

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
According to a recent World Health Organization (WHO) report, an estimated 1.5 billion people worldwide now have hearing loss, and more than 5% (430 million) of the world’s population require hearing rehabilitation due to severe hearing loss. As the population ages, nearly 2.5 billion people are expected to experience some degree of hearing loss by 2050, of which at least 700 million will need hearing rehabilitation.1
South Korea’s population is rapidly aging at an unprecedented rate.2 The aging of the Korean population is progressing much faster than Japan, a representative aged country, and Korea will become a super-aged society (20% of the population in the 65 or over) after 2025.3 Hearing impairment has a significant impact on quality of life and may lead to cognitive decline.45 Therefore, active hearing rehabilitation is essential. However, the adoption rate of hearing aids (HAs) in Korea is relatively low compared to other countries. According to a previous study, the prevalences of HA acquisition and regular use were 17.4% and 12.6%, respectively.6 The main reasons for the low adoption rate of HA in Korea were outlined as follows: 1) inconvenient to wear; 2) high purchase price and maintenance cost; and 3) stigma against HA wearers.7 However, this study was conducted ten years ago and included only 317 respondents. As the adoption rate of HA has grown steadily in recent years, a further comprehensive investigation including current trends is necessary.
A large-scale survey of HA users has periodically been conducted by MarkeTrak in the United States since 2004 and published by the Better Hearing Institute (BHI) on behalf of the hearing care industry.8 In Europe, the European Hearing Instrument Manufacturers Association (EHIMA) began the EuroTrak study, an extensive study of hearing loss and HA, in 2009.9 These detailed and continuous nationwide surveys are helpful to monitor patients seeking HA and can be used as primary data for marketing HAs. These data help manufacturers seeking to increase the level of HA adoption by creating and providing products that are more suitable for people in need of HAs. Adoption of HA is associated with cognitive improvement and may reduce the social costs associated with hearing loss, which are projected to become enormous in the future. Unfortunately, a systematic survey of HA adoption has never been implemented in Korea. We constructed a survey and analyzed our data to describe the current status of the Korean HA market based on recent survey research, similar to MarkeTrak and EuroTrak. Our first goal was to investigate factors that influence the adoption of HA.
METHODS
Participants
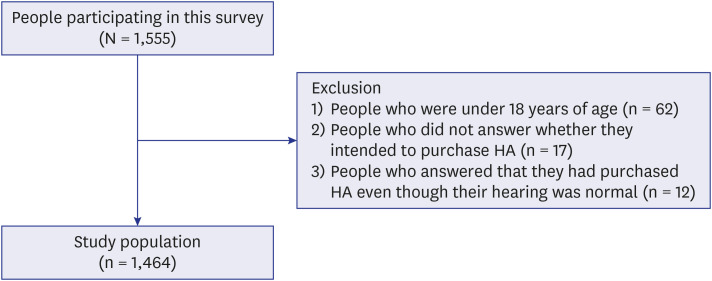
We conducted a large-scale prospective survey of patients who visited hospitals or HA centers due to hearing loss. A total of 1,555 individuals were surveyed across South Korea. We excluded 62 pediatric patients (under 18 years of age), 17 respondents who did not answer whether they intended to purchase HA, and 12 respondents who answered that they had purchased HA even though their hearing was normal. Finally, we analyzed data for 1,464 respondents. The flow chart of participants is shown in Fig. 1. The mean age was 70.4 ± 12.2 years, and there were 818 males and 646 females.
Survey questionnaire
Survey items relating to each of the variables of interest in this study were selected from those included in a large-scale survey based on theoretical and methodological considerations drawn from prior research. The dependent variable was a binary variable indicating whether to purchase HA. Independent variables were classified into three domains: demographic, audiological, and HA-related. The demographic domain included age, level of education, household income, and occupation. The audiological domain encompassed the total score of the Korean version of the Hearing Handicap Inventory for the Elderly (K-HHIE), hearing loss duration, disability registration status, and tinnitus. The HA-related domain consisted of the first HA consultation institution, HA recommendation during consultation, and obtaining HA-related information.
Data collection
The face-to-face survey was conducted by otologists or HA experts on a national basis. The data were collected at 10 tertiary hospitals, 7 general hospitals, 11 clinics, 22 HA centers, 3 medical equipment distributors, 1 community welfare center, and 1 other. The survey was conducted in multiple regions at 11 locations in Seoul, 13 locations in Gyeonggi-do, 5 locations in Incheon, 3 locations in Busan, 3 locations in Gangwon-do, 2 locations in Gwangju, 1 location in Gyeongsangbuk-do, 2 locations in Daejoen, 2 locations in Jeollabuk-do, 2 locations in Chungcheongbuk-do, and 1 location in Jeju. The data were collected by the Big Data center of Demant Korea and the Hearing Research Laboratory of SMC.
Statistical analysis
Data were analyzed using SAS ver. 9.4 (SAS Institute, Cary, NC, USA) and STATA ver. 14 (StataCorp, College Station, TX, USA) at the Clinical Epidemiology Center of SMC. The specific method of analysis is as follows:
1) An independent t-test or χ2 test was performed to identify the characteristics of HA owners and non-adopters.
2) Factors influencing whether to purchase HA were confirmed through multivariate logistic regression after adjusting for degree of hearing loss. Variables with P values < 0.15 in the independent t-test or χ2 test were included as independent variables.
RESULTS
Differences in characteristics between HA adopters and non-adopters
Among the 1,464 respondents, 1,190 (81.3%) purchased HA. Among the demographic characteristics, there were significant differences in age (P = 0.002), level of education (P = 0.002), household income (P = 0.005), and occupation (P = 0.003) between the HA purchase group and HA non-purchase group. Regarding audiological features, there were differences between HA adopters and non-adopters in all of the items investigated. There were significant differences in K-HHIE total score (P = 0.005), hearing loss duration (P = 0.003), disabled registration status (P = 0.002), and tinnitus (P = 0.005) between groups. In terms of HA-related traits, there were significant differences in first HA consultation institution (P = 0.004) and HA recommendation during consultation (P = 0.007) (Table 1).
Table 1
Characteristics of HA adopters and non-adopters (N = 1,464)
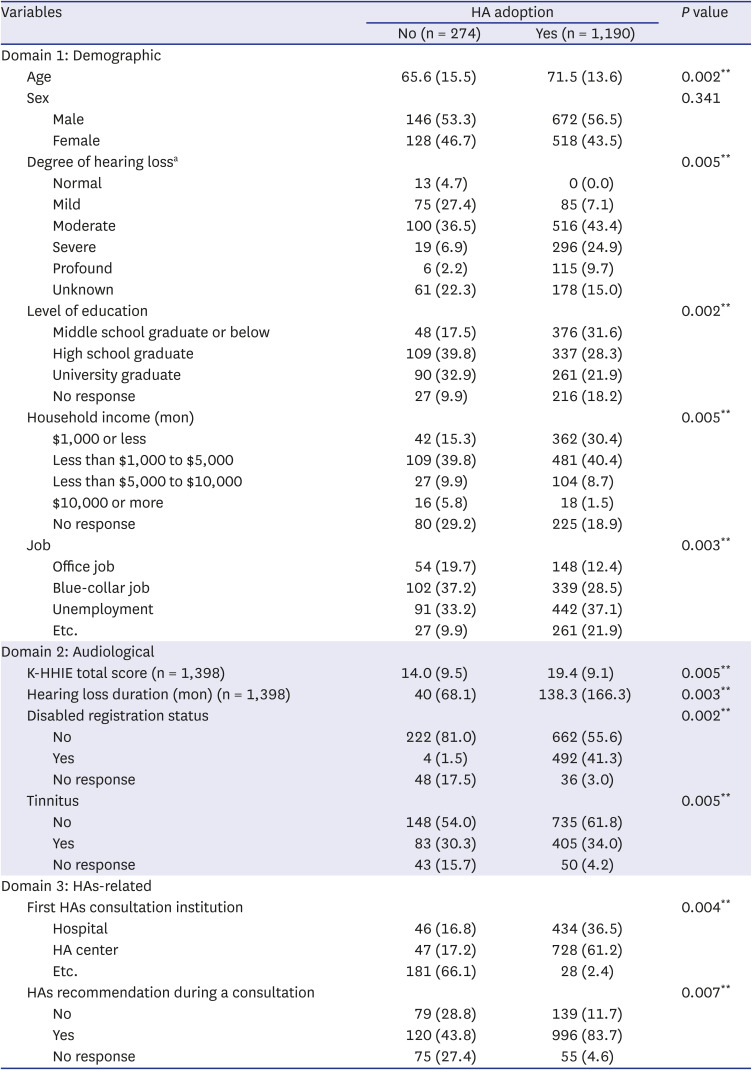
Values are presented as number (%).
HA = hearing aid, K-HHIE = Korean version of the Hearing Handicap Inventory for the Elderly.
aIt is the degree of subjective hearing loss, and it is defined as the severe one among the degree of hearing loss in both ears. If there is no degree of hearing loss in both ears, it is defined as unknown.
**P < 0.01.
Factors influencing HA purchase
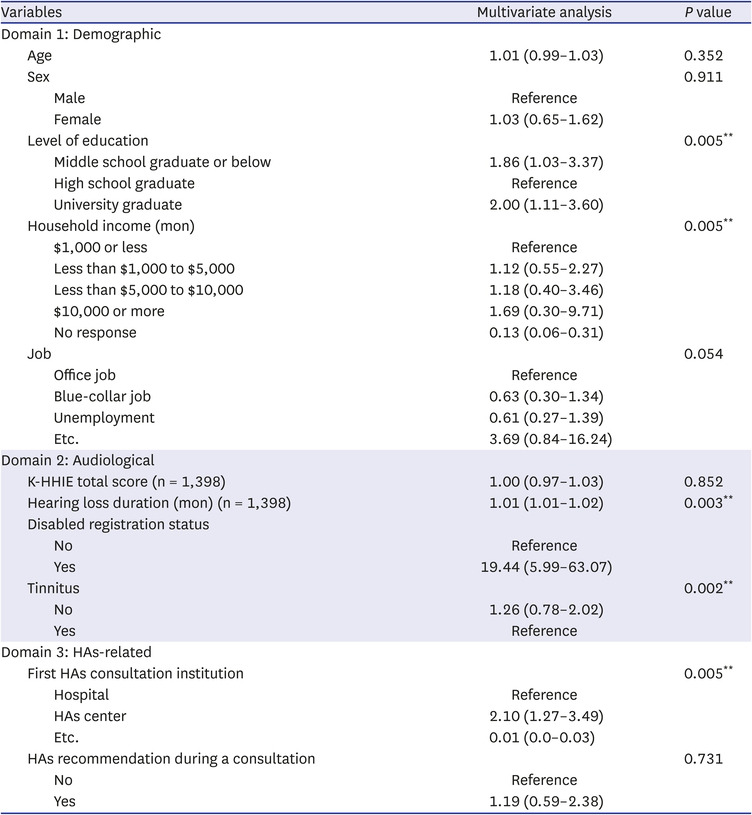
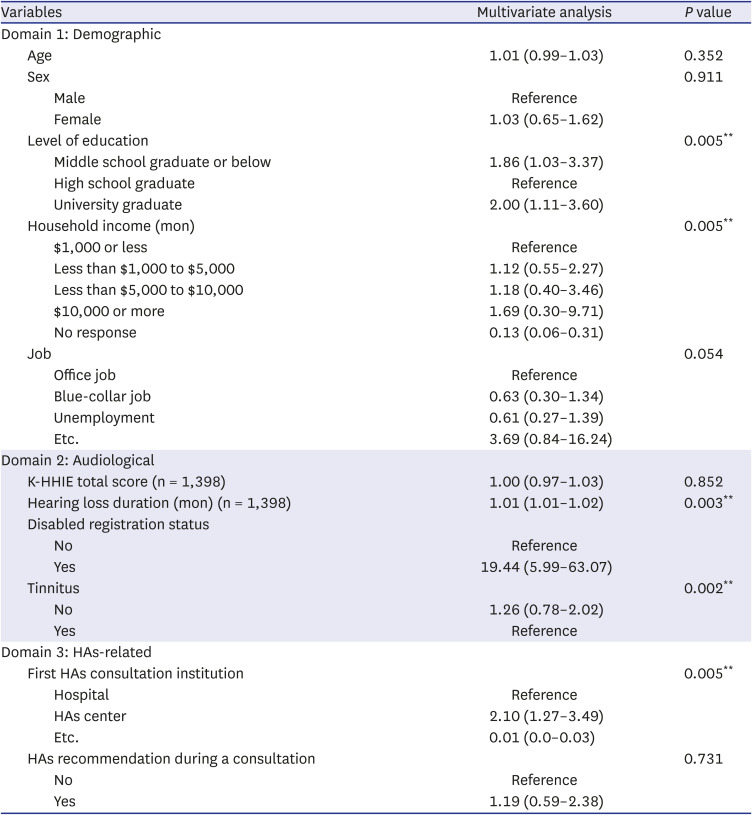
Multivariate logistic regression analysis was performed using variables showing significance in the univariate analysis (P < 0.15). Consequently, level of education, household income, hearing loss duration, disability registration, and first HA consultation institution were significant factors for HA adoption. In terms of level of education, individuals who were middle school graduates or below were 1.86 times (odds ratio [OR], 1.86; 95% confidence interval [CI], 1.03–3.37), and university graduates were two times (OR, 2.00; 95% CI, 1.11–3.60) more likely to purchase HA compared to high school graduates. In terms of household income, respondents who earned less than $1,000 to $5,000 were 1.12 times (OR, 1.12; 95% CI, 0.55–2.27), less than $5,000 to $10,000 were 1.18 times (OR, 1.18; 95% CI, 0.40–3.46), and $10,000 or more were 1.69 times (OR, 1.69; 95% CI, 0.30–9.71) more likely to purchase HA compared to those earning $1,000 or less. Related to hearing loss duration, tendency to purchase HA became 1.01 times (OR, 1.01; 95% CI,1.01–1.02) higher every month for the duration of hearing loss increased. Regarding government assistance status, those who received a 3rd party reimbursement were 19.44 times (OR, 19.44; 95% CI, 5.99–63.07) more likely to purchase HA compared to those who received no reimbursement. Regarding the first HA consultation institution, respondents who received consultations at a HA center were 2.1 times (OR, 2.10; 95% CI, 1.27–3.49) more likely to purchase HA than those who received consultations at hospitals (Table 2).
Table 2
Logistic regression models for HA adoption in patients with hearing loss
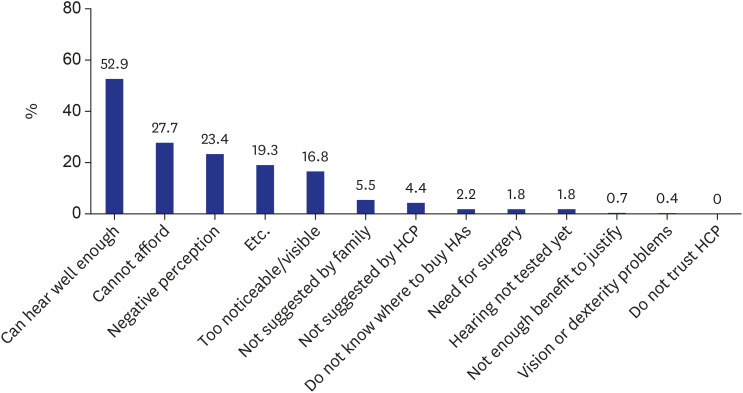
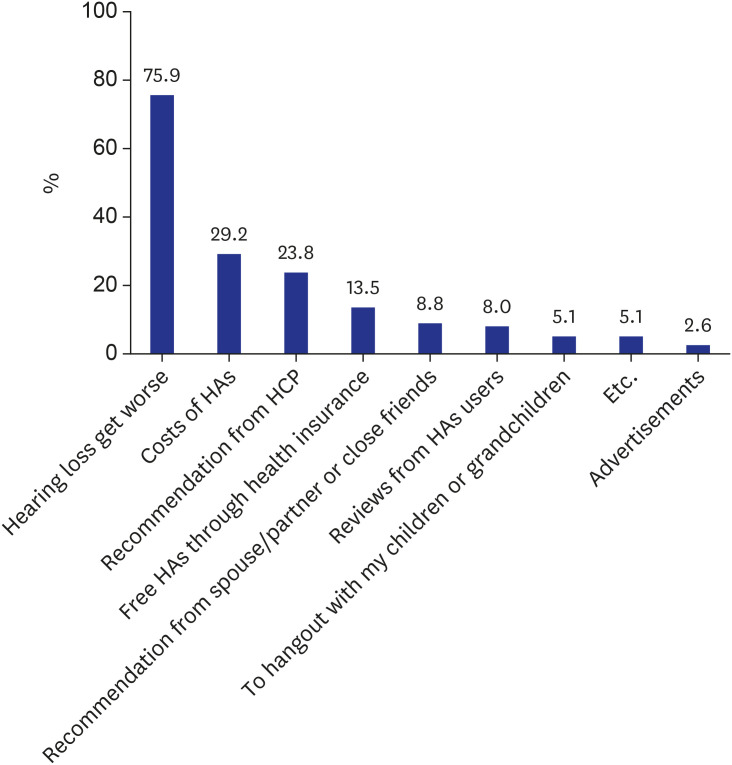
Descriptive analysis of reasons for non-adoption of HA, factors affecting purchasing decisions, and intention to purchase HA
Two hundred and sixty-seven people who did not purchase HA elucidated reasons for non-adoption of HA, factors affecting purchasing decisions, and intention to purchase HA in the future. The top three reasons cited were: can hear well enough (52.9%), cannot afford (27.7%), and negative perception (23.4%) (Fig. 2). The three most common factors affecting the purchasing decision were progression of hearing loss (75.9%), cost of HA (29.2%), and suggestion of health care professionals (23.8%) (Fig. 3). Furthermore, 86% of respondents said they are willing to purchase HA in the future.
DISCUSSION
This is the first large-scale, systematic, comprehensive study of HA adoption in Korea. In the context of a rapidly increasing elderly population, we comprehensively analyzed factors influencing HA purchase. These factors were education level, household income, hearing loss duration, disabled registration status, and first HA consultation institution.
The HA adoption rate was 1.86 times higher among individuals who were middle school graduates or below (low-educated) and two times higher among university graduates (high-educated) compared to high school graduates. This is because low-educated respondents have a high probability of belonging to lower household income strata, and therefore receive 100% HA subsidies. High-educated respondents might be more likely to purchase HA due to greater awareness of the importance of hearing rehabilitation and higher household income.
Financial constraints are considered significant barriers to HA adoption. The MarkeTrak10 survey indicated that household income impacts the decision to purchase HA.10 In a 2007 survey, about 76% of respondents answered that financial issues were a barrier to HA adoption.11 In addition, 64% of the responders reported that they could not afford HA, and nearly half (49%) indicated financial problems were straightforward reasons for non-adoption of HA. The drastic improvement in the economy affected about 1 in 5 people (18%) with moderate-severe hearing loss in the U.S. when deciding to purchase HA.12 Our findings were in line with previous surveys indicating that the higher the household income, the greater the availability of HA. Furthermore, 27% of the non-adopters responded that they do not use HA because they cannot afford the cost. Although there were no significant differences in the HA adoption rates according to workplace in this survey, office workers were more likely to adopt HA than blue-collar workers or unemployed respondents. This also indirectly explains the impact of financial factors on HA purchases. According to EuroTrak UK 2018 data, people with HA recognize that HA increase the chances of hearing impaired individuals to be promoted, to obtain good jobs, and to attain higher salaries. Therefore, it is necessary to analyze the HA adoption rate of office workers in the future by dividing the sample into specific occupational groups.
In Korea, until 2015, registered persons with hearing disabilities were eligible for only about $300 per ear under Korean National Health Insurance reimbursement rules. However, since government subsidy rates have more than tripled from $300 to $1,150 in November 2015, the HA adoption rate has rapidly increased. These policies are intended to relieve the financial burden of hearing loss and offer HAs of good quality at reasonable prices. In this study, the proportion of respondents with third party reimbursement was 19.44 times higher than those without reimbursement. This results in a much greater effect than the previously mentioned impact of household income on HA purchases. Therefore, third party reimbursement is one of the most critical factors for HA adoption. These results agree with those of the MarkeTrak10 survey, showing that the rate of the likelihood of HA adoption rises with increased rates of insurance coverage.10
The decision to acquire HAs is also dependent on hearing loss duration. According to the MarkeTrak10 survey, HA adopters reported longer durations of hearing loss (mean duration of hearing loss = 14.6 years) than HA non-adopters (mean = 10.5 years).10 The survey found that HA adopters tended to be older and to have more significant hearing loss. In the present survey, HA adopters (mean age = 71.5 years) were significantly older than HA non-adopters (mean age = 65.6 years) (P < 0.01). Age-related hearing loss is characterized by gradual, progressive sensorineural hearing loss leading to impaired communication. Therefore, the elderly are the main users of HAs. However, age alone was not a predictor of HA purchase.
We found that the HA adoption rate was approximately twice as high when receiving HA counseling at a HA center rather than a hospital. The reason for this is that many hearing loss patients who have visited hospitals expect other treatments, such as surgery or medication, in addition to HA, and may undergo hearing rehabilitation through other methods. However, patients who visit HA center may visit with the intention to purchase HA. In the MarkeTrak8 survey, the frequency of purchasing HA after being referred by an audiologist rather than an ear, nose, and throat doctor was slightly higher.12
A recent study of HA adoption among Americans reported that married status, white race, high socioeconomic status, poor hearing, and high HHIE scores increase the adoption rate of HA.13 In our study, we found that the higher the HHIE score, the higher the probability of adopting HA, but there were no significant differences according to degree of hearing loss. This suggests that if the degree of hearing loss is similar, the price or support policies surrounding HA may be more important than the discomfort caused by hearing loss itself.
We further studied the reasons for non-adoption of HA, factors affecting purchasing decisions, and intention to purchase HA. The greater reason for non-adoption of HA and factors affecting the purchasing decision were directly related to hearing. In general, older people tend to underestimate their hearing loss.14 In the Korea National Health and Nutrition Examination Survey conducted several years ago, 13.1% of subjects underestimated their hearing loss compared to their actual hearing.15 This discrepancy is also an important barrier to purchasing HA. However, hearing loss can lead to other disorders such as depression, falling and cognitive impairment. Therefore, it is necessary to regularly conduct hearing evaluations for the elderly and to rehabilitate hearing with HA in a timely and appropriate manner to prevent or delay further deterioration. In addition, barriers to the adoption of HA included negative perceptions and cost of HA. In this case, other types of hearing devices, such as personal sound amplification products, may be options for patients with mild-to-moderate hearing loss.1617
This study has limitations. First, the HA adoption rate reported in this study is much higher than in previous research. One possible explanation may be sampling bias. The data were mainly collected at hospital outpatient clinics or HA centers. However, our main purpose was to investigate factors influencing HA adoption, and it is necessary to focus on these results. Second, this study was a retrospective analysis of existing clinical data. In particular, the degree of hearing loss of the subjects could not be evaluated objectively like the pure tone hearing average or speech discrimination score. Similarly, we could not add more variables that could be related to HA adoption, including hearing outcomes. Further prospective research is required to explore such variables further.
In conclusion, education level, duration of hearing loss, household income, and place of purchase were important factors associated with intention to purchase HA, with third party reimbursement identified as the most prominent factor. These findings suggest that the government needs to play a more active role in increasing the distribution of HA to patients with hearing loss in South Korea in the future.
 XML Download
XML Download