

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
It is a well-known fact that chronic disease conditions such as hypertension, dyslipidemia, and obesity or diabetes mellitus pose the biggest disease burden worldwide.1) In most cases, therapeutic effects in real world practice depend on adherence, even if the efficacy has been clearly validated in scientific clinical research. For decades, the World Health Organization (WHO) has advocated for several different stages in the improvement of approaches to adherence among patients with chronic diseases.2) In the past, patients themselves were considered to be the source of non-adherence. However, in current research, the role of medical service providers has been regarded as much more important. Since the early 2000s, the need for a more systematic approach has been argued. The term systematic approach is a problem-solving paradigm that takes into consideration all the elements needed to fulfill a goal or solve a problem.2) Since there is a significant sense of blaming patients in the term compliance, the term adherence is a more accurate description of all the elements that work in a complex and dynamic process over a long period of time.2) According to the WHO, to improve adherence, a systematic approach starting with strategies to improve medical service quality and reimbursement for medical practice dispensed to solve various difficulties faced by both patients and their families is needed.2) Thus, the goal of this paper is to propose a useful starting point as the form of expert consensus to overcome the limitations of previous approaches to adherence interventions. This will be done by enumerating the variety of elements that must be included within the framework of a systematic approach to improve adherence.
The scope of this paper is for conditions that need long-term lifestyle changes or drug treatments for the primary prevention of cardiovascular diseases among those who do not experience cardiovascular complications. Because there may be greater motivations in situations of secondary prevention, especially during the early phase of complications, these ideas could also be applied to the chronic phase if a patient has no sequela or is without symptoms. In primary prevention, individuals with chronic conditions subject to cardiovascular complications must change their lifestyle habits and maintain treatments throughout life, even without current symptoms. The scope of chronic diseases defined by the WHO is much broader, but this document will be limited in scope to chronic diseases related to cardiovascular diseases.
In recent international guidelines in primary prevention field such as guidelines for hypertension, diabetes, dyslipidemia, and obesity, more and more adherence issues have been addressed.3)4) But in terms of implementation of those guidelines in real world practice, separate approaches by dozens of related academic specialties need to be integrated into a comprehensive strategy. For generating the comprehensive expert consensus dedicated on the adherence intervention, the guideline committee in Korean Society of Cardiology launched a task force for the expert consensus statements composed of the delegated members from the Korean Society of Cardiology (Seung-Woon Rha), Korean Association of Clinical Cardiology (Kyung Jin Lee, Jong Won Won), Korean Society of Hypertension (Sang Hyun Ihm, Kwang-il Kim, Jinho Shin), Korean Society of Cardiometabolic Syndrome (Sang-Hyun Kim, Hack-Lyoung Kim), and Korean Society of Lipid and Atherosclerosis (Jin Oh Na).
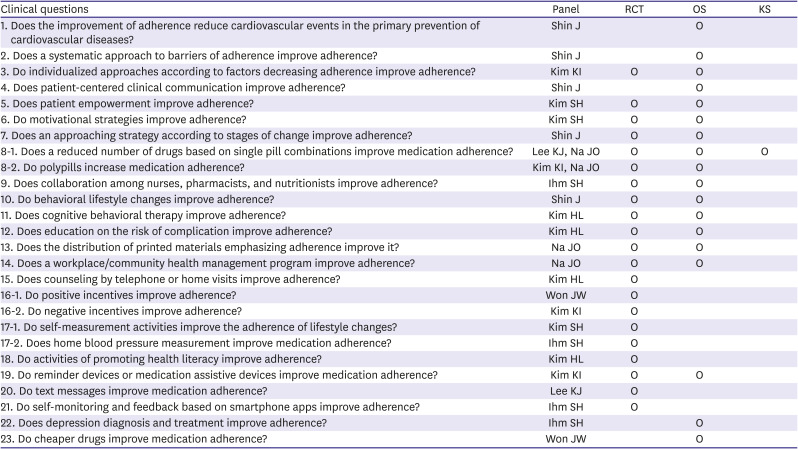
The task force concluded that, in relation to the adherence intervention for primary prevention of cardiovascular diseases, currently there is no randomized controlled trial evidences for clinical hard outcomes essential for generating the formal grade of recommendation with level of evidence. So, it was decided that the format of present report was to be expert consensus statements. Twenty-eight clinical questions for the adherence intervention for primary prevention of cardiovascular diseases were collected from the delegate from each academic society. Among them, 26 clinical questions for the manuscript were chosen unanimously by discussion at the task force meeting as shown in the Table 1. Consensus statements were drafted by the assigned panel reviewing the relevant literature as shown in Table 1. Each consensus statement was approved with unanimous agreement at the task force meeting.
Table 1
Clinical questions related to the primary prevention for cardiovascular diseases and the related studies to the evidence of expert consensus
PART 1. GENERAL APPROACHES TO ADHERENCE
Definition of adherence
At a WHO consensus meeting on adherence in 2001, it was pointed out that, in the definition of “the extent to which the patient follows medical instructions,” the word ‘medical’ was not appropriate for chronic disease conditions in which patients usually have few illnesses or discomfort, and the word ‘instructions’ emphasized the patients’ passiveness in accepting professional advice. It was argued that this definition cannot embrace the recent revision of the role of the patient as an active collaborator in the treatment process.5) In this guideline (page 18), adherence refers to “the extent to which a person carries out lifestyle changes, including medication and dietary habits, according to the agreed recommendations from a health care provider.”2) Based on this idea, adherence in primary prevention for cardiovascular diseases now can be defined as the extent to which a person’s behavior: taking medication, following a diet, and/or executing lifestyle changes, corresponds with the ‘agreed recommendations’ from a health care provider. It was highlighted that the term ‘adherence’ includes an agreement process; thus, it was differentiated from the old term ‘compliance.’ In other words, compliance is applied to treatments that are not dependent on patient consent. Thus, patient-centered clinical communication (PCCC) is essential to facilitate active collaboration from the patient and provide effective treatment for patients with chronic diseases. The quality of the therapeutic relationship between medical personnel and patients is an important element to determine adherence. An effective therapeutic relationship between the provider and the patient is characterized by a therapeutic environment that comfortably promotes 1) inquiry into alternative therapeutic means; 2) negotiations regarding prescription drugs; 3) conversations about adherence; and 4) visiting plans.
Measurement of adherence
An accurate evaluation of adherence is essential for an effective treatment plan, but there is no clear standard to measure adherence. As a result, there is a tendency to overestimate adherence in routine questions or patients’ subjective self-reports. That is, answers that suggest they are not following the instructions are accurate whereas answers that suggest they are following the instructions are inaccurate. Even standardized surveys adjusted for the patients’ personality characteristics cannot predict adherence. In addition, there is no clear evidence behind the criteria to distinguish good adherence from bad adherence. No reliable factor has been proposed to predict adherence. However, some indirect and detailed methods such as a survey on the frequency of food consumption in lifestyle changes that are needed to regulate weight can be useful for assessing adherence. The refill rates of prescriptions at pharmacies in nationwide databases may offer the most useful information, but more general methods to measure whether patients are adherent not only to medication but also to therapeutic behavior is needed.
In the clinical field, the first step in the improvement of adherence is accurate assessment. Patients with adherence issues tend to neglect or reduce it or be reluctant to give detailed explanations. Even when such data is obtained, it is not clear whether adherence is improved when measured by objective methods or drug prescription databases. For lifestyle changes in which there is a wide discrepancy in the awareness of adherence between patients and healthcare providers, some practical plans that patients can agree to as helpful for their behavioral changes could become much more effective.
In PCCC about medication adherence, it is better to stay away from direct questions to which patients can give a short answer with “Yes” and “No.” For instance, once patients respond “Yes” to a direct question of “Are you taking your medication regularly?” even though they are not, it is more likely that they will keep saying “Yes” to the following questions regardless of their accuracy, and they may deny their situation and decide to give a false answer.6) Even in the clinical research process, there has been a recent attempt to introduce the category of non-adherence to obtain standard information about adherence, but this approach is feasible only on the premise that patients give accurate information, which makes interviewing methods to determine adherence very important.6)
Effects of adherence interventions
Adherence is a basic element to determine the effects of lifestyle changes as well as drug treatment, which means that the incidence rates of complications vary according to the degree of adherence.7)8)9) Improved adherence reduces mortality and complications in the primary prevention of cardiovascular diseases.10)11) Improving adherence is cost effective by reducing the cost to treat complications and by helping patients increase their social roles and productivity through the maintenance of their health conditions. Resistance to treatment, on the other hand, weakens adherence and causes serious public health issues, including preventable early death and increasing medical expenditures.
Adherence is very low in the primary prevention of cardiovascular diseases, so there is much room for improvement. Even a small improvement can enhance overall therapeutic effects in addition to individual therapies.5)12) Medical experts and policy professionals are accustomed to making predictions for the effects of individual therapies when measuring the performance of medical policies, the utilization of resources, or the effects of interventions. To ensure the accuracy of prediction, they should be careful not to neglect many diverse issues in the course of providing necessary health management services including adherence.13)
It has been reported that low-cost interventions to improve adherence can reduce expenditures and increase the efficiency of treatment, thus possibly improving the efficiency of health policies.14) The active intervention of barriers to the improvement of adherence is the most important in population-based approaches. In the short-term, it may cause an increase in expenditures, but it is an investment in cutting high-cost medical expenditures and lowering overall healthcare costs.
As a result, a strategy to reduce the gap between therapeutic effects in clinical trials and those in real world practice and to even reduce residual risk by lifestyle changes is needed. Such a strategy would eventually increase the effectiveness of the healthcare system.
Clinical question 1: Does the improvement of adherence reduce cardiovascular events in the primary prevention of cardiovascular diseases?
Consensus: Adherence is associated with reduced mortality and complications in the primary prevention of cardiovascular diseases.
Systematic approaches
Studies since the 1990s regarding adherence improvement at the levels of healthcare providers, patients, and systematic stages have shown that increasing the awareness of behavioral styles of patients and healthcare providers and awareness of the problems of the medical system is effective. Therefore, a systematic strategy that encompasses all healthcare providers, patients, and policy makers is mandatory to improve adherence. An approach using a multidimensional context is also important to help patients maintain their health behavior in the long-term.
Factors influencing adherence
There are 5 major groups of factors that influence adherence: 1) socioeconomic factors; 2) factors related to the healthcare system and treatment teams; 3) factors related to the attributes of treatment; 4) factors related to health conditions; and 5) patient factors. Factors related to the healthcare system and treatment teams in connection to the primary prevention of cardiovascular diseases include poor insurance systems, poor quality of education for healthcare personal, overworked medical practitioners, short consultation time, absence of evaluation or reward systems for medical practice, lack of cooperation from the community, absence of self-management programs, and poor management for adherence. Factors related to the attributes of treatment include the complexity of prescriptions, long durations of treatment, experiences of treatment failure, frequent changes in prescriptions, long periods before the manifestation of therapeutic effects, and side effects. Factors related to health conditions include mild or no symptoms, absence of physical, psychological, or social disabilities, and the slow progression of diseases. These characteristics have grave effects on a patients’ awareness of risks and the priority of treatments in the primary prevention of cardiovascular diseases.2) A stronger rapport between a patient and healthcare professional has been found to improve adherence.15)
Patient factors include knowledge, attitudes, beliefs, awareness, and expectations. There is a complex interplay among motivations for treatment, self-efficacy to continue therapy, and expectations for the outcomes of therapy or non-adherence. Other patient factors include forgetfulness, stress, anxiety about side effects, low levels of motivation, lack of knowledge or ability for symptoms or treatments, low self-awareness for the need of treatment, ignorance about therapeutic effects, negative beliefs about therapeutic effects, misunderstanding or disregard of the disease, doubts about the diagnosis, neglect of risk, misunderstanding of treatment protocols, rejection of consistent visits, low expectations for therapeutic benefits, failure to frequently visit, frequently being absent from educational programs, despair or negative emotions, disappointment with medical professionals, fear of dependence, anxiety over complex prescriptions, and labeling effects.2)
Awareness of the need for drug treatment is affected by the symptoms themselves as well as awareness of risk.16) Diseases related to the primary prevention of cardiovascular diseases have few symptoms and take a long time before the manifestation of complications or therapeutic benefits. This creates major disadvantages in awareness of the need for drug treatment. There can also be a strong abstract concern about the side effects of medication, such as misconceptions of side effects, burden of having to take medication every day, and/or drug dependency during long-term treatment.17) These views can foster negative attitudes about all types of drugs and may be associated with broader caution or doubts about chemicals detected in food or the environment resulting in further generalized suspicion of science, medicine, or technology itself.18)19)20)
According to the WHO, healthcare systems have an influence on adherence. The control of consultation time, distribution of resources, medical reimbursement systems, communication, and information systems can have impacts on accessibility to medical services. A desirable system has the following attributes: healthcare providers are given enough time to support behavior related to adherence; threats to patient interviews or education due to the lack of reimbursement are improved; resource distribution that can lower adherence by too many requirements and stress from healthcare providers is improved; continuous treatment from the same provider is received; data on prescriptions between doctors’ offices and pharmacies is shared; and ongoing counseling, including contact by phone call, is encouraged. Unless these systematic requirements are met, it will be limited for healthcare providers and patients to achieve adherence due to suppression from external factors.
The WHO report recommends that policy authorities set a policy goal of improving adherence and play a central role in adherence issues as they are related to the efficiency of the healthcare system as well as the health of the population. There are 5 issues concerned with adherence with respect to policy making: 1) lack of awareness and ignorance with regard to adherence; 2) lack of clinical tools to assist medical personnel to evaluate and intervene adherence issues; 3) shortage of behavioral tools needed to change negative behavior as well as promote positive ones; 4) a gap in rewards for the treatment of chronic diseases; and 5) lack of communication between patients and medical personnel. These issues can be solved by developing accurate evaluation tools for adherence and identifying factors influencing it. Healthcare providers play important roles in the improvement of adherence and in reasonable interventions at the healthcare system level which can, in turn, have impacts on their behaviors.
Even with the best coping measures at the healthcare system level, it is not sufficiently effective at the social level. The social ecological model raises the need for systematic changes that are broader and more diverse than just families and schools in order to maintain healthy behavior for a long period of time. Factors influencing patients’ behavior in the ecological aspect include personal, interpersonal, organizational, community, and public policy factors. There should be measures across all these areas. A recent emphasis on social context proposes an approach of intervening behavioral changes through the organized fusion of community situations, the government, and policies in addition to the healthcare system.
Importance of systematic interventions in the 5 areas
It is critical to take a systematic approach to assessing potential barriers to interventions for improved adherence while identifying factors causing inconvenience. In general, it is because of dependence on fragmentary approaches that adherence issues are not resolved. In many cases, only single dimension approaches limited to patient factors have been taken. It is common to use self-management programs that are known to be effective,21)22)23) intervention programs by nurses, pharmacists, and experts of other medical backgrounds,24)25)26) counseling,27)28) or behavioral interventions, follow-up, and reminders29) separately. However, considering the interactions among these factors, the effect is very likely to be limited if only used separately.
A multidimensional team intervention seems to be the most effective. This team approach, for instance, has been reported in Multiple Risk Factor Intervention Trial and The Hypertension Detection and Follow-up Program research. An innovative and advanced medical service team has been found to be more effective than conventional therapy by doctors alone and minimally structured methods.30)31)
2) Medical teams and healthcare interventions
Healthcare providers should receive specialized education about the management of adherence, and a system should be established to plan and provide it. There should be training regarding the 3 major topics in order to reinforce the capabilities of medical personnel by a counseling tool set on adherence: first, information about adherence; second, effective uses of information about adherence and frameworks for understanding it; and third, behavioral tools to form and maintain therapeutic behavior. In such education, behavioral tools based on educational strategies at least should include a role play for them to be applied for clinical and community practice.38)39)40)41) The key determinants of adherence are how healthcare providers interact and communicate with the patient. Provider behaviors that positively correlate with long-term adherence are 1) communication styles asking patient specific questions about adherence followed by informing them using positive talk; 2) continuity of follow-up; 3) involvement of the patient in the care process and building partnership; 4) warmth and empathy with emotional support; 5) patient satisfaction with the medical regimen. Provider barriers are giving limited information, lack of skills in motivational interviewing, lack of knowledge, and frustration experience in teaching patients. Structured, thoughtful, and sophisticated interactions are essential.
3) Treatment-related interventions
Doses, administration frequency, and side effects of drugs are major issues related to treatment and require close cooperation with pharmaceutical companies and research activities.
4) Disease-specific interventions
Disease-specific requirements, symptoms, or disabilities can be major objects of interventions in secondary prevention situations, but many risk factors related to the primary prevention of cardiovascular diseases are a weak motivation for patients in their treatment from the perspective of symptoms and disabilities. Thus, it is very important to understand the patients’ perspective regarding the risk factors.
5) Patient-related interventions
Major issues include a lack of information and skills needed for self-management, difficulties with motivation and self-efficacy, and lack of assistance for behavioral changes. These issues hold special importance for lifestyle changes. They are also important for drug adherence. Although it is known that education alone is not sufficient, many interventions designed to encourage adherence continue to depend on conventional patient education without motivational strategy. Instead, patients should be educated to obtain the correct information, motivate themselves, and make good use of cognitive or behavioral self-regulation strategies.
There should be an ongoing effort to provide patients with pertinent instruction, but it is most important to motivate them to take a long-term perspective as it is the driving force in the improvement of adherence.
Clinical question 2: Does a systematic approach to barriers of adherence improve adherence?
Consensus: A systematic approach to barriers of adherence can improve adherence.
Individualized approaches
When customized approaches for patients were applied during interventions, patients improved in medication adherence.42) Meta-analysis results also showed that customized approaches for patients improved medication adherence.43) Real barriers to patient adherence include lack of skills and information for self-management, absence of motivation and self-efficacy, and lack of support for behavioral changes. This applies to drug therapy such as the number of pills and the presence of comorbidity,44)45) but it is even more important for lifestyle changes. Conventional education can result in weak effects, but it could be enhanced by motivational strategies. Patients need motivation in addition to simple information and should be accustomed to making use of cognitive and behavioral self-regulation strategies. Given the attributes of primary prevention of cardiovascular diseases, one of the biggest difficulties in the healthcare system is to ensure ongoing provision of information over a long period of time and motivation to drive an adherence state. In the domain of chronic diseases involved in the primary prevention of cardiovascular diseases, it is important to improve adherence through the motivation and promotion of self-management. Since it is difficult to consistently motivate patients about chronic diseases through the healthcare system or medical professionals, there is growing interest in education and self-management programs based in the community.
Risk factor-specific strategies
1) Smoking
There are many different approaches to effective smoking cessation. PCCC techniques and related guidelines for smoking cessation programs developed by Ockene et al.41) are widely known. They can be summarized as follows: 1) All subjects should recognize the risk of smoking through posters and printed materials in the waiting area; 2) they should be asked about their smoking habits at every visit; 3) there should be exploratory interviews about elements that hinder or support smoking cessation; 4) there should be compromising and goal-oriented interviews according to the patients’ level of knowledge, stages of change, and elements that hinder or support their smoking cessation; 5) drugs used in nicotine dependence products, such as nicotine patches, gums, inhalants, and drugs with proven effects should be taken into consideration during interview therapy; and 6) follow-up visit plans should be made to discuss the progress that patients have achieved in relation to smoking cessation.
2) Hypertension
Drug adherence has been improving, but it is still low among hypertension patients. Evidence-based suggestions recommend an examination of patient beliefs and concerns by multi-disciplinary teams, tracking observation, feedback, and free medication therapy programs. The treatment guidelines should be followed in the treatment process for their diseases with comprehensive lifestyle changes.4)46)47)
3) Meals/dyslipidemia
Recent guidelines suggest that multidimensional interventions are effective for patients with a risk of coronary artery diseases including dyslipidemia. These can be summarized as follows: 1) evaluation of saturated fatty acid and cholesterol intakes; 2) meal guidelines emphasizing a balanced diet through various educational materials including pamphlets and printed materials; 3) educational materials about low fat dairy products, lean meat, low fat processed meat, and low fat cooking to reduce saturated fatty acid in purchasing and cooking food; 4) reflection on the stages of change and degree of motivation; 5) individualized nutrition counseling and lifestyle changes by nutritionists to achieve a low-density lipoprotein-cholesterol (LDL-C) level within an acceptable scope; and 6) reinforcement of diet principles according to follow-up LDL-C changes.
4) Obesity
In a primary care environment, the most important issue with being overweight and obesity is to monitor weight. Burke48) reported that consistent contact between medical personnel and patients improves weight maintenance the most. Following this observation, regular physical activities are essential for long-term weight maintenance. A management program with social support is even more effective. These findings indicate that reducing obesity needs to take approaches similar to other chronic conditions and to ensure continued observation, reevaluation, and reinforcement.
5) Diabetes
All the recommendations related to meals, obesity, and physical activities are applied in cases of diabetes.
6) Physical activities
Patient-centered evaluation and interview programs using interactive information and bidirectional communication technologies related to physical activities and nutrition have been reported. The minimum requirements are the following: 1) regular physical activity through history taking about physical activities; 2) pamphlets and printed materials about the general principles of physical activities; and 3) moderate physical activities for 30 minutes every day.49)
7) Medication
Those who give drugs to patients are basically recommended to have counseling with their patients about their drug adherence state and to bring the remaining drugs. Adverse drug effects and resultant psychosocial responses of the patient should be closely followed and monitored.50)51) There are many different ways that are known to increase medication adherence for cardiovascular diseases: 1) oaths; 2) behavioral skill training; 3) self-monitoring; 4) contact by phone call/mail; 5) support from a spouse; 6) promotion of self-efficacy; 7) conditional contacts; 8) short-term exercise prescription; 9) external cognitive assistive tools; 10) persuasion; 11) workplace consultation; 12) nurse management and intervention; 13) education and meal programs by a school unit; and 14) the strategies in Table 2.52)
Table 2
Practice items to improve adherence for prevention and treatment recommendations
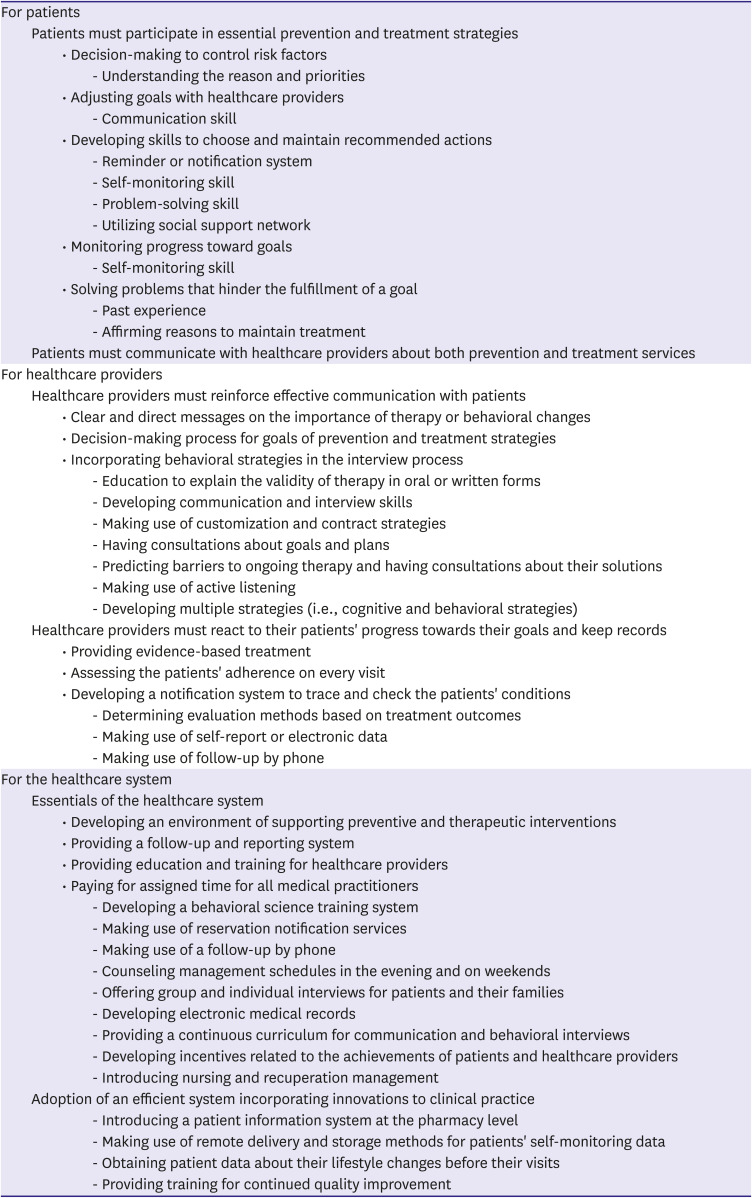
Adapted from reference.79)
Clinical question 3: Do individualized approaches according to factors decreasing adherence improve adherence?
Consensus: Individualized approaches customized for each patient improve drug adherence for the primary prevention of cardiovascular diseases.
PART 2. SPECIFIC INTERVENTIONS FOR ADHERENCE IMPROVEMENT IN PRIMARY PREVENTION OF CARDIOVASCULAR DISEASES
The primary prevention setting itself is a challenging factor to be overcome in improving adherence. In most cases of primary prevention of cardiovascular diseases, patients should follow a nonpharmacological or pharmacological therapy for life despite not having any uncomfortable symptoms in relation to their risk factors, which means that very low adherence is likely. In cases of hypertension, dyslipidemia, and diabetes, medication adherence continues to drop after the start of therapy and stays within a range of 20–60% in one year of therapy.53)54) Therefore, it requires a different strategy from an acute strategy for a patient with cardiovascular complications. Eventually, a comprehensive strategy similar to the primary prevention setting may be required so that adherence can be maintained in long-term therapy.55) To overcome the 2 unfavorable conditions, i.e., lifelong therapy and no symptoms, the most important approach is patient-centered. Effective intervention for adherence is specifically important to clinically implement the recent trends of earlier interventions in younger and middle-aged patients.
Development of individual capabilities of the physician
Patient-centered clinical communication
Since the 1990s, the transtheoretical stage of change models has been applied in research and therapy with a focus on behavioral changes at the individual level. This approach can be applied to many different theoretical models simultaneously. A synthetic application to PCCC is helpful for the improvement of adherence. Here, application means “to have patients get involved and help them make a therapeutic plan and stick to it.”56)57)58) In PCCC, the following types of questions are asked: 1) open-ended questions to induce patients in a decision-making process; 2) questions about the patients’ thoughts about risks; and 3) questions that enable a comparison between the costs and benefits in behavioral changes and adherence. These questions cover the 5 areas for a time efficient application of PCCC: 1) whether patients have the desire or motivation to change their behavior; 2) whether they have had experiences of attempting behavioral changes in the past and what their experiences were; 3) what hindered their behavioral changes; 4) what they think about their surrounding conditions and abilities for behavioral change; and 5) plans for behavioral change and times of revisits. It has been emphasized that past experiences should be utilized to facilitate the motivation and efficacy patients. In PCCC based on the health belief model, records are made of 1) the patients’ cognitive states to the risk of their behavior and deteriorating diseases; and 2) the patients’ beliefs about their behavioral changes to lower the risk. In the relapse prevention model, education and tools to determine the characteristics and clues of high-risk situations should be provided. Patients should be equipped with coping methods for each situation in detail including communication, initiation of support, and stress management methods. Well organized PCCC should be sequentially progressed in the following steps.
1) Creation of a therapeutic environment
As far as adherence is concerned, patients should be helped, not blamed. Non-adherence is a normal phenomenon. The desired therapeutic environment should be non-judgmental, empathic, genuine, curious, and collaborative. This is critical because the biggest predictor of motivation for behavioral change has been found to be the interviewer’s interview method.59)
2) Initiation of questions
The interview should let patients know that non-adherence is a natural phenomenon (A) and consent should be received to talk about adherence with them (B). For instance, “Many people have a difficult time getting all the drugs they need and taking them all the time (A). It is very important how you take your medication in order to make a safe and effective drug therapy plan. How about talking about this issue for a moment (B)?” From a comprehensive standpoint such as “What do you want to talk about today?”, however, inducing patients to decide on the interview topic itself is more patient-centered. This is because patients who have low medication adherence may not want to talk about it.
3) Specific interview progress
Examples of desirable questions regarding medication include “How many times did you miss your medication last week, including the weekend?” and “What was your medication percentage for the last month? If you took your medication regularly, it is 100%. If you took your medicine half the time, it is 50%” so that the patients cannot answer with “Yes” or “No.” Following the patients’ answers, the interviewer may ask an additional question such as “Have you ever suspended or started your medication according to your own judgment?” Follow-up questions for reinforcing emotions may include “What was helpful in getting you to take your medication?” Follow-up questions related to disability factors may include “What makes it difficult for you to take your medication?” or “On which days did you forget to take your medicine?” or “How did you feel about your medication on that day?” If a patient has ambivalence, exploratory questions may follow “For what reason did you decide not to take your medicine?” or “What made you take your medicine?” This process helps patients figure out and reflect on their viewpoints about their medication. Questions about their understanding of medication adherence can also be asked for motivation and education purposes. For example, “We have discussed methods to help you take your medication regularly. If you could tell me about your medication plan from now until your next visit, it will be helpful for me to see if I did a good job in explaining it to you.”
4) Wrap-up of an interview
The interviewer should wrap-up an interview by summarizing the patients’ viewpoints related to his or her symptoms or plans and by offering encouragement and reinforcement about their ideas for improvement. For example, “We have talked about taking your medication regularly for a while. I recommend you take your medicine as prescribed. It is the most effective way to prevent any potential problems as well as manage your disease. Of course, it is entirely up to you whether you take your medicine or not. If you decide to carry out the plan we’ve covered today, you will be able to find a good implementation method for yourself.”
Clinical question 4: Does PCCC improve adherence?
Consensus: PCCC improves adherence in the primary prevention of cardiovascular diseases.
Empowerment
Empowerment is allowing patients to control their own situations and exercise their rights in order to take care of themselves and maximize their individual quality of life. The WHO defines empowerment as “a process through which people gain greater control over decisions and actions affecting their health” and it should be seen as both an individual and a community process (page 16).60) In terms of the primary prevention setting, it means that patients should gain more control over the shared decision-making process as well as actions related to lifestyle changes. There are 5 dimensions of adherence factors, and the other factors of adherence are neglected in the actual field of treatment with the tendency to continue labeling patient factors as causes of non-adherence. According to research findings, however, patients get frustrated when they are not encouraged to voice their opinions and have them reflected in the decision-making process about their treatments. The more they feel they are not given any decisions of authority, the more negative their attitude will become towards therapy and their adherence is likely to be lower.61) Adherence has something to do with an individual patient’s way of judging the potential side effects and need for therapy.19)62) It is helpful to explore the patients’ major beliefs regarding their concerns and need for therapy, listen to their concerns, and help them become clear in understanding their ideas about decision-making and adherence. Empowerment helps to improve adherence in drug therapy to regulate the risk factors of cardiovascular diseases.4)
Clinical question 5: Does patient empowerment improve adherence?
Consensus: Patient empowerment improves adherence in the primary prevention of cardiovascular diseases.
Motivational strategies
The patients’ motivation for adherence is influenced by the unique values they give adherence and their views on its efficacy.63) Motivational interviews are effective in facilitating lifestyle changes to manage risk factors.64) The clear goal of behavioral therapy to improve overall adherence is to establish an internal motivational state by reinforcing the patients’ awareness of the importance of adherence and their efficacy about their self-management abilities.59) In motivational interviews, motivational strategies can help patients move to therapeutic behavior by examining their motivational state and giving them feedback based on PCCC. Motivational strategies are also valid in changes to the patients’ habits, lifestyles, or attitude towards medication.4) Structured training for motivational strategies has not been well implemented but seems to be important to assure the quality of PCCC.65)
Clinical question 6: Do motivational strategies improve adherence?
Consensus: Motivational interviews are effective in facilitating lifestyle changes to manage risk factors.
Behavioral changes and transtheoretical stages of the change model
There is no doubt that the improvement of adherence is a continuous and dynamic process. There is a misconception that patients are naturally motivated and follow the best therapy. In real treatments, it is common for clinical specialists to prescribe one-sided intervention attempts or treatments off the target to patients who are not yet ready.2) There is the usual focus on education to increase knowledge to improve adherence, but knowledge alone is not enough to create and maintain good adherence. Thus, it is necessary to make a shift from the provider’s perspective that is oriented toward complex and detailed therapies to the patient’s own perspective, for instance, educating patients in how they should respond for their specific needs.
The transtheoretical model in stages of changes reflects the need for a specific intervention according to the stages of a certain behavior. The stages are as follows: 1) Pre-contemplation stage: patients have no intention to change a certain behavior; 2) Contemplation stage: they are considering behavioral change but are not prepared to start it; 3) Preparation stage: they are willing to start a behavioral change within a couple of months; 4) Action stage: they have actually started to change their behavior; and 5) Maintenance stage: they have implemented a change and strategy to prevent a relapse. These stages can be applied to various behavioral models. Clinical specialists should implement the proper method to establish the patients’ current stage of change and help them make sequential changes. Forced encouragement or advice can be effective for patients at the action stage, but it may cause resistance in patients at the pre-contemplation stage, in which an interview with a focus on the provision of information and a focus on motivation will be helpful in a PCCC environment.66)67) Transtheoretical model was effective for smoking cessation and its efficacy for weight reduction was proved by randomized trial.66)68)
Clinical question 7: Does an approaching strategy according to stages of change improve adherence?
Consensus: Interview strategies according to stages of change improve adherence.
Drug prescription strategies
It is known that the complexity of prescriptions involving the total number of drugs and frequency of medication usually lowers medication adherence in drug therapy for cardiovascular diseases.69)70) It has been reported that taking medication once a day increased adherence with regards to the frequency of the medicine.71)72) In hypertension therapy, single pill combinations increased medication adherence and decreased the risk of lower adherence more than the conventional combination therapy.73)74)75) Single pill combinations increased medication adherence partly because they were cheaper than combination therapy.76) It is expected that an increased number of drugs will drop adherence, but research has reported that patients who felt that their illness was serious tended to take their medication better to a certain extent even with increased drugs. A study reported that adherence was the highest when patients took 4 to 5 drugs.77)
Polypill refers to a single pill of heterogeneous medicine for 2 different diseases or more such as hypertension and dyslipidemia. It has been reported that polypills improve medication adherence and are effective for the primary and secondary prevention of cardiovascular diseases.78) Meta-analysis results show that polypill prescriptions improved medication adherence for blood pressure, cholesterol, and antiplatelet drugs.79) They have especially improved cholesterol treatment in low-income countries and socioeconomically alienated classes.80) Polypills have advantages of improving adherence, being advantageous for the management of risk factors, and increasing the quality of life. They also have a couple of disadvantages, including difficulties with the regulation of dosage and possibilities of increased dosage. However, the efficacy for long-term prognosis needs to be proved.81)
Clinical question 8-1: Does a reduced number of drugs based on single pill combinations improve medication adherence?
Consensus: A reduced number of drugs based on single pill combinations improves medication adherence.
Clinical question 8-2: Do polypills increase medication adherence?
Consensus: Polypills improve medication adherence.
Development of the capabilities of treatment teams
Effects of multi-disciplinary treatment teams
In its preventive cardiology report in 2002, the American Heart Association put a major emphasis on the active role of patients as well as the practice of the healthcare system for improved adherence (Table 1). Doctors, nurses, pharmacists, and physician assistants should all practice the key concepts of 1) PCCC, 2) interview or counseling, and 3) behavioral science so that patients can perform their roles. As health education nurses, nutritionists, and psychology counselors are added to the group of healthcare providers, adherence can be promoted through education, motivation, monitoring, and feedback.82) In metabolic syndrome patients, collaboration between nutritionists and physical therapists improves adherence in lifestyle changes.83) Collaboration between nutritionists or pharmacists and nurses improves the adherence of cardiovascular and hypertension therapy.84)85)86)87) A total approach through diverse collaborations in the clinic improves the adherence of a program for lifestyle changes.88)
Under specific strategies to develop systematic team approaches to provide therapy to improve adherence, clinical specialists should receive specific education on adherence intervention. The healthcare system should also plan and deliver a corresponding medical service. If there are no established training sets of clinical skills applied broadly in actual therapy, a team approach will not be effective, even with a well-established program as long as it is not dedicated to adherence intervention. That is, one of the major issues in current education is that the efficacy of treatment proven in clinical research is not implemented in real world practice due to the lack of an educational strategy for healthcare personnel to contribute team approaches to improve adherence.
It is therefore urgent to develop a “PCCC training tools set for adherence improvement” that will assess adherence systematically, propose an intervention plan, and promote effective follow-up through the well-developed capabilities of healthcare staff. Such education for healthcare personnel should include 3 topics. The first topic is information about adherence: 1) factors and intervention methods affecting adherence; 2) dynamics and economics related to adherence; and 3) behavioral mechanisms to determine patient factors related to adherence. The second topic describes how to effectively make use of clinical information regarding adherence improvement and how to think about strategies for evaluating and facilitating changes. With such education, healthcare providers should be able to explain 1) interview methods to assess adherence, 2) learn from local factors and interventions, 3) choose the best intervention, and 4) assess the progress and follow-up. The third topic should cover behavioral tools that develop and maintain lifestyle changes. Medical experts should be trained for each element of these tools with role play and pedagogical strategies; consequently, they should be able to confidently apply behavioral tools to improve adherence to daily practice.
Clinical question 9: Does collaboration among nurses, pharmacists, and nutritionists improve adherence?
Consensus: A multi-disciplinary team unit approach involving nurses, pharmacists, nutritionists, physical therapists, and behavior therapists improves the adherence needed in the primary prevention of cardiovascular diseases.
Behavioral approaches
Various behavioral lifestyle changes improve adherence for the primary prevention of cardiovascular diseases.3) Psychological/behavioral theoretical grounds related to adherence have been established. The basic foundations for approaches related to adherence include theoretical concepts and behavioral change models such as 1) transtheoretical theory and the stages of change model; 2) health belief model; 3) social cognitive theory; 4) relapse prevention model; and 5) social ecological model.89)90)91) The 5 stages of change are the 1) pre-contemplation stage, in which patients do not take changes into consideration; 2) the contemplation stage, in which they are considering changes but are not prepared to act; 3) the preparation stage, in which they are ready to act within a couple of months; 4) the action stage, in which they are showing behavioral changes; and 5) the maintenance stage, in which they implement measures and strategies to prevent a relapse. This model can be applied in combination with other models. Clinical specialists’ encouragement policies may be effective for patients at the action stage, but patients at the pre-contemplation stage may reject them. Clinical specialists need to encourage their patients’ step by step development by taking an approach that fits each of their stages of change. Neither clinical specialists nor patients should be discouraged or alienated at any of these stages.82)
The health belief model is useful for exploring the beliefs of individual patients regarding factors influencing the possibility of behavioral change. Within the larger framework where the possibility of behavioral change is determined by an individual patient’s perceptions of 1) their health conditions; and 2) gain and loss according to behavioral change, such sociodemographic features as race, personality, socioeconomic background, and health knowledge have impacts on their perceptions. Patient perceptions of severity and risk affect their perceptions of their health conditions. In chronic diseases, cues from symptoms play weak roles, whereas cues from education and media information play more important roles.
Social cognitive theory emphasizes interpersonal, cognitive, and environmental impacts on patient behavior and the ways they are applied to behavioral change. The basic elements of a self-management program applicable to cardiovascular diseases include self-observation and analysis of behavior, self-management including external stimuli, training for behavioral know-how, behavior substitution, and behavior reinforcement. In social cognitive theory, self-efficacy is related to motivation, which is the patients’ willingness to participate in their behavioral change. A wide variety of specific methods related to behavioral change are applied in practice. Examples of external cognitive assistive tools include written contracts, training for behavioral know-how, self-supervision, reinforcement of self-efficacy, spouse and social support, contact by phone call/mail, and notifications or messages.
In the relapse prevention model, a relapse is considered a stage of behavioral change. An early relapse state is a turning point between regression to old behavior and positive changes. A relapse goes through an emotional, conscious, and physical relapse stage and is influenced by various factors, including self-efficacy, predictions for outcomes, desire, motivation, coping abilities, emotional states, and interpersonal relationships. Therefore, patients need to master know-how to recognize the cues and characteristics of high-risk situations. It is critical to make a detailed plan to cope with a situation including communication, mobilization of support, and stress management.
In the social ecological model, the emphasis is on changes across the social system encompassing the individual, interpersonal, collective (school and workplace), community, and public policy levels since interventions at the healthcare system level will not guarantee consistent effects long-term. For the promotion of physical activities, for instance, several components of an urban environment should be taken into consideration, including safe pedestrian pavements, parks, spaces for leisure, and nighttime lighting.
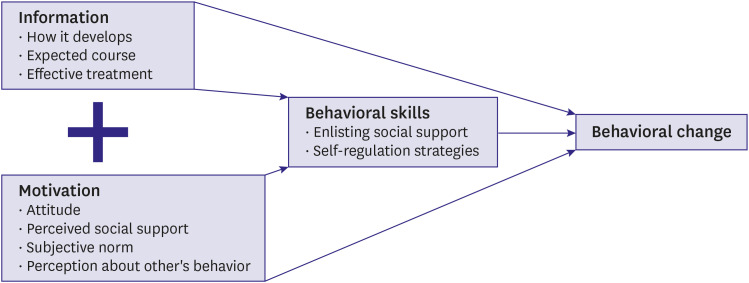
The information–motivation–behavioral skills model shown in Figure 1 is a useful conceptual framework to guide thinking about complex health behaviors. In both prospective and correlational studies, the construct of information, motivation, and behavioral skills can explain 33% of the variance in behavioral change.92)93)
Figure 1
Information–motivation–behavioral skills model. The correlation between the information and motivation is weak. Strategic approach to link information and motivation is needed. And the presence of both information and motivation increase the likelihood of adherence or behavioral changes. Modified from reference.2)
Clinical question 10: Do behavioral lifestyle changes improve adherence?
Consensus: Various behavioral lifestyle changes improve adherence for the primary prevention of cardiovascular diseases.
Cognitive behavioral therapy
Various behavioral therapy strategies including skill training for cognitive behavioral therapy to improve adherence in the management of cardiovascular risk factors have been found to be effective.52) Cognitive behavioral therapy via telephone counseling improves the patients’ lifestyle changes and lowers their risk of cardiovascular disease.94) Cognitive behavioral therapy via telephone counseling, smartphone, internet, and education improves the adherence of medication and adherence of lifestyle changes in hypertension patients and increases their blood pressure control rates.95)96)97)98)99) A doctor’s strong and clear advice for smoking cessation increases the patients’ success rate to quit smoking more than his or her suggestions.100)
Clinical question 11: Does cognitive behavioral therapy improve adherence?
Consensus: Cognitive behavioral therapy improves adherence for the regulation of cardiovascular risk factors.
Education on complications
When hypertension patients are not correctly aware of the risks of cardiovascular events, their adherence drops.46) Education on the disease enhances medication adherence and leads to better blood pressure management.11)24)101) Home visit education for the elderly with diabetes can improve medication adherence.24)102) When patients believe that blood pressure drugs are not effective for lowering their blood pressure or have prior knowledge of their side effects, it can reduce their medication adherence.64) Education that emphasizes only the risk of the disease generates small effects on the improvement of adherence, even when the effects of education are recognized. Education on the awareness of risk alone is not sufficient to increase adherence. Therefore, multi-disciplinary and multidimensional approaches should be combined to improve adherence.46)103) It is more important to educate patients according to their immediate interests using acceptable approaches than to emphasize potential cardiovascular events in 5 or ten years to improve adherence.46)
Clinical question 12: Does education on the risk of complication improve adherence?
Consensus: Education on the risk of complications improves adherence.
Printed materials emphasizing adherence
As part of a national health program to prevent non-contagious diseases, leaflets containing behavioral information for health promotion were distributed and examined for their effects. The results show that such leaflets generated no significant effects. People had no interest in such leaflets, and although such leaflets could help with their decisions, they did not change their actual behavior.104)
Clinical question 13: Does the distribution of printed materials emphasizing adherence improve it?
Consensus: Printed materials about behavioral reinforcement for health promotion have limited effects on adherence.
Healthcare system factors
Workplace or community health management programs
In education on the reduction of cardiovascular risks for African Americans with a cardiovascular disease or risk, additional participation in a church music program (for example, gospel hymns) helped them to participate in health education longer and improved their health.105)
Clinical question 14: Does a workplace/community health management program improve adherence?
Consensus: A workplace/community health management program improves adherence.
Close monitoring
A 1-hour session of telephone counseling once a week over 6 weeks can improve patient lifestyle changes and lower their cardiovascular risk.94) When nurses used phone calls for diabetes patient education, lifestyle changes, and drug regulation, patients improved in the adherence of dietary habits and self-measurement of blood glucose, and regulated their blood sugar level better.106)107) Regular phone calls to hypertension patients can improve their adherence to medication and lifestyle changes and lower their blood pressure95)108)109)110) and further save hospital and medical expenditures.110) When such phone calls stop, however, the effects dwindle or disappear.108)109) A home visit program at an interval of 2–4 months for elderly patients with hypertension improved their knowledge of hypertension, blood pressure monitoring, and adherence in meal regulation and medication.111) In elderly patients with diabetes, education via home visits and activities to increase their awareness of diabetes improved their adherence of taking drugs for diabetes.24)102)
Clinical question 15: Does counseling by telephone or home visits improve adherence?
Consensus: Counseling or monitoring by telephone or home visits improves adherence.
Monetary incentives
Incentives did not lead to a huge improvement of health outcomes in relation to chronic diseases or an increase in health-oriented behavior.112)113) There was no improvement in adherence in studies for prevention programs, medication adherence, or treatment for diabetes.113)114)115) However, a study reported significant efficacy of lottery-style incentives on weight reduction in a short-term period.116) Positive incentives did not show statistically significant differences in medication adherence. Further studies on more diverse groups and drugs are needed.117) Incentives offered both to doctors and their patients were more effective for reducing lipid level.118) Monetary incentive rewards could be effective for weight regulation and physical activities. Negative incentives were more effective than positive incentives, and group-based incentives were more effective than individual incentives.119)120)
Clinical question 16-1: Do positive incentives improve adherence?
Consensus: Incentives offered to patients did not improve adherence in the primary prevention of cardiovascular diseases.
Clinical question 16-2: Do negative incentives improve adherence?
Consensus: Negative incentives were effective for weight regulation and improved adherence in physical activities.
Patient-related factors
Self-management programs
Meta-analysis results show that the self-measurement group showed an increased amount of physical activity compared to the control group.121) Self-measurement was effective for diet control when it was combined with other measures. It was more effective when patients were young, with higher level of education, and were positive.122) Self-measurement activities were helpful for interventions based on lifestyle changes and showed greater benefits when accompanied by other interventions such as counseling.123) However, in diet therapy, self-measurement for the sodium/potassium ratio in urine did not show a benefit.124) In hypertension patients, self-measurement of blood pressure improved medication adherence without improved adherence in lifestyle changes.125)
Home blood pressure measurement improves medication adherence126) and increases blood pressure control rate.109)127) In a high-risk cardiovascular group, the self-titration of dosage of antihypertensive drug according to measured home blood pressure level improved medication adherence and hypertension control rates.128)
Clinical question 17-1: Do self-measurement activities improve the adherence of lifestyle changes?
Consensus: Various self-measurement activities improve the adherence of lifestyle changes.
Clinical question 17-2: Does home blood pressure measurement improve medication adherence?
Consensus: Home blood pressure measurement improves medication adherence.
Health literacy
There are many patients who have low health literacy in real world practice. Low health literacy is common among elderly patients.129)130) Low health literacy weakens health conditions131) and increases hospitalization rates and management costs.132) Patients with low health literacy have a weak awareness of their diseases, suffer difficulties in communicating with medical personnel, are not good at following the doctors’ instructions, and have decreased adherence for medication and lifestyle changes.131)133)134)135) Poor health literacy resulted in poor regulation of blood pressure136) and blood sugar137)138) and greater possibilities of failure in smoking cessation139) and weight control.140) When patients with low health literacy were served by patient-centered drug labeling using prioritizing information, larger font size, and increased white space with standard medication intervals, adherence of taking medications for hypertension and diabetes increased 4 to 5 times.140) When flashcards or smartphone videos were used for patients with low health literacy, medication adherences of hypertension, diabetes, and heart failure were improved.141) Multifaceted approaches encompassing communication, education, reinforced social activities, and economic support can improve adherence with greater effects on patients with lower health literacy.134)142)143) The utilization of health information technologies, such as mobile apps, can improve the patients’ health literacy and adherence.144) When treating patients with low health literacy, medical personnel should give explanations loudly, clearly, and slowly, in bigger fonts, and make active use of pictures or videos.134)135) Patients should be assessed for their health literacy every 4 to 6 years to maximize the preventive effects for cardiovascular diseases.134)
Clinical question 18: Do activities of promoting health literacy improve adherence?
Consensus: Activities of promoting health literacy improve adherence.
Cognitive-assisted methods
1) Reminder devices
In a study targeting patients with various cardiovascular diseases combined with hypertension and/or dyslipidemia, reminder devices did not improve medication adherence.145) Another study with hypertension patients, however, reported that reminder devices improved adherence by 6 percentage points.146) In a study with an electronic reminder device, it did not improve medication adherence of statins but had significant effects in female patients in secondary preventive therapy.147) Therefore, a reminder device should be considered when used with other motivational programs.
Clinical question 19: Do reminder devices or medication assistive devices improve medication adherence?
Consensus: Reminder settings alone cannot improve medication adherence in the primary prevention of cardiovascular diseases.
2) Text messages
When text messages were sent via cellular phone to hypertension patients by a community agency, medication adherence was improved.148) Integrated implementation of an electronic reminder, pharmacist-led intervention, and medical professional-led interventions in primary and secondary prevention were effective for improving medication adherence. However, in a study limited to primary prevention, text messages alone did not improve mediaction adherence.149) Text messages are widely used today, cheap, and get instant responses, so they are being considered as a potential tool applicable to the clinical field for behavioral changes.150)
In studies on smoking cessation, obesity, or chronic diseases, text messages improved adherence to therapy. The effects of text messages in secondary prevention on medication adherence have been reported in several studies.151)152)153)154) Text messages increased the scores of the Morisky Medication Adherence Scale for antihypertensive drugs in African Americans but with no clinical benefit for blood pressure control in a randomized trial.155)156) Outcomes may vary according to the format of text messages, such as short versus long sentences, addition of educational materials, and special systems of transmission, which raises the need for additional research.157)
Clinical question 20: Do text messages improve medication adherence?
Consensus: Text messages improve medication adherence for the primary prevention of cardiovascular diseases.
3) Smartphone apps
In recent years, smartphones use has increased rapidly and widely. When a smartphone apps is used in primary prevention, it is effective for improving adherence.158)159) By using text messages or apps on a smartphone, patients can improve their medication adherence, maintenance of lifestyle changes, and control rate of chronic diseases.149)158)160)161)162) When special equipment or technology is introduced in addition to a smartphone, it can result in difficulties or inefficiency, which calls for caution.163) Specifically for primary prevention of cardiovascular diseases, MedISAFE-BP® was reported for small improvement in self-reported medication adherence but no changes in blood pressure level. This finding suggests that the efficacy of apps may be much different among the patient populations according to the various factors related to the adherence.164)
Clinical question 21: Do self-monitoring and feedback based on smartphone apps improve adherence?
Consensus: Self-monitoring and feedback based on smartphone apps improve adherence.
Factors related to health conditions
Emotional issues
Depression is known to decrease adherence to lifestyle changes165)166)167) and medication adherence including antihypertensive drugs.168)169)170) Antidepressant treatments for patients with depression in addition to cardiovascular diseases improves adherence for the primary prevention of cardiovascular diseases.45)171)
Clinical question 22: Does depression diagnosis and treatment improve adherence?
Consensus: The diagnosis and treatment of depression improves adherence.
Socioeconomic factors
Medication costs
The prevalence rate of self-reported cost related non-adherence in medication was reported as 16% in US elderly patients.172) Medication adherence drops according to the growing burden of medication costs on patients themselves. Vulnerable patients, including the elderly, may take less medicine due to the burden of medication costs.173)174)175)176)177)178)179)180)181) In all studies, medication adherence improved when patients did not have the burden of medication costs.53) Medication adherence was higher in generic drugs than branded drugs.179)182)183) Therefore, there is a need for research on medication adherence based on price differences between branded and generic drugs in domestic conditions.
Clinical question 23: Do cheaper drugs improve medication adherence?
Consensus: Reduction of medication cost improves medication adherence.
CONCLUSION
In conclusion, it requires significant changes in those 5 systems involved to successfully implement the guidelines supporting systematic approaches, which are evidence-based as reviewed in the present statements as shown in Table 3. Randomized clinical trials for long-term clinical hard outcomes are needed for formal guideline recommendations. Improving adherence might be an effective strategy to make a breakthrough on the decade-long stagnant control rate of chronic conditions for primary cardiovascular prevention in Korea.
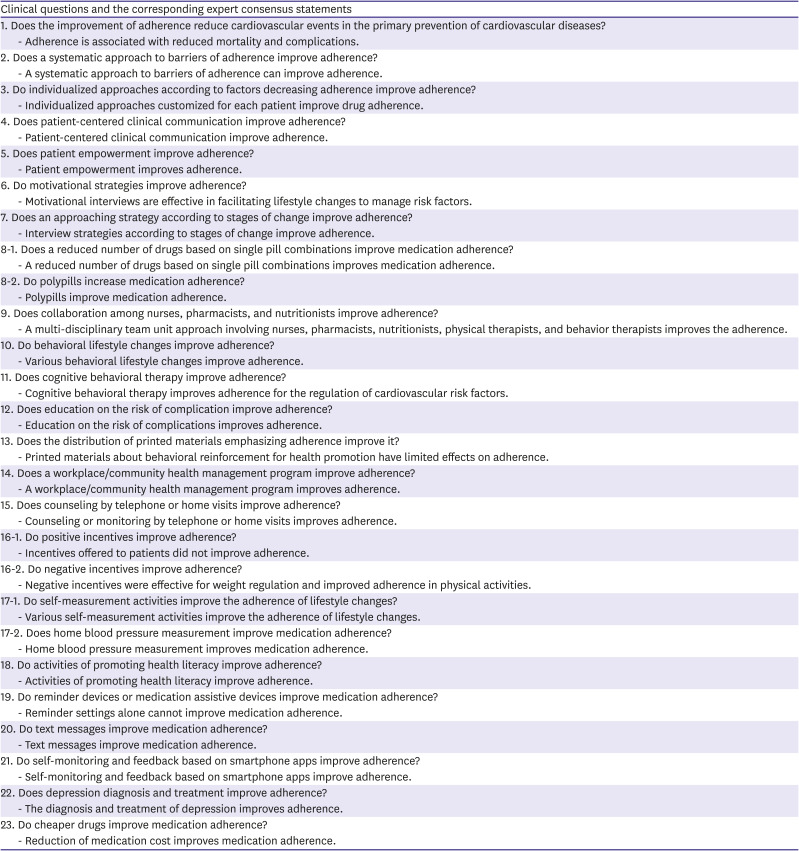
Table 3
Clinical questions related to adherence specifically for the primary prevention for cardiovascular diseases and the related expert consensus statements
 XML Download
XML Download