

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In the clinical field, spasticity is commonly assessed by the modified Ashworth scale (MAS).1 Even though the inter-rater and intra-rater reliability of the MAS is good, some limitations exist because spasticity is measured subjectively by the rater's own hand.2,3
The pendulum test is a biomechanical method of evaluating muscle tone by using gravity to provoke muscle stretch reflex during passive swinging of the lower limb. Some researchers have reported that the ratio of the amplitude of the swings significantly correlated with clinical scales such as the MAS scores in spastic patients. However, this test also has limitations, such as difficulty in keeping patients in a fully relaxed status, difficulty in measuring the spasticity in different angular velocities and in usage at other joints.4
The isokinetic dynamometer has been widely used for quantitative assessment and evaluation of spasticity. It allows accurate joint stretching according to specific angular velocities and quantitative measurement of resistance and spasticity. However, it is hardly used in clinical settings because of the large size of the device as well as poor mobility.5
In addition, the H-reflex and T-reflex are available for assessing spasticity. However, the results of these tests poorly correlate with the cause of spasticity, lesion site and degree of spasticity.6
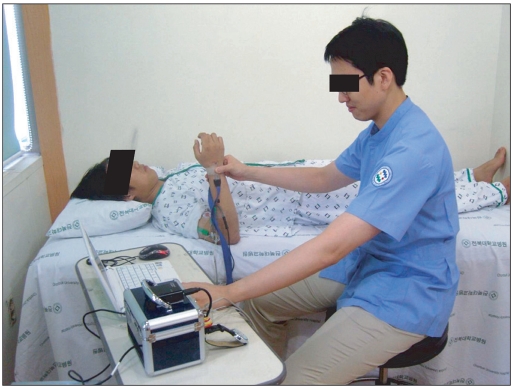
To overcome the problems that were encountered using the previous methods of measuring spasticity, we introduced a portable hand-driven isokinetic system for measuring spasticity quantitatively and comprehensively with mobility.7 Upon evaluation of spasticity of the elbow using this system, the examiner grasps the wrist of the subject and passively extends and flexes the elbow joint as the clinical bedside method for measuring spasticity. This system is designed to measure the joint angle, EMG signals, angular velocity, and torque during passive elbow movements.
The objective of this study was to evaluate the stretch reflex of the elbow joint of normal persons and analyze the parameters before the application of this system on patients with spasticity.
MATERIALS AND METHODS
Participants
Thirty normal persons (18 males and 12 females) without history of diseases involving the central nervous system (mean age 25.7, range 22-30 years) were enrolled in this study. The subjects did not show neurologic symptoms, signs or spasticity either (MAS 0).
Methods
Portable isokinetic system
This developed system was designed to measure the angle, angular velocity, torque and EMG signals by moving the elbow joint of a subject with the examiner's own hand. The surface EMG signal was measured using 10 mm diameter, disposable Ag-AgCl electrodes (Meditrace™ 200, Tyco Healthcare Group LP, Mansfield, Massachusetts, USA). Two active electrodes were placed on the belly of the biceps brachii (BB) muscle and triceps brachii muscle, respectively. Two reference electrodes were attached firmly on the medial and lateral aspect of the elbow joint. The ground electrode was placed on the middle of the forearm. The joint angle of the elbow was measured by means of a twin-axis flexible electro-goniometer (SG150®, Bio metrics Ltd., Gwent, UK) attached on the arm and forearm along the lateral side. In addition, the angular velocity was calculated by the differentiation of the angle signals. Torque was measured by two pressure sensors (FlexiForce A201® Tekscan, South Boston, Massachusetts, USA) attached around the wrist. The examiner grabbed the wrist and the pressure sensors and performed passive elbow extension/flexion movement during this study. The resulting data were then transferred to a laptop computer via its USB port and simultaneously displayed on the monitor. The data were also analyzed by newly developed software using the Labview language (ver. 8.6, National Instrument™, Autin, Texas, USA).
Experimental protocol
The subjects comfortably lay down in the supine position, and the upper limb was slightly abducted and relaxed (Fig. 1). To monitor the activity of the elbow flexor and extensor, surface electrodes (Meditrace 200, Kendall, US) were attached to the arm. The skin for the electrodes was cleaned with a 95% ethanol mixture to reduce skin impedance. Two pressure sensors were also attached on the wrist of the subject, anteriorly and posteriorly. The 'sensor calibration' button was used to manually remove the offset of the signals measured by the various sensors. The '0° setting' and '90° setting' buttons were used for converting the voltage signals obtained from the flexible electro-goniometer to the specific angular displacement. In order to reduce the muscle tension, the subjects were taught not to contract the biceps and triceps muscles during the test and had 3 instances of passive extension-flexion practice before the test. The subjects lay on a bed in a relaxed position. The starting position involved the slight abduction of the shoulder, neutral position of the wrist and full flexion of the elbow. In order to reduce muscle tension, the subjects maintained this starting position for at least 2 minutes. The tests started after confirming the silence of EMG signals by monitoring them. The subject's elbow joint was passively extended and flexed by the examiner at a randomly selected stretching angular velocity of either 60, 90, 120, 150 and 180°/sec, in order to avoid adaptation of the stretch response. A motion from full flexion to full extension was defined as 'elbow extension', whereas 'elbow flexion' was defined as a motion from full extension to full flexion. 'Full extension' meant an angle of 0o between the arm and forearm, while 'full flexion' meant an angle of about 120°. One cycle of elbow joint motion consisted of one elbow extension and one flexion over an approximate angle range of 120°→0°→120°. Measurements were performed repeatedly ten times at the selected stretching angular velocity with at least 10 seconds of rest between each measurement. Proper angular velocity of the elbow joint motion could be maintained by the beeping sound of the device. The maximal EMG amplitude and the maximal torque were collected at each stretching angular velocity.
RESULTS
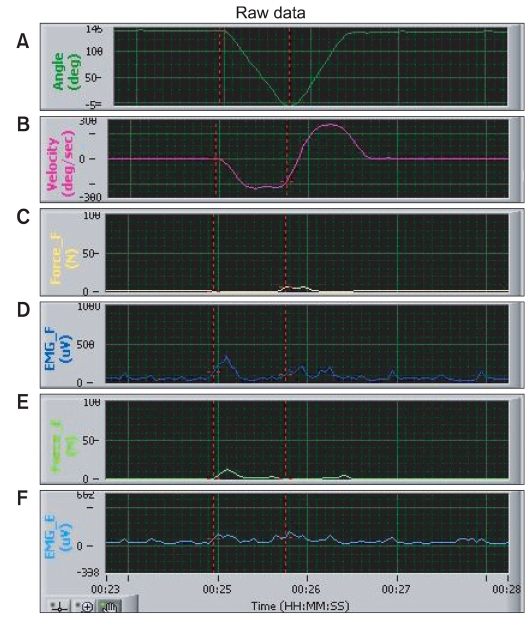
We observed EMG activity and torque even in normal persons without spasticity (Fig. 2). EMG activity was observed in biceps when the elbow was extended and in triceps when the elbow was flexed. Torque was measured when the elbow was extended and flexed.
The maximal EMG activity
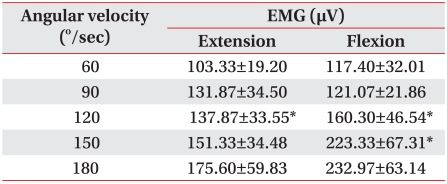
In normal subjects without spasticity, the maximal EMG activities recorded on biceps and triceps showed an increasing tendency with incremental increase of stretching angular velocities (Table 1). The maximal EMG activity recorded on the biceps when the elbow joint was passively extended showed increasing tendency compared to the stretching angular velocity of 60°/sec and 90°/sec, 90°/sec and 120°/sec, 120°/sec and 150°/sec, 150°/sec and 180°/sec, respectively. The maximal EMG activity recorded on the biceps significantly increased on the stretching angular velocity of 120°/sec compared to the stretching angular velocity of 90°/sec. The maximal EMG activity recorded on the triceps when the elbow joint was passively flexed increased on the stretching angular velocity of 120°/sec and 150°/sec compared to the stretching angular velocity of 90°/sec and 120°/sec, respectively (p<0.05).
The maximal torque of the elbow joint
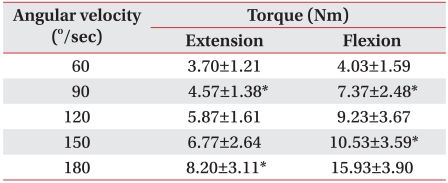
In normal subjects without spasticity, the maximal torque recorded on the sensors attached to the subject's wrist increased with incremental increase of stretching angular velocities (Table 2). When the elbow joint was passively extended, the maximal extension torque recorded on the wrist increased on stretching angular velocity of 90°/sec and 180°/sec compared to 60°/sec and 150°/sec, respectively. The maximal flexion torque recorded on the wrist when the elbow joint was passively flexed increased on stretching angular velocity of 90°/sec and 150°/sec compared to 60°/sec and 150°/sec, respectively (p<0.05). Interestingly, the maximal torque increased as they were compared to the stretching angular velocity of over 60°/sec difference (p<0.05).
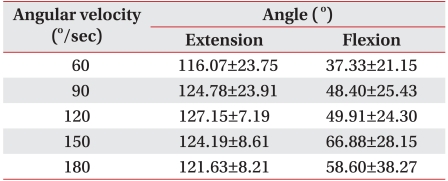
Elbow joint angle when maximal EMG activity was recorded
In normal subjects without spasticity, the elbow joint angle at the maximal EMG activity on biceps was the biggest at the angular velocity of 120°/sec. The elbow joint angle at the maximal EMG activity on biceps was significantly different between the stretching angular velocity of 60°/sec and 120°/sec, and 120°/sec and 180°/sec, respectively. In normal subjects without spasticity, the elbow joint angle when the maximal EMG activity on triceps was observed was the biggest with stretching angular velocity of 150°/sec. However, there was no significant difference between the stretching angular velocities (Table 3).
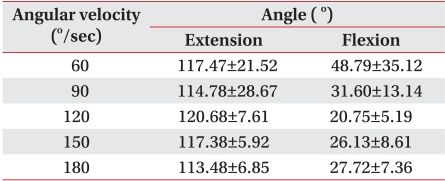
The elbow joint angle when the maximal torque was recorded
In normal subjects without spasticity, the elbow joint angle when the maximal torque was observed on passive extension was the biggest at the angular velocity of 120°/sec. The elbow joint angle when the maximal torque of the elbow joint was observed on passive flexion was the biggest at the angular velocity of 60°/sec (Table 4).
DISCUSSION
The present study showed that EMG activity and torque during the passive motion of elbow joint increased with incremental increase of stretching angular velocities. These results are possibly due to 1) the increase of inertial force due to acceleration, 2) viscoelastic property of muscle and joint tissue, and 3) antagonistic muscle contraction due to stretch reflex.8-10
Simon et al.11 reported that EMG activity and torque of the knee joint increased with incremental increase of angular velocities during the knee joint's passive extension-flexion in rat. These findings were possibly because of passive torque and stretch reflex related to the proprioceptor. Pisano et al.12 reported that the EMG activity and torque of flexor carpi radialis and extensor digitorum communis were recorded when a normal subject's wrist stretched with a servo-controlled torque motor in 500°/sec of angular velocity increased compared to 10°/sec of angular velocity. They also reported that stretch reflex was recorded in 54% of normal subjects. Lee et al.13 reported that stretch reflex was recorded in the ankle joints of all normal subjects and hemiplegic patients examined with an isokinetic dynamometer and dynamic EMG recorder. In the present study, the stretch reflex was recorded in all subjects. The maximal torque recorded on the wrist during passive motion increased as the stretching angular velocity significantly increased over 60°/sec interval. Direct comparison with other studies is inappropriate because previous studies involving the elbow joint are lacking. In the present study, all normal subjects showed stretch reflex, which was different to the results of Pisano's study.12 Those differences are thought to be caused by 1) the differences of spasticity measurement sites, 2) the differences of length of each muscle, and 3) the differences of measurement technique. Clinical experiences that the spasticity was observed more commonly in the elbow than in the wrist support our results.
In clinical settings, the examiner usually passively extends and flexes the upper limb for measuring the spasticity of the upper extremity. Quantitative data such as the joint angle, torque and EMG activity was obtained during the passive elbow extension-flexion.14,15 On examining the spasticity with the modified Ashworth scale, the data tended to be subjective, and it was difficult to maintain the stretch angular velocity. Therefore, we designed this portable hand-driven isokinetic system to make an electric "beep" sound to match extension-flexion to maintain the stretch angular velocity. Before the measurement, the examiner practiced the rhythmic stretch sufficiently. In normal subjects, the elbow joint angle, when the maximal EMG activity was observed in each stretch angular velocity, was 116-127 degrees on elbow extension, 37-66 degrees on elbow flexion. The difference of the angle when the maximal EMG activity was observed was not significant between each stretching angular velocity (Table 3). That is, the joint angle when the maximal stretch reflex appears was similar in each stretch angular velocity. Lee et al.16 also observed the maximal torque of the ankle when passive joint exercise was applied with isokinetic dynamometer. They presented that the joint angle of maximal torque was not different between each stretch angular velocity.
Levin and Feldman17 quantitatively measured the stretch reflex by tonic stretch reflex threshold (TSRT), which is a linear regression of dynamic stretch reflex threshold. Our results suggested a way to analyze the stretch reflex quantitatively using comprehensive data such as EMG activity, joint angle and angular velocity, and torque.
The objective of this study was to evaluate the elbow joint of normal persons and analyze the parameters before the application of the new portable hand-driven isokinetic exercise system on spastic patients. We could detect EMG activity and torque by the system in normal subjects without spasticity. The data we collected could be good reference data for analyzing spasticity with this system.
The limitation of this study was that the baseline of the EMG signal was not calm. The authors had difficulties in detecting the take off point of EMG signal from the baseline. This was the reason why we used the maximal EMG activity and torque. To overcome this problem, the authors are currently trying to improve the system.
CONCLUSION
The portable hand-driven isokinetic system was designed to analyze spasticity both quantitatively and comprehensively. Using this system, we were able to detect EMG activity and torque in normal subjects without spasticity. The results were relatively smaller than that of patients with spasticity. This suggests that the portable hand-driven isokinetic system is precise enough to detect this type of delicate data. Those results are considered to be caused from the stretch reflex and viscoelastic component of muscle and joint. They could be reference data for analyzing the spasticity in the future.
 XML Download
XML Download