

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bladder pain syndrome (BPS) is a debilitating chronic inflammatory bladder disorder that and has a significant negative impact on quality of life.1 The diagnosis is based on clinical symptoms, characterized by persistent or recurrent chronic pelvic pain, pressure, or discomfort, accompanied by at least one urinary symptom, such as urgency or frequency, without other pathologic findings that could cause these symptoms.123 Although multiple national and international guidelines have been published on the diagnosis and management of BPS, a global consensus on its definition, the nomenclature used, and criteria for its diagnosis and treatment are lacking.1 The inconsistency in the definition of the disease and its diagnostic criteria has made epidemiological investigations challenging,4 several of which have reported mixed results due to non-standard diagnostic criteria (such as physician-confirmed diagnoses or the use of various questionnaires) and different survey methods (medical records, phone, or mail).4567891011121314
Recent studies on the prevalence of BPS have screened patients with BPS-like symptoms using validated questionnaires such as the O'Leary-Sant Interstitial Cystitis Symptom and Problem (OLS) index and the Pelvic Pain and Urgency/Frequency (PUF) Patient Symptom Scale.481112131415 Prevalence studies using the OLS questionnaire reported that the prevalence of BPS-like symptoms among women is 0.26–0.57%.811121314 In a population-based study,11 the prevalence of BPS-like symptoms among US women was 0.57% when based on the OLS questionnaire results, but much higher at 12.6% when based on the PUF scale scores. The PUF scale is a symptom questionnaire for screening BPS in the general population and is useful for assessing pelvic pain, such as that caused by symptoms related to sexual intercourse, as well as urinary symptoms (urgency/frequency).16 The PUF scale is closely related to the results of the potassium sensitivity test (PST), which is a specific test for detecting interstitial cystitis (IC) in the general population.16 This suggests that BPS may be underdiagnosed and substantially more common than previously thought.415 In 2010, a Korean version of the PUF questionnaire was developed using linguistic validation.17
To the best of our knowledge, there have been few studies on population-based symptom prevalence of BPS among Korean adults using the PUF scale. Therefore, this study aimed to investigate the prevalence of BPS-like symptoms in the general population of South Korea between the ages of 40 and 79 years using the PUF Patient Symptom Scale.
METHODS
Study design and population
To investigate a reliable estimate of the prevalence and identify sufficient cases to describe the characteristics of people with the disease, we commissioned a survey from Hankook Research, the nation's largest marketing and opinion research firm in Korea. Between April 16, 2016 and April 29, 2016, we conducted an online survey and computer-assisted personal interviews (CAPI) with adults aged 40–79 years who live in 15 metropolitan cities in Korea, using structured questionnaires. For respondents aged ≥ 60 years, the self-written CAPI was administered by trained interviewers, considering their limited online access and understanding of questionnaire items. The sample size was 3,000 (95% confidence level standard error ± 1.79%), and the sampling method was simple randomization according to sex, age, and residential area in proportion to the resident registration demographic data of the Korean Ministry of Interior and Safety as of March 2016.
On obtaining consent, all participants were surveyed using the Korean version of the PUF Patient Symptom Scale17 to determine the prevalence and severity of BPS-like symptoms. Additional questionnaires for demographic characteristics were investigated as follows: sex, age, residential area, marital status, education level, current smoking and alcohol consumption status, history of taking antimicrobials related to urinary problems in the preceding 1 month, and diagnosis/treatment for IC. To assess the relationship between the degree of depression and the PUF scale, all participants were examined using the Geriatric Depression Scale (GDS), a self-reported assessment tool for identifying depression in the elderly.
Definitions and outcome measures
The primary outcome of the present study was the prevalence of BPS-like symptoms, defined as a total PUF score of ≥ 12.18 The GDS scores can be divided into four groups: normal, 0–4; mild depression, 5–8; moderate depression, 9–11; and severe depression, 12–15.
Statistical analysis
All statistical analyses were performed using the statistical software SPSS version 20.0 (IBM, Armonk, NY, USA). Statistical comparisons of the PUF scores between groups were conducted using the independent t-test and one-way analysis of variance test for continuous variables. For categorical variables, the Z-test was performed to compare the prevalence of BPS-like symptoms (PUF score ≥ 12) between the groups. A P value < 0.05 was considered statistically significant.
Ethics statement
The present study was approved by the Kyung Hee University Hospital Institutional Review Board (IRB numbers: 2021-07-050) and followed the provisions of the Declaration of Helsinki (revised, Edinburgh 2000). This study is based only on retrospective analysis of results of online survey and CAPI with adults, and there is no minimum risk to subjects during the study. Therefore, this study was exempted from obtaining informed consent after IRB review.
RESULTS
Sample description
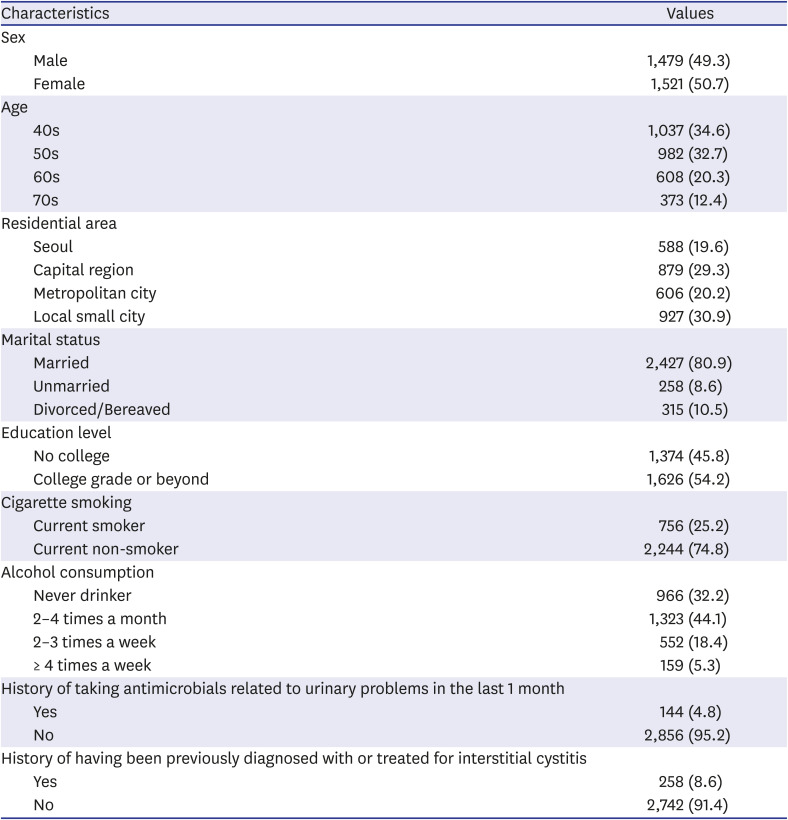
We analyzed a sample of 3,000 adults who participated in the survey among the panels owned by Hankook Research. Table 1 presents the demographic characteristics of the participants. There were 1,479 (49.3%) males and 1,521 (50.7%) females. A total of 1,037 (34.6%) participants were in their 40s, 982 (32.7%) were in their 50s, 608 (20.3%) were in their 60s, and 373 (12.4%) were in their 70s, respectively. Based on the marital status, 2,427 (80.9%) participants were married, 258 (8.6%) were unmarried, and 315 (10.5%) were divorced/bereaved. Among the participants, 144 (4.8%) had a history of taking antimicrobials related to urinary problems in the last 1 month, and 258 (8.6%) had a history of having been previously diagnosed with or treated for IC.
Table 1
Participant demographic characteristics
Relationship of BPS symptom severity to sex, age, and GDS
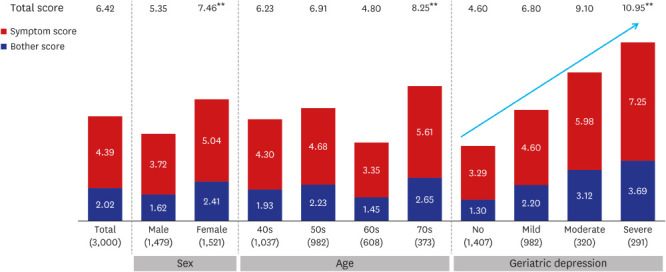
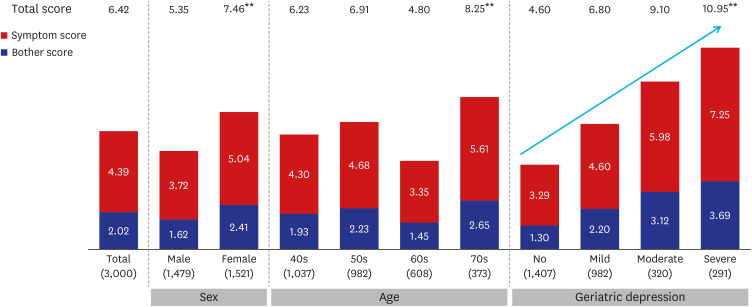
Fig. 1 presents the PUF scores according to sex, age, and GDS. The mean PUF score was significantly higher for women than for men (7.46 ± 5.11 vs. 5.35 ± 4.65, P < 0.01). The mean PUF score by age was the lowest in the 60s, and significantly higher in the 70s than in the other age groups (P < 0.01). The mean PUF score tended to increase significantly as the severity of depression increased on the GDS (P < 0.01).
Fig. 1
PUF Patient Symptom Scale according to sex, age, and the Geriatric Depression Scale (Total respondents, n = 3,000; Unit: points). Statistical significance of the difference in the PUF Patient Symptom Scale: independent t-test, analysis of variance (**P < 0.01). Arrows indicate that there is a linearly significant difference.
PUF = Pelvic Pain and Urgency/Frequency.
Prevalence of BPS-like symptoms according to the PUF Patient Symptom Scale
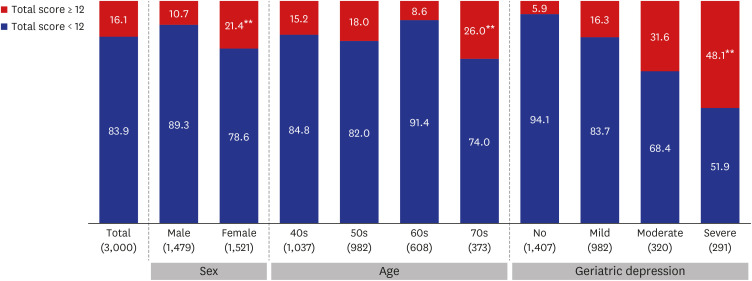
Fig. 2 shows the prevalence of BPS-like symptoms based on the PUF scale. Overall, the prevalence of BPS-like symptoms was 16.4% (483 of 3,000 participants). Women (21.4%) had a significantly higher prevalence of BPS-like symptoms than men (10.7%) (P < 0.01). The prevalence by age was the lowest in the 60s and significantly higher in the 70s than in the other age groups (P < 0.01), and was 15.2% in the 40s, 18.0% in the 50s, 8.6% in the 60s, and 26.0% in the 70s, respectively. The prevalence of BPS-like symptoms increased significantly with the increasing severity of depression on the GDS (P < 0.01). The prevalence was 5.9% in the normal group, 16.3% in the mild depression group, 31.6% in the moderate depression group, and 48.1% in the severe depression group, respectively. The prevalence of BPS-like symptoms based on marital status was significantly different; that is, the prevalence among divorced/bereaved individuals (22.3%) was higher than that among married (15.7%) or unmarried individuals (12.7%, P < 0.01). Participants who had a history of taking antimicrobials related to urinary problems in the last 1 month (58.6% vs. 14.0%, P < 0.01) or who had a history of having been previously diagnosed with or treated for IC (42.5% vs. 13.6%, P < 0.01) had a higher prevalence than those who did not.
Fig. 2
Prevalence of bladder pain syndrome-like symptoms according to the PUF Patient Symptom Scale (Base: Total respondents, n = 3,000; Unit: %). Statistical significance of the difference in the PUF Patient Symptom Scale: Z-test (**P < 0.01). Bladder pain syndrome-like symptoms was defined as the PUF total score ≥ 12.
PUF = Pelvic Pain and Urgency/Frequency.
DISCUSSION
Many epidemiological studies have determined the prevalence of BPS.4567891011121314 However, even the terms describing this condition have not been standardized, and the inconsistency in the definitions and diagnostic criteria makes it challenging to assume that the results of previous studies indicate the actual prevalence of the disease.14 Since BPS is a chronic disorder diagnosed from its clinical symptoms, recent studies have screened BPS-like symptoms using validated symptom questionnaires such as the OLS index and PUF scale; however, these may be limited in terms of completely screening the disease.481112131415
The OLS index was developed to identify pain and voiding symptoms that are commonly complained in patients with IC; however, it does not address pelvic pain or sexual intercourse-related symptoms other than bladder pain; therefore, the prevalence of BPS may have been underestimated.416 Most population-based studies using the OLS index found that the prevalence of BPS-like symptoms was 0.26–0.57% among women.8111213 In a study using the OLS index for the general population of South Korea, the prevalence of BPS-like urinary symptoms among adult women was 0.26%, which was apparently lower than that in the United States and Europe, and similar to that in Japan.14
Parsons et al.16 developed the PUF Patient Symptom Scale, a symptom questionnaire that focused on gynecologic issues (pelvic pain, especially pain and symptoms related to sexual intercourse), and urologic issues (urinary urgency and frequency) based on their clinical experiences. The PST seems to be a highly specific test for detecting a bladder-origin problem and is positive in approximately 80% of patients with IC.192021 The PUF scale was remarkably effective in predicting positive PST in urologic patients with suspected IC and gynecologic patients with pelvic pain.16 The previous finding that 85% of gynecologic patients with pelvic pain had a positive PST suggests that nearly 22% of women in the general population may have IC clinically based on the PUF scores.1622 In a population-based survey using two questionnaires, the prevalence of BPS-like symptoms among US women was only 0.57% according to the results of the OLS index, but was significantly different at 12.6% when assessed according to the PUF scale scores.11 In the present study of both men and women aged 40–79 years, the prevalence of BPS-like symptoms among Korean adults was 16.4% (483 of the 3,000 individuals), which was higher than that among US women. As per most studies, BPS is a disorder that occurs mainly in women, with the ratio being 5:1 or higher.23 In our results, the prevalence of BPS-like symptoms was 21.4% among women and 10.7% among men, approximately twice as high as that in women.
In the present study, the prevalence of BPS-like symptoms increased significantly with the increasing severity of depression on the GDS, and differed according to marital status; that is, the prevalence among divorced/bereaved individuals was significantly higher than that among married or unmarried individuals. Psychological factors may have affected the occurrence of BPS-like symptoms.
Our data were collected using a symptom-based questionnaire, and the presence of BPS-like symptoms was determined based on patient self-reports and not on clinical diagnosis or urological examination. However, BPS is diagnosed based on symptoms, and its diagnostic criteria have not been established. To the best of our knowledge, this is the first report to evaluate the prevalence of BPS-like symptoms among adults in the Korean general population using the PUF scale. To investigate a reliable prevalence and identify sufficient cases, we commissioned a survey from a professional opinion research firm.
Our large, representative population-based study showed that BPS-like symptoms are widespread in the general population of South Korea, as assessed by the PUF Patient Symptom Scale. These results suggest that the prevalence of BPS-like symptoms among Korean women may have been underestimated in a previous study based on the results of the OLS questionnaire, which reported a prevalence of 0.26%.14 BPS is a disease that deserves more attention as it is far more common than previously thought and can negatively affect many people's quality of life.
 XML Download
XML Download