

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular diseases (CVDs) are the most typical causes of mortality and morbidity in the world. The Global Burden of Disease (GBD) Study 2019 had estimated that there are 523 million cases of CVD in 2019. The number of CVD deaths had increased from 12.1 million in 1990 to 18.6 million in 2019. Ischemic heart disease (IHD) had contributed to about 182 million disability-adjusted life years (DALYs), 9.14 million deaths, and 197 million prevalent cases in 20191) and is the topmost cause of death according to World Health Organization (WHO) for 2019.2) In comparison with 2000, the number of deaths has increased from 2 million to about 8.9 million in 2019.2) It is estimated that around 80% of deaths from CVD occurred in low and middle-income countries. It is estimated that around 23.6 million deaths are expected to occur from CVDs by 2030.3)4) Around 85% of these deaths are expected to occur from Myocardial infarction (MI) and stroke.3)
The most common symptoms of MI are pain, or discomfort felt in the center of the chest; in the arms, in the left shoulder, in the elbows, in the jaw, or back; or shortness of breath; or feeling of being sick or vomiting; or a feeling of light-headedness.5) The prognosis is good in MI when reperfusion is sought immediately after the onset of symptoms.6)7) Prompt presentation for medical attention can drastically decrease the associated mortality and morbidity associated with patient delay. ‘Patient delay’ is the delay since symptom onset and pursuing medical assistance.8) In surveys conducted worldwide, most of the population have recognized chest pain as the predominant symptom of MI.9)10) However, there is a lack of knowledge about other symptoms in MI.11) Knowledge about the atypical presentation of MI and its recognition lacks in the world's common population.9)10)11)12)13)14)15)16)17) Therefore, inadequate awareness of heart attack symptoms ensures direct association with patient delay and adverse health events subsequently.9) Due to the increased risk of CVDs, the WHO has set a target of a 25% reduction in CVD-associated premature mortality by 2025.18) This starts from primary prevention by addressing CVD risk factors and symptoms of the diseases to the public, timely and appropriate treatment of cardiovascular events like acute coronary syndrome, and evidence-based secondary prevention programs to reduce adverse outcomes.19)20) Knowledge about symptoms of CVDs and it's risk factors is vital to change the health attitudes, behavior, and lifestyle practices of an individual.21) Identifying the gaps in knowledge of CVD illnesses among the general populace with unremitting behavioral changes effectively combatting. Though various studies provide knowledge on heart attack symptoms, there is a dearth of literature that shows the overall level of knowledge.22) In the past, systematic reviews have identified the population's proportion not having the knowledge to identify a single risk factor or symptom as 1.8% among hospital workers in Nigeria to a maximum of 75.1% in a general population in Uganda.22) Various studies have been done regarding public knowledge of MI symptoms.21)23)24) However, these studies have focused on specific groups, and no study addressed the global prevalence of MI symptoms awareness. The present systematic review and meta-analysis is carried out to estimate the prevalence of awareness of myocardial infarction symptoms among the general population.
METHODS
Search strategies
This systematic review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement as presented in the PRISMA checklist. (Supplementary Table 1)25) and registered on PROSPERO (CRD42020219802) on December 2020.
On December 9th 2020, we searched 5 databases, including PubMed, Google Scholar, Scopus, WHO Global Health Library, and Virtual Health Library (VHL), to retrieve relevant articles using the following search term: (Awareness OR Attitude OR Knowledge OR perception OR understanding) AND ((myocardial infarction) OR (acute coronary syndrome) OR (heart attack) OR STEMI OR NSTEMI) AND (symptom OR symptoms OR sign OR signs) (Supplementary Table 2). A manual search of references was done to retrieve any missed relevant papers. The reference lists of all included studies were screened against inclusion criteria with full-text screening whenever needed, references of previous review articles were also searched.
Study eligibility criteria
The citations generated from all the studies were exported in endnote version 8 to remove the duplicates. The articles were then exported in excel, and 3 independent reviewers screened titles and abstracts to identify potential studies according to inclusion and exclusion criteria. The inclusion criteria included; articles reporting the prevalence of awareness level of signs and symptoms in the general population. There was no restriction on language, age or demographic characteristics, or socioeconomics of the study population. Articles reporting awareness in medical staff, paramedical staff, medical residents, students, health care workers, and nurses were excluded. Moreover, abstract only articles like conference papers, letters, commentaries, or thesis projects, books, case reports, editorial review, or author's response, and study from which data could not be extracted and overlapped data were excluded.
All the full-text versions of included articles through title and abstract screening were obtained and reviewed carefully by 3 independent researchers to reach a final inclusion or exclusion decision. In case of disagreement, help from another independent reviewer was taken to reach the final conclusion.
Data extraction
We developed a data extraction sheet in Microsoft Excel, piloted it with 3 randomly different included papers, and modified it accordingly. The extraction sheet consisted of three categories: essential study characteristics (authors, year of publication, year of research, country of the first author, country of the patients, inclusion and exclusion criteria, and sample size), participants characteristics (age, sex, occupation, country of participants, socio-economic profile, ethnicity) and data sheet (prevalence of awareness of typical symptoms of MI). Each article's data was extracted by three independent reviewers and was checked again to resolve disagreements and reach a consensus through discussion. Articles published by the same study group or same research group of authors were checked for the potential duplicate data; these articles were checked for country and recruitment year of participants. When overlapping data were identified in the extraction process, we chose the data of latest set or before intervention to extracted data.
Quality assessment
Three reviewers independently performed the quality assessment. National Institutes of Health (NIH) quality assessment tool was used to determine the quality of selected studies.26) Quality assessment was also performed by discussion and consensus after the independent review of each study by 3 reviewers. In case of disagreement, an opinion from another independent reviewer was taken.
Statistical analysis
All analyses were done by R statistical software version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria).27) Packages meta and metafor were used.28)29) A random-effects model was used due to the data's heterogeneous nature for both source and patients' characteristics. Pooling data from each study calculated overall prevalence with 95% confidence interval (CI). Heterogeneity was assessed with Q statistics and I2-test considering it significant with I2 value >50% or p-value <0.10. The subgroup analysis was conducted according to continents, country, sex, and ethnicity. Egger's regression test30) was used to assess the publication bias. Its graphical representation was done using Begg's funnel plot in the case of studies numbering ten or more than ten. A p value of <0.05 was considered statistically significant for Egger's regression test. In case of publication bias, missing studies were added by using the trim and fill method of Duvall and Tweedie. New prevalence with 95% CI was then calculated by adding the missing studies.
RESULTS
Literature search results
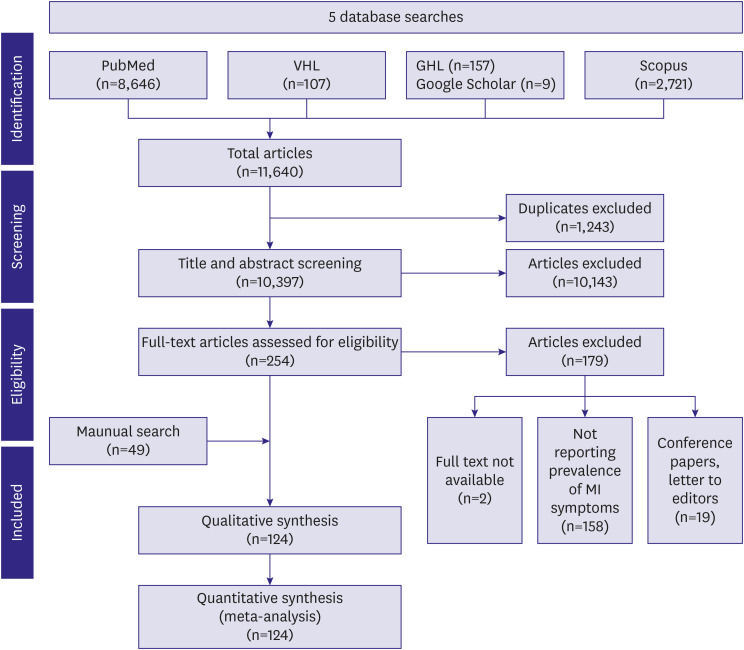
The PRISMA flow diagram shows the process of study selection and inclusion (Figure 1). Five databases were searched using keywords. This preliminary search yielded a total of 11,640 articles. One thousand two hundred and forty-three duplicates were identified and excluded via endnote. The remaining 10,397 articles were assessed for eligibility by title and abstract. This screening yielded 254 articles. Of these 254 articles, 179 were excluded during full-text screening. The reasons for their exclusion were not reporting the prevalence of MI (n=158), conference papers and letters to editors (n=19), nonavailability of full text (n=2). A manual search yielded 49 articles. This resulted in a total of 124 articles for final analysis.
Baseline characteristics of included studies
A total of 124 studies from 35 countries were included in the final analysis. The study design, sample size, gender, and inclusion criteria of the individual studies are described in Supplementary Table 3. A majority (n=49) of the studies were done in the USA, followed by Canada (n=6). Regarding the studies' quality, 64 studies were of good quality, 58 studies were of fair quality and 3 studies were of poor quality. Most (n=112) of the studies were observational studies. Of these, 110 were cross-sectional studies or surveys. In 12 studies, outcomes were reported either as a part of experimental studies or quasi-experimental studies. The final analysis included a total of 120,988,548 individuals, of whom 311,943 (0.002%) individuals had the previous history of MI.
Main results
Prevalence of awareness of typical symptoms of MI
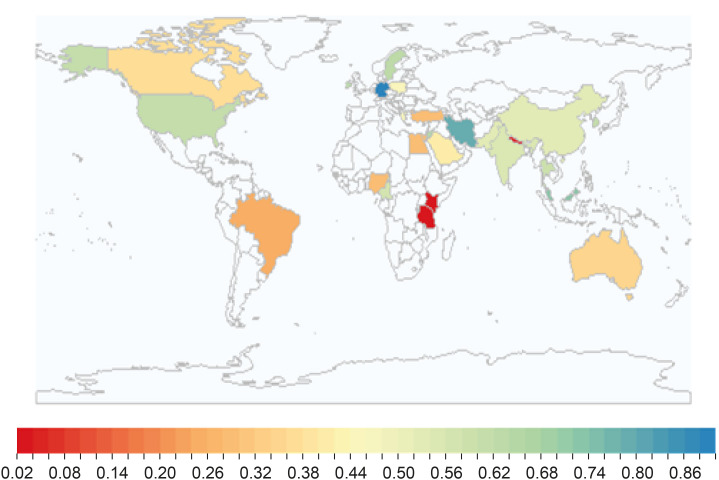
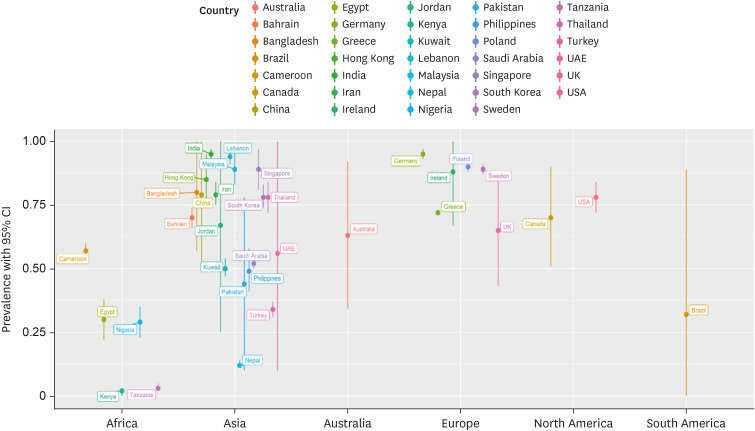
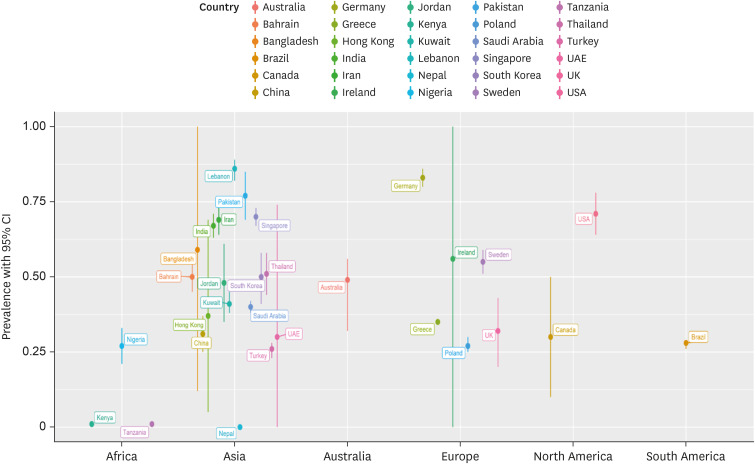
Figure 2 shows the prevalence of awareness of all typical symptoms of MI in different countries of the world. The prevalence varies from less than 5% in African countries such as Tanzania (3%), Kenya (3.4%), and less than 30% in UAE (28%), Nigeria (29%) to as high as 89% in Germany, 79% in Lebanon and Iran, 72% in Malaysia, 71% in Singapore, 65% in Jordon, and 64% in Sweden.
Figure 2
Global prevalence awareness of all typical symptoms of MI of different countries.
MI = myocardial infarction.
The overall prevalence of awareness of all typical MI symptoms in males was 57% (95% CI, 51–62%) and 57% (95% CI, 52–63%) in females. Meta-regression analysis was performed to see the effect of gender. The overall proportion of variance explainable by gender in the final model was 0% (R2=0%, p=0.87). Gender is not associated with the change in the effect size of prevalence awareness (Supplementary Figure 1A).
Total 13 articles studied the prevalence in various ethnicities, of those 11 studies were carried out in USA. Prevalence of awareness of all typical symptoms of MI was higher in Caucasian White, White, and non-Hispanic white group 66% (95% CI, 59–74%) compared to non-Hispanic blacks and black group 56% (95% CI, 46–66%), Hispanic group 53% (95% CI, 44–61%) and Asians 42% (95% CI, 33–52%). On Meta-regression analysis, ethnicity account for the 7.89% variance (R2=7.89%, p=0.01). It was found that Caucasian Whites, White, and non-Hispanic whites ethnicity is associated with a higher prevalence of symptoms (Supplementary Figure 1B).
Prevalence of awareness of chest pain as a symptom of MI
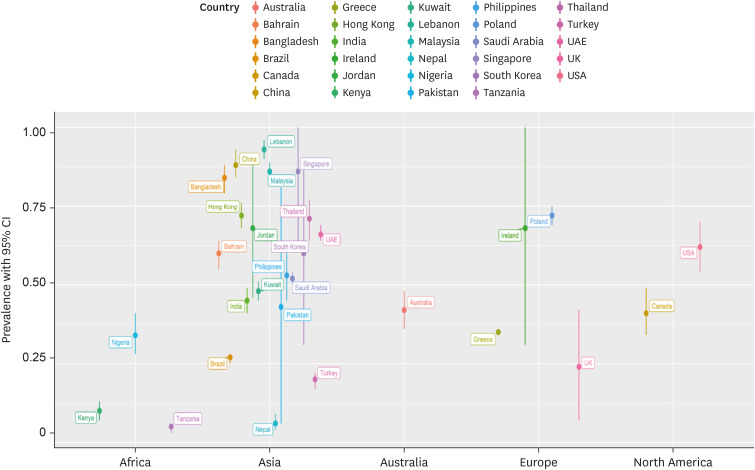
A summary of chest pain awareness as a symptom of MI in different countries is presented in Figure 3. One hundred and five studies were included in the overall quantitative analysis. The pooled prevalence of awareness of chest pain as a symptom of MI for each continent (Supplementary Figure 2) was Africa 30% (95% CI, 10–51%), Australia 63% (95% CI, 34–92%), Asia 68% (95% CI, 60–76%), South America 4% (95% CI, 3–4%), North America 77% (95% CI, 71–82%), and Europe 80% (95% CI, 69–91%). Major weight of the pooled estimate (41.9%) was contributed by studies conducted in the USA. The highest prevalence was seen in Germany (95%; 95% CI, 93–97%), India (95%; 95% CI, 93–97%), and Lebanon (94%; 95% CI, 91–96%). However, studies from these countries involve people who have early incidents of MI. The lowest prevalence was seen in Kenya (2%; 95% CI, 1–4%) and Tanzania (3%; 95% CI, 2–5%).
Prevalence of awareness of the shortness of breath as a symptom of MI
Figure 4 shows the awareness of shortness of breath as symptom of MI in different countries. Eighty-eight studies were included in the overall quantitative analysis. The pooled prevalence of awareness of shortness of breath pain as a symptom of MI for each continent (Supplementary Figure 3) was Africa 34% (95% CI, 9–59%), Australia 42% (95% CI, 36–48%), Asia 59% (95% CI, 49–69%), South America 27% (95% CI, 25–28%), North America 62% (95% CI, 54–69%) and Europe 45% (95% CI, 25–65%). The highest prevalence was seen in Lebanon 93% (95% CI, 90–95%) and China 88% (95% CI, 84–93%). The lowest prevalence was seen in countries such as Tanzania 5% (95% CI, 3–6%), Nepal 6% (95% CI, 4–9%) and Kenya 10% (95% CI, 7–13%). No publication bias was found (Egger's p value=0.0989)
Prevalence of awareness of pain and discomfort in the arm as a symptom of MI
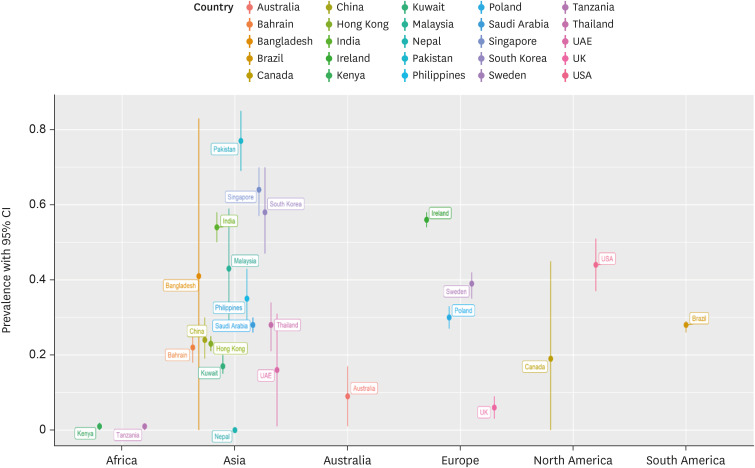
Eighty-two studies were included in the overall quantitative analysis. The pooled prevalence of awareness of pain and discomfort in the arm as a symptom of MI for each continent (Supplementary Figure 4) was Africa 42% (95% CI, 26–58%), Australia 68% (95% CI, 48–88%), Asia 54% (95% CI, 44–65%), South America 93% (95% CI, 93–93%), North America 51% (95% CI, 42–59%) and Europe 66% (95% CI, 55–77%). Germany 83% (95% CI, 80–86%), Pakistan 77% (95% CI, 69–85%) and USA 71% (95% CI, 64–78%) had high prevalence, while Nepal 0 (95% CI, 0–1%), Kenya 1% (95% CI, 0–2%) and Tanzania 1% (95% CI, 0–1%) (Figure 5) had the lowest prevalence. No asymmetry was found on the funnel plot on visual inspection, which was confirmed with an Egger's-regression test (p=0.191)
Prevalence of awareness of jaw, neck, and back pain as a symptom of MI
Figure 6 shows a summary of awareness of jaw, neck, and back pain as a symptom of MI in different countries. Seventy studies were included in the overall quantitative analysis. The pooled prevalence of awareness of jaw, neck and back pain as a symptom of MI for each continent (Supplementary Figure 5) was Africa 10% (95% CI, 0–23%), Australia 9% (95% CI, 1–17%), Asia 40% (95% CI, 31–48%), South America 28% (95% CI, 26–29%), North America 41% (95% CI, 34–48%) and Europe 33% (95% CI, 12–53%). The highest prevalence was seen in Pakistan 77% (95% CI, 69–85%), and Singapore 64% (95% CI, 57–70%). The lowest prevalence was seen in countries such as Nepal 0 (95% CI, 0–1%), Kenya 1% (95% CI, 0–2%), and Tanzania 1% (95% CI, 0–1%). The Egger's p value for publication bias was insignificant (p=0.54)
Prevalence of awareness of weakness, light-headedness, and fainting as a symptom of MI
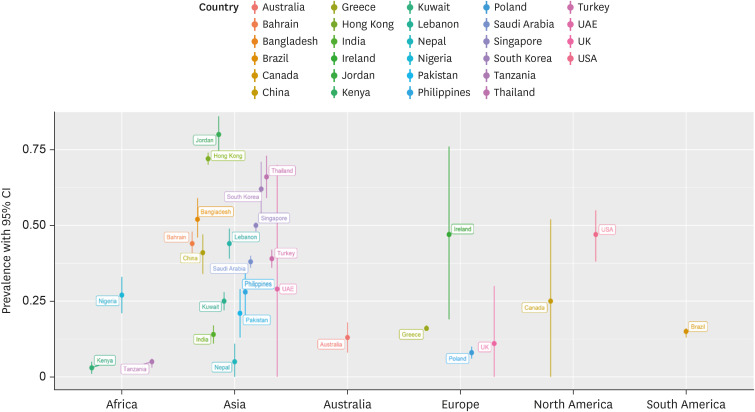
Seventy-seven studies were included in the overall quantitative analysis. The pooled prevalence of awareness of weakness, light-headedness and fainting as a symptom of MI for each continent (Supplementary Figure 6) was Africa 28% (95% CI, 4–53%), Australia 50% (95% CI, 3–97%), Asia 45% (95% CI, 36–53%), South America 15% (95% CI, 8–21%), North America 37% (95% CI, 29–45%) and Europe 51% (95% CI, 31–71%). Regarding countries, Jordan 80% (95% CI, 74–86%), Hong Kong 72% (95% CI, 70–74%) and Thailand 66% (95% CI, 59–73%) had high prevalence, while countries such as Kenya 3% (95% CI, 1–5%), Tanzania 5% (95% CI, 3–6%) and Nepal 5% (95% CI, 0–11%) had low prevalence (Figure 7). No publication bias was detected.
DISCUSSION
In this meta-analysis, we have included 124 studies and explored the knowledge of MI symptoms in 120,988,548 subjects in total, expanding across 35 countries. Studies done in the USA were in maximum numbers, followed by Canada. Amongst all the subjects, 48.9% were males. In this meta-analysis, chest pain is the most identifiable symptom of MI, while the feeling of light-headedness and pain in the jaw, neck, and back are the least identifiable symptoms. Seeking medical attention lately by delaying from the onset of heart attack symptoms is of international concern. In a systematic review done by Birnbach et al.31), including 86 articles, weighed mean for chest pain as a symptom of MI was found to be 74.3% which is in line with the pooled prevalence of 70% for awareness for chest pain as a symptom of MI reported by our study. Fourteen studies (China, Bangladesh, Ireland, USA, Australia, Germany, Spain, USA, Jordon [2], UK [2], Brazil, Sweden) involved patients with a history of the previous diagnosis with MI. These individuals have higher prevalence than other persons.
Our meta-analysis also finds that countries like Tanzania, Kenya, Nepal, Brazil, UAE, and Nigeria have the lowest prevalence of awareness of MI symptoms. Because these countries have a high burden of infectious disease, much of the government's sources are used in combating infectious disease. Although there has been decreased communicable disease burden in Kenya, it still predominates the total disease burden. Similarly, according to the 2019 report of Centers for Disease Control and Prevention, human immunodeficiency virus and Tuberculosis are the leading cause of death in Tanzania. In Tanzania, only 3 out of 100 people can recognize the typical symptoms of MI. Although Tanzanian Ministry of Health has initiated efforts to educate people about heart disease, they are not well-wide spread in community.
Similarly, Nepal and Nigeria, with limited resources, are mainly fighting the infectious disease burden also. In the case of the UAE, the low awareness of MI symptoms is due to gender disparity. Our meta-analysis found the overall prevalence of awareness of MI symptoms in the UAE is 28%. However, only 19% of women in UAE are aware of symptoms of heart disease. There is an apparent lack of knowledge on the severity and vulnerability of heart disease in women.
Germany, Lebanon, Iran, Malaysia, Singapore, Jordon, Bangladesh, and Sweden have a high prevalence of typical MI symptoms. The studies from Germany, Lebanon, Jordon, Bangladesh involved patients who had a previous history of MI and had a higher level of awareness than others.
The present meta-analysis showed no variation regarding the knowledge of MI symptoms among males and females, and these results were congruous with the studies done by O'Brien et al.17)
Several studies have stressed the health gaps in different ethnic groups and hypothesized the reasons for the same, identifying that such variations could also serve as a barrier in identifying MI symptoms. Our study explored the prevalence of awareness of typical MI symptoms in various ethnic groups, including Whites, Caucasian White, Blacks, non-Hispanic blacks, Hispanics/Latino, Asians. It has been observed in various studies that African-Americans have a greater predisposition to various cardiovascular and metabolic diseases. Higher mortality due to CVD-associated diseases has also been observed in this group. This is a matter of concern and has further been highlighted in our study; the overall prevalence of awareness of various typical MI symptoms was lower in blacks than Caucasian white and white ethnic groups. Data taken from the 2001 Behavioral Risk Factor Surveillance System, a telephone survey conducted across 17 USA states, also points out to greater prevalence of knowledge of symptoms amongst the Whites than other ethnic groups.
This study findings have significant implications for health policy and further research. From this study, we can say that there is a need for the health department authorities to develop strategies and programs to improve knowledge among the general population for the recognition of symptoms of heart attack, which will help the individuals seek appropriate urgent care. Health Education and Promotion must be conducted considering gender, age, education level, and occupation of the people. More significant efforts should be directed toward high-risk populations with low awareness, such as racial/ethnic minority groups and low educational levels. Intensified public health promotion campaigns via radio, television, advertisements, and text messages will help educate the public on warning signs of heart attack and CVD risk factors. Our meta-analysis found that most patients identified chest pain as a symptom of MI, while there was a low prevalence of other MI symptoms. In this study, most of the studies used the self-reporting method which might lead to under or overestimation of data. Some studies used open and some close-ended questionnaires; the validity of such studies could not be deduced, leading to reporting bias in results. Some patients may have correctly guessed the answers. Some studies involve patients who have been previously suffered MI. Clearly, such patients have a higher prevalence of awareness than other general populations. This would have resulted in an overestimation of knowledge levels. From many countries, only one study was available that limits the generalizability of prevalence of that country. The main purposes of most literatures included in this meta-analysis were heterogeneous and those in some studies were not related to the prevalence of the awareness of MI symptoms. Keeping these limitations in mind, our study provides support for the importance of raising awareness among the general population.
 XML Download
XML Download