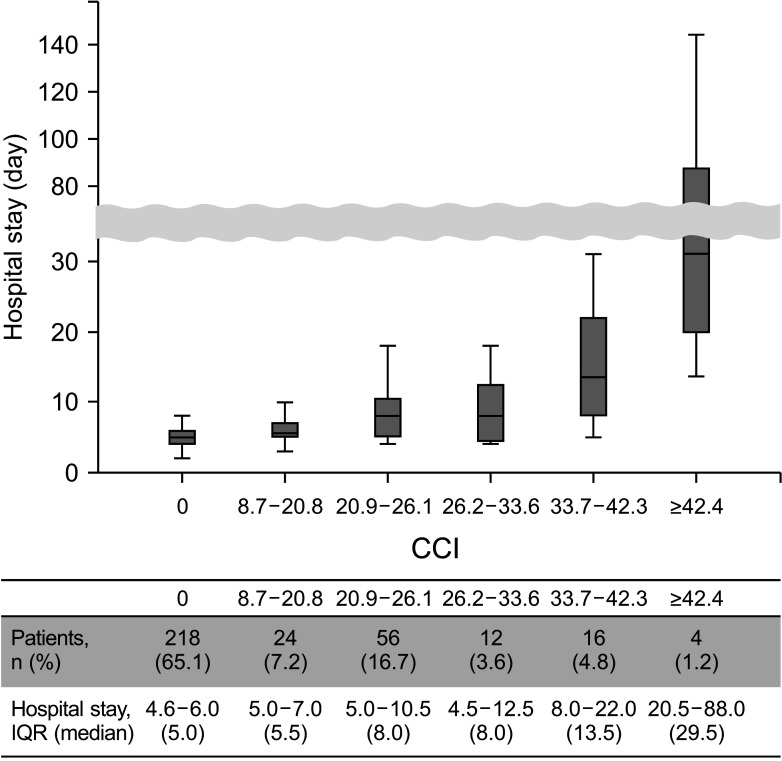
After calculating the CCI score of all patients, the distribution is shown in Fig. 1. Of the 335 patients, the mean CCI for overall colorectal cancer surgery was 9.1 ± 16.7. The number of patients featuring low CCI (<26.22) was 297 (88.7%) and high CCI (≥26.22) was 38 (11.3%). Since there is a corresponding CCI score for each CDC (8.7 = CDC I, 20.9 = CDC II, 26.2 = CDC IIIa, 33.7 = CDC IIIb, 42.4 = CDC IVa, and 46.2 = CDC IVb), it shows high values at 8.7 and 20.9, corresponding to CDCs I and II, respectively. As the CDC grade increased, the CCI scores showed a wider range of distribution. Patients with the highest degree of complications with CDC III had a CCI distribution between 26.2 and 44.7. In addition, patients with the highest degree of complications with CDC IV showed CCI distribution between 53.2 and 70.3. This was because patients with severe complications are often accompanied by several mild complications. The length of hospital stays according to the CCI score is shown in Fig. 2. The median length of stay in 218 patients (65.1%) without complications was 5 days (interquartile range [IQR], 4.0–6.0 days). As the CCI scores increase, hospital stays were prolonged. The CCI scores of 26.2–33.6, 33.7–42.3, and 42.4–46.2 corresponding to severe complications were hospitalized for 8 days (IQR, 4.5–12.5 days), 13.5 days (IQR, 8.0–22.0 days) and 29.5 days (IQR, 20.5–88.0 days), respectively.
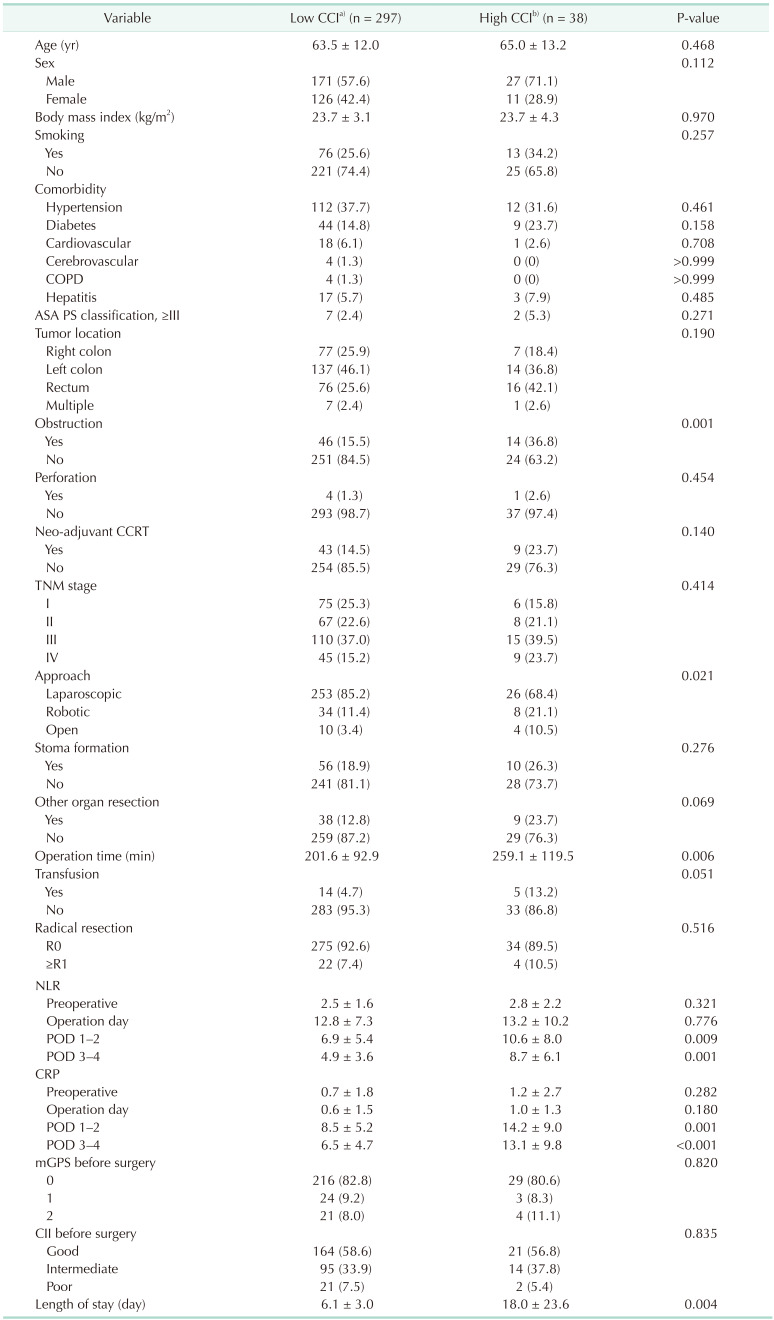
The basic characteristics and perioperative outcomes between the low and high CCI groups are compared in Table 2. There were no significant differences in age, sex, BMI, smoking, comorbidity, American Society of Anesthesiologists physical status classification, or tumor location between the 2 groups. Obstructive colorectal cancer was significantly higher in the high CCI group than in the low CCI group (14 [36.8%] vs. 46 [15.5%], P = 0.001). The ratio of open and robotic surgery was higher in the high CCI group than in the low CCI group (P = 0.021). Operation time was significantly longer in the high CCI group (259.1 ± 119.5 minutes vs. 201.6 ± 92.9 minutes, P = 0.006). In laboratory findings, preoperative NLR, CRP, mGPS, and CII showed no difference in both groups. However, NLR POD 1–2, NLR POD 3–4, CRP POD 1–2, and CRP POD 3–4 was higher in high CCI group than in low CCI group, respectively (10.6 ± 8.0 vs. 6.9 ± 5.4, P = 0.009; 8.7 ± 6.1 vs. 4.9 ± 3.6, P = 0.001; 14.2 ± 9.0 mg/dL vs. 8.5 ± 5.2 mg/dL, P = 0.001; 13.1 ± 9.8 mg/dL vs. 6.5 ± 4.7 mg/dL, P < 0.001). The high CCI group showed a prolonged length of hospital stay (18.0 ± 23.6 days vs. 6.1 ± 3.0 days, P = 0.004).
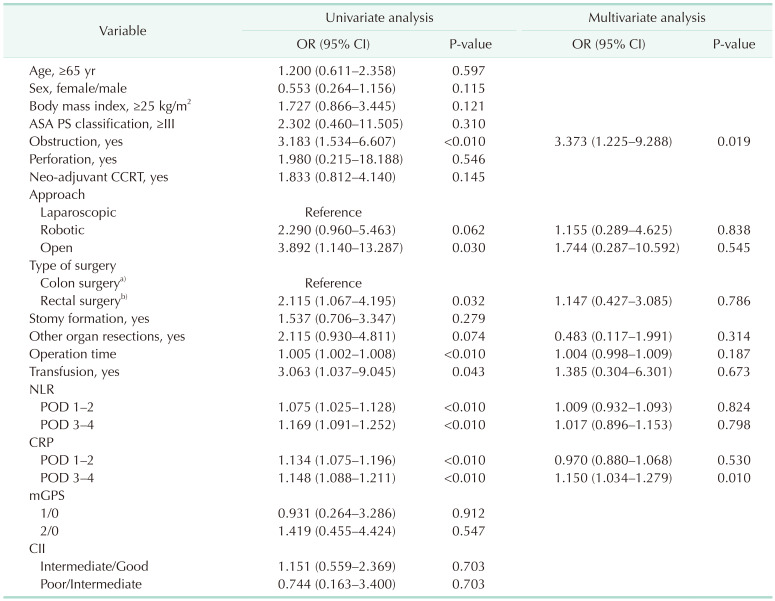
In univariate analysis, obstructive colorectal cancer, operation method, operation time, transfusion, NLR POD 1–2, NLR POD 3–4, CRP POD 1–2, and CRP POD 3–4 were associated with high CCI. In multivariate analysis, obstructive colorectal cancer (odds ratio, 3.278; 95% confidence interval, 1.217–8.829; P = 0.019) and CRP POD 3–4 (odds ratio, 1.152; 95% confidence interval, 1.036–1.280; P < 0.010) were significant predictors for high CCI (Table 3). Detailed complications in these patients were described in Supplementary Table 3.
Subgroup analysis according to postoperative CRP
The distribution of complications according to postoperative CRP was analyzed by subgroup (Supplementary Table 4). The cutoff values for CRP POD 1–2 and CRP POD 3–4 were determined by the ROC curve, and the values were 9.21 mg/dL and 6.47 mg/dL, respectively. We divided the 4 groups according to the cutoff value. Low-Low (POD 1–2 CRP, low; POD 3–4 CRP, low), High-Low (POD 1–2 CRP, high; POD 3–4 CRP, low), Low-High (POD 1–2 CRP, low; POD 3–4 CRP, high), High-High (POD 1–2 CRP, high; POD 3–4 CRP, high). A total of 244 patients with available CRP values were analyzed. In the Low-Low group, 85 patients (73.9%) did not show any complications, and there were 4 CDC IIIa (3.5%) and 1 CDC IIIb (0.9%). In the High-Low group, 21 patients (80.8%) did not show any complications, and there was 1 (3.8%) with CDC IIIb. In the Low-High group, 17 patients (58.6%) did not show any complications, and there was 1 (3.4%) CDC IIIa and 1 (3.4%) CDC IIIb. In the High-High group, 29 patients (39.2%) did not show any complications, and there were 4 (5.4%) CDC IIIa, 6 (8.1%) CDC IIIb, 2 (2.7%) CDC IVa, 1 (1.4%) CDC IVb, and 2 (2.7%) CDC V. Patients with severe complications, CDC IIIa or higher, was observed in 5 patients (4.3%) in Low-Low group, 1 (3.8%) in the High-Low group, 2 (6.9%) in the Low-High group, and 15 (20.3%) in the High-High group. There was a significant statistical difference in patients without complications (P < 0.001) and patients with severe complications (P = 0.002) in each group.
DISCUSSION
According to previous reports, early postoperative complications in colorectal cancer patients were reported in 19%–40% [1220]. In this study, the results were similar to those of previous reports. Previous reports have shown that the incidence of surgical site infection after colorectal surgery ranges from 5% to 20%, and the incidence of ileus is estimated to be around 10%–30% [212223]. The incidence rates of this study were similar but relatively low; 7.8% and 7.2%, respectively.
In comparison by operation type, patients who underwent ISR and APR had an overall complication rate of 70% or higher, and those who underwent LAR had an overall complication rate of 40.2%. On the other hand, the overall complication rate in patients who underwent colectomy and AR was significantly lower (22.8%–36.4%). Surgical complications such as surgical site infection (wound complication, intraperitoneal abscess), urinary retention, and anastomosis leakage were more prevalent in rectal cancer surgery. General complications such as cardiovascular disease and pulmonary disease showed similar incidence rates for each type of surgery. As shown in Table 2, robotic surgery was more frequent in the high CCI group, but it was due to the difference in the surgical site. In our institution, robotic surgery was only applied to rectal cancer surgery. Thus, the patients who underwent robotic rectal cancer surgery were inclined to have higher CCI than those who underwent laparoscopic colorectal surgery in this study.
Concurrently, there are only few cases that reported complications assessed by CCI. The mean CCI for laparoscopic gastrectomy was 4.9 ± 9.5, mean CCI for open gastrectomy was 9.0 ± 13.4, and mean CCI for natural orifice transluminal endoscopic cholecystectomy was 3.5 ± 6.4 [1824]. In our study, the mean CCI for overall colorectal cancer surgery was 9.1 ± 16.7. In comparison by surgery, mean CCI for colectomy was 6.1 ± 13.8, AR was 7.9 ± 17.2, LAR was 10.9 ± 17.4, APR was 16.6 ± 14.2, and ISR was 20.5 ± 24.7, respectively. Using CCI, it can quantitatively compare the severity of complications by the operation method and operation type. Furthermore, it is possible to compare complications by period and according to the change in treatment modality.
Fig. 2 shows the length of hospital stay according to the CCI score. Most patients without complications were discharged on POD 4–6 days according to the ERAS protocol. The length of hospital stay is shortened by 30%–50% compared to traditional treatment [25]. However, similar to previous reports, as CCI scores increase, the length of hospital stays tends to increase [1826]. The correlation coefficient R was 0.435 (P < 0.001), which shows a moderate correlation. This observation was due to extreme cases of patients who died within 10 days and those who lived that were discharged after hospitalization for more than 140 days. Shortened hospital stay has the advantage of improving patient satisfaction, improving quality of care, and reducing medical costs, but there is a concern about the occurrence of complications after discharge. Evaluating the predictive factors of high morbidity can help determine the timing of discharge and cautious care.
Obstructive colorectal cancer and CRP POD 3–4 were highly associated with high CCI in multivariable analysis. Colorectal cancer obstruction is known to be associated with high complication rates [2728]. Obstruction causes pathophysiologic changes such as dilation of the proximal colon, impaired blood flow in the bowel wall, imbalance of water and electrolytes, and frequent infection [29]. It represents a more advanced stage, often accompanied by other organ metastasis, and the operation is more complicated [30]. In addition, since the incidence of anastomosis leakage is high, a stoma is often made to protect it. Although data were not shown, in this study, patients with obstructive colon cancer had higher TNM stage, higher rate of open surgery, and higher preoperative mGPS and CII.
CRP is an acute phase protein synthesized in the liver and its concentration increases according to the inflammatory response [31]. In the acute inflammatory phase, CRP begins to increase from 4–6 hours and peaks at 36–50 hours [32]. This is a sensitive indicator of postoperative systemic inflammatory response, and in our institution, it is routinely measured before and after surgery. In our study, CRP POD 3–4 appeared to be a strong predictive factor associated with high CCI. The optimal cutoff value for CRP POD 3–4 was determined according to the ROC curve (CRP, 6.47 mg/dL). In the subgroup analysis, regardless of the high and low values of POD 1–2 CRP, the incidence of severe complications was low when POD 3–4 CRP was low (Supplemetary Table 4). However, the incidence of severe complications was high in the group with high POD 3–4 CRP. Of the 23 patients with severe complications, 17 patients (73.9%) showed high POD 3–4 CRP. In addition, severe complications were significantly higher in the High-High group (P = 0.002). In cases when both POD 1–2 and POD 3–4 CRP were high, the severity and frequency of complications tended to increase further. Yamashita et al. [4] reported that postoperative NLR was highly correlated with high CCI, but this study did not show statistical significance in multivariable analysis. Other predictors of systemic inflammation, mGPS and CII, also did not show a significant correlation with high CCI. Based on our study, even for colorectal cancer patients who implemented the ERAS protocol, it is recommended that reconsider the timing of discharge in cases of obstructive colorectal cancer or CRP POD 3–4 of 6.47 or higher.
There were several limitations in this study. First, it was a retrospective study. Minor complications that did not require admission were not evaluated after discharge. In addition, the date of blood test is heterogeneous, such as POD 1–2 and POD 3–4. Due to the limitations of retrospective design, it can be evaluated with further prospective studies. Second, the sample size is relatively small. Analysis of complications by period and according to the change in treatment modality can be evaluated in a further large cohort study. However, to our knowledge, this is the first report to analyze factors related to high CCI in colorectal cancer surgery using the ERAS protocol. This can be used as a reference study for surgical quality control in our institution, and prospective studies will follow in the future.
In conclusion, it is feasible and clinically useful to evaluate postoperative complications using CCI in colorectal cancer with the ERAS protocol. Furthermore, it can be used for surgical quality control by comparing the CCI between operations, institutions, and periods. The strong predictive factors for a high CCI were obstructive colorectal cancer and POD 3–4 CRP (≥6.47 mg/dL). Patients with these findings require more cautious care, and careful determination of the timing of discharge.
 XML Download
XML Download