

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Development refers to the specialization of functions which occurs longitudinally and cross-sectionally in various areas, largely divided into gross motor skill, fine motor skill, language, adaptive ability and social skills. Developmental delay can be characterized by the lack of development appropriate for the age in each area of the specified development, causing permanent functional impairment.1 The early detection of development delay can minimize permanent disability and prevent secondary impairments, maximizing the potential that young children with developmental delay can achieve.1-3 In Korea, infant screening projects have been implemented for five sessions for four months to five years old children according to the Mother and Child Health Law and Childcare Act since 2008 by National Health Insurance Corporation. The main concern for developmental screening tests among the health screening projects is to find young children at risk of developmental delay by using screening tests that can be easily used by anyone, and not just by specialists in the areas of development. To meet this purpose, Korean Ages and Stages Questionnaires (K-ASQ), the standardized screening tool widely used in Korea and Denver Developmental Screening Test II (DDST II) have been recommended.
DDST II was developed by Frankenberg and Dodds in 1967, to assess the degree of development in young children and its revised version was published in 1992. One of the assessment tools widely used as the screening test for the developmental delay, it examines the four areas of development, social contact, fine motor skill, gross motor skill and language, and its validity and reliability have been proven by various reports.1, 4-7
K-ASQ is a parent-completed child monitoring system and original Ages and Stages Questionnaires' first edition was published based on the findings from a 20 year study by Squires and co-workers in the USA in 1995. With additional questionnaires developed in 1997, the second edition, K-ASQ complete with 19 questionnaires reflected the situations of Korea, devised by Heo et al.8,9 in 2006.
This test is cost-effective, can be filled out with reliability without special training and it is simple in scoring, which makes it advantageous because it can be used as a screening test for developmental delay in outpatient clinics. However, in Korea, studies on clinical efficacy of K-ASQ are lacking and research on the relationship of K-ASQ and other developmental tests has been limited.10,11
Thus, the purpose of this study was to analyze the concurrent validity between K-ASQ and DDST II for young children who visited rehabilitation outpatient clinics, and who were suspected of developmental delay through the comparison of screening tests. Also, the Capute scale12 and Alberta Infant Motor Scale (AIMS),13 were used to assess the clinical efficacy of K-ASQ as the screening test for the developmental delay.
MATERIALS AND METHODS
Subjects
Among children ranging from 4-months to 60-months-olds who visited the rehabilitation outpatient clinic from March to August of 2009, children for whom K-ASQ and more than one test from DDST II, Capute scale and AIMS was conducted were designated as the primary subjects. Subjects whose interval between each test exceeded 7 days were excluded from study.
Methods
This study was implemented in the retrospective chart review, and reviewed by the Institutional Ethics Committee. K-ASQ was designed to have questionnaires suitable for the age for the young children who visited the rehabilitation outpatient clinic, filled out by their parents. The criteria for developmental delay were specified as cases with less than 2 standard deviations in five areas. In DDST II, the standardized test for Korea14 was used and was conducted by three experienced occupational therapists. Children at the risk of developmental delay were specified as those that failed over 2 items in more than two categories or failed in more than 2 items in one category and failed in 1 item in another category while not passing the age lines in the same category.
Capute scale and AIMS were utilized as diagnostic tests for developmental delay and AIMS was conducted with infants under 12 months after birth. Capute scale was assessed by a pediatric physiatrist, and cutoff point for developmental delay with the basis of less than Developmental Quotient (DQ) 85 and less than DQ 75.12 AIMS was assessed by three physical therapists specialized in pediatric rehabilitation, and the reliability between the three testers was 97.7%.15 The cutoff point used for developmental delay in AIMS was at the 10th percentile.13
RESULTS
Children who had completed K-ASQ were 226 in total (119 male and 107 female), with an average age of 17.5±12.0 months (ranging from 4 to 60 months).
The comparison of K-ASQ and DDST II
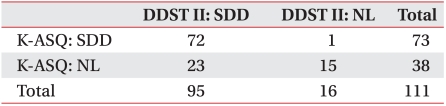
From 111 children for whom K-ASQ and DDST II were conducted simultaneously, 73 subjects were classified as children at the risk of developmental delay in K-ASQ compared to 95 subjects in DDST II. Kappa value for K-ASQ and DDST II was found to be 0.442, which is relatively high strength and statistically significant (p<0.05) (Table 1).
The comparison of K-ASQ and capute scale
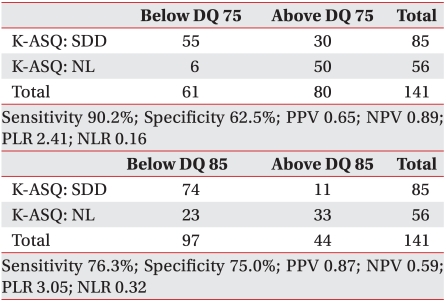
When the cutoff points were specified as less than DQ 75 in the Capute scale, sensitivity of 90.2%, specificity of 62.5%, positive predictive value (PPV) of 0.65, negative predictive value (NPV) of 0.89, positive likelihood ratio (PLR) of 2.41 and negative likelihood ratio (NLR) of 0.16 were found for developmental delay in K-ASQ (Table 2). On the other hand, sensitivity 97.0%, specificity 25%, PPV of 0.57, NPV of 0.89, PLR of 1.29 and NLR of 0.12 were found for DDST II.
When the cutoff point was specified as less than DQ 85 in the Capute scale, sensitivity of 76.3%, specificity of 75.0%, PPV of 0.87, NPV of 0.59, PLR of 3.05 and NLR of 0.32 were found for developmental delay in K-ASQ (Table 2). On the other hand, sensitivity of 95.7%, specificity of 38.9%, PPV of 0.80, NPV of 0.77, PLR of 3.40 and NLR of 0.26 were observed in case of DDST II.
The comparison of K-ASQ and AIMS
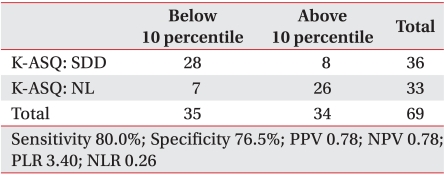
When a comparison was made between the specified cutoff points for developmental delay as less than the 10th percentile in AIMS, sensitivity of 80.0%, specificity of 76.5%, PPV of 0.78, NPV of 0.78, PLR of 3.40 and NLR of 0.26 were found for developmental delay in K-ASQ (Table 3). In case of DDST II, 92.0% and 37.9% were found for sensitivity and specificity, respectively, and PPV of 0.56, NPV of 0.84, PLR of 1.48, and NLR of 0.13 were observed.
DISCUSSION
Korea is yet to conduct research on the exact prevalence rate of developmental delay. In the US, according to research from 1997, about 17% of young children were found to display developmental delay such as cerebral palsy, visual and hearing impairment, language impediment, developmental disorders and learning disability. Among these children, less than 50% were diagnosed with developmental delay before the primary school years, and the rest were diagnosed as having lost the chance for treatments because they already had severe disabilities.16
Correlation between K-ASQ and Bayley Scale of Infant Development-II (BSID-II) by Kim and Kim10, was relatively high when BSID-II was divided into three groups, which were significant delay, mild delay and normal. The research recommends the referral for further developmental evaluation only for cases where the scores were lower than or in proximity to the cutoff points. Kim and Sung11 suggests the use of K-ASQ for screening test with negative predictive value of 92% when compared with BSID-II.
This study evaluated the clinical efficacy of K-ASQ, which can be simply conducted in outpatient situations for children with possible developmental delay and confirmed that concurrent validity for the two tests was relatively high, based on the comparative study of K-ASQ and DDST II,5,6,17-21 which has been widely used in Korea as the screening test for developmental delay.
The likelihood ratio used in this study was assessing the effectiveness of the tests. Positive likelihood ratio is a relative scale to compare people with a disorder diagnosed as positive compared to those without disorder. Negative likelihood ratio is the relative comparison on how many times people without the disorder diagnosed as negative compared to those with disorder. If only sensitivity and specificity were to be used, it is plausible that the screening test results could be interpreted exaggeratedly, and to eliminate such possibility, the likely ratio was provided as well.22
As the confirmatory test for developmental delay, Capute scale and AIMS were used in the study.12,13 Capute scale is the test developed by Arnold J. Capute from Johns Hopkins Medical School, USA, and it consists of a cognitive adaptive test (CAT) and clinical linguistic and auditory milestone scale (CLAMS). Capute scale assesses the degree of cognitive adaptive development and language development as the developmental quotient targeted for infants younger than 36 months. It is effective in development assessment of premature infants and diagnosis for developmental delay in language. Its assessment is possible in relatively short-time by experienced tester, showing high correlation with Bayley scale, which means that it can be used as a diagnostic tool for developmental delay when conducted by the specialist.1,23 In addition, in Capute scale the cutoff points for developmental delay were specified as less than DQ 85 and less than DQ 75. A child was diagnosed as normal with over DQ 85 and with apparent developmental delay with less than DQ 75.
AIMS is a test focused on gross motor skill. For infants less than 12 months of age, whose developmental assessment are difficult in other areas, overall developmental delay usually manifests as a delay in gross motor skill development. Thus, AIMS was used as the diagnostic tool for children aged 12 months or less.24-26
Since the sensitivity for developmental delay was scored lower overall compared to DDST II, young children at the risk of developmental delay in DDST II were diagnosed as normal in K-ASQ in some cases. However, a relatively high sensitivity of 76.3-90.2% overall was observed. Moreover, it was determined K-ASQ has an advantage which is that despite the test being conducted on reporting from parents, the specificity was higher than DDST II.
Furthermore, DDST II had drawbacks like having to be conducted by a trained tester and the time required for testing was longer than that of K-ASQ. K-ASQ was standardized to fit the situations in Korea. K-ASQ is advantageous in that it is cost-effective, can be filled out reliably without special training and it is simple in scoring, eliminating the need for an expert in its interpretation. Previous reports showing that parents of the children could successfully assess the development of growing children further supported the findings of this study.27
K-ASQ was designed for the selection of questionnaires for each age range, and when the age of the child was in this range, the questionnaire for younger children was used in the study. Thus there is a possibility for low sensitivity compared to DDST II which necessitates future additional research on how to improve sensitivity when using two age groups simultaneously.
This study had limitations, including not assessing screening of K-ASQ for specific disorders. Therefore, additional research would be required in the future for screening of each area of development. Another limitation of the study was that developmental delay was only fragmentarily evaluated, since long-term follow-ups were not done on children.
The study also includes cases of regular follow-ups done on premature babies based on the characteristics of the hospital. It is thought that children who have shown abnormal diagnosis using the Capute scale improved to normal at follow-up, which is the natural course for many cases of children with developmental delay.
However, the early detection of severe developmental delay, which causes functional impairment through consistent follow-up on developmental delay clinically, is crucial for the prognosis of children. Thus, K-ASQ is cost-effective and useful for repeated assessments and deemed useful for consistently monitoring developments.
CONCLUSION
Conclusions are based on results from K-ASQ, DDST II, Capute scale and AIMS on children who visited the rehabilitation outpatient clinic from March to August, 2009. K-ASQ showed relatively high concurrent validity with DDST II. Although K-ASQ showed lower sensitivity compared to DDST II, when compared with DQ 75 in Capute scale and 10th percentile in AIMS, it showed relatively high sensitivity of 80.0-90.2%. Furthermore, it showed higher specificity, PPV and PLR compared to DDST II. Therefore, it can be concluded that K-ASQ would be appropriate for consistent follow-up of children with developmental delay because of its cost-effectiveness and simplicity.
 XML Download
XML Download