

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has rapidly spread worldwide.12 It is vital for clinicians to figure out how pre-existing comorbidities affect the infectivity risk and outcomes for this new, rapidly disseminating disease. Previous studies between liver disease and COVID-19 focused on hepatic manifestations of COVID-19 (such as elevated liver enzyme and COVID-19 induced hepatitis3) and pre-existing hepatic comorbidities including liver cirrhosis,4 liver-transplant recipient,5 and chronic liver disease.6 However, studies involving non-alcoholic fatty liver disease (NAFLD) have not evaluated the severity of COVID-19 completely; there is also no study focusing on the association between SARS-CoV-2 susceptibility and pre-existing NAFLD.5
NAFLD has a high prevalence and is the most common cause of chronic liver injury, but it has been underestimated over the past decades.78 As NAFLD is a metabolic disease that is not confined to the liver, it is associated with extra-hepatic manifestations, liver-related events, and mortality.7 Among patients with COVID-19, common findings include a 14–53% increase in liver enzyme levels,5 and the most common post-mortem histopathologic findings of the liver showed moderate macrovesicular steatosis and mild lobular inflammation.9 We believe that underlying NAFLD, which is characterized by predominant macrovesicular steatosis of the liver parenchyma, could be vulnerable to the attack of SARS-CoV-2.10
Thus, we hypothesized that the presence of NAFLD can influence the epidemiological aspects related to COVID-19, including infectivity and disease-related outcomes. For this reason, we aim to investigate the potential associations on COVID-19 infectivity, severity, and related death among NAFLD patients who underwent laboratory SARS-CoV-2 testing through a population-based, nationwide cohort in South Korea.
METHODS
Database
We conducted a population-based cohort study using data from the Korean National Health Insurance Service (KNHIS), which is linked to national COVID-19-related registers from the Korea Disease Control and Prevention Agency (KDCA). It provided the data of individuals who underwent SARS-CoV-2 testing in South Korea between January 1 and May 30, 2020 by medical or KDCA referral (excluding self-referral). The KNHIS covers almost 98% of the total Korean population,111213 and the Korean government provided mandatory and complementary health insurance for all COVID-19 patients during the pandemic.14 Data from the KNHIS included demographic characteristics, general health screening records, and medical history of inpatients and outpatients; on the other hand, COVID-19-related outcomes and death were taken from the KDCA data. This nationwide cohort dataset is anonymized using patient identifiers.
Study population
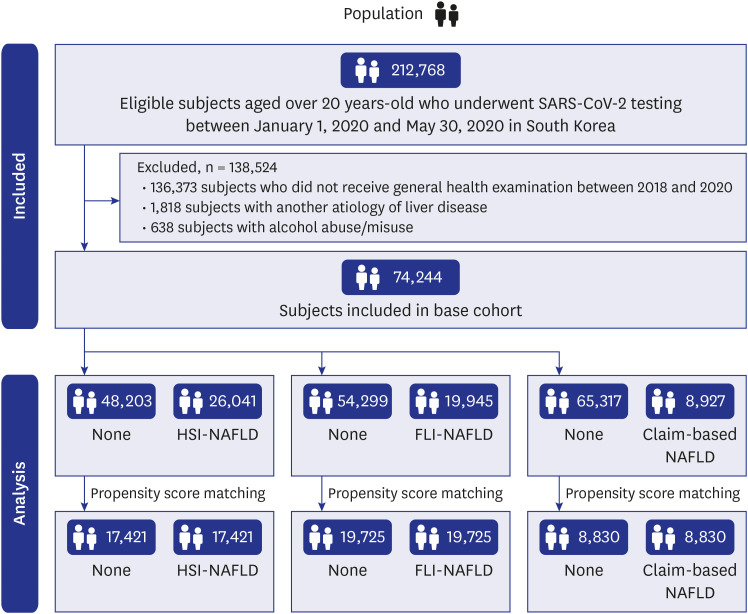
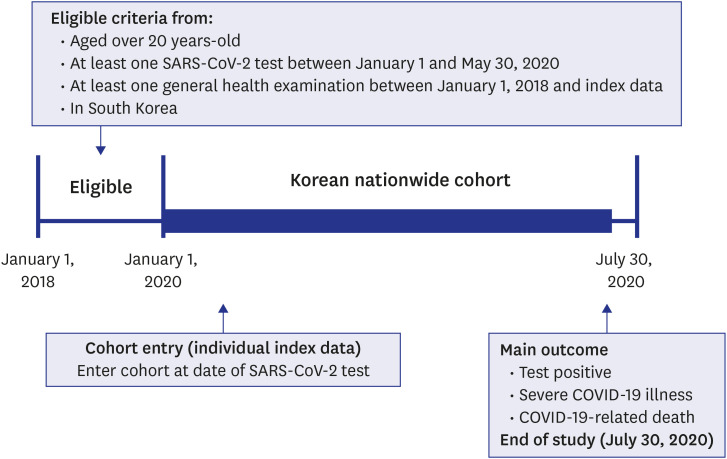
The preliminary results of our research have been published previously.15 All Korean individuals ≥ 20 years of age who underwent SARS-CoV-2 testing between January 1, 2020 and May 30, 2020 by medical or KDCA referral (excluding self-referral; n = 212,768) were enrolled. Among the 212,768 included subjects, subjects who did not recently receive general health examination (n = 136,373), those with another etiology of chronic liver disease (n = 1,818), and those with alcohol abuse/misuse (those with alcohol-related disease [F10.0, F10.1, F10.3, F10.4, F10.5, F10.6, F10.7, F10.8, F10.9, G62.1, K70.x, K70.0, K70.1, K70.2, K70.3, K70.4, K70.9, K86.0] and those who had alcohol intake more than 210 g [for men] and 140 g [for women] per week; n = 638) were excluded from the study. After exclusion, 74,244 subjects were available for analysis. A positive SARS-CoV-2 test was confirmed by real-time reverse transcriptase-polymerase chain reaction assay of the specimen from nasal and pharyngeal swabs, which was authorized by the KDCA.16 The observational period was from January 1, 2020 to July 30, 2020, and individual index data was the data of the first SARS-CoV-2 testing for each patient.
Insurance eligibility data offered the baseline personal data such as age, gender, household income, and region of residence.111718 The history of diagnosed comorbidities such as diabetes mellitus, tuberculosis, stroke, cardiovascular disease, hypertension, dyslipidemia, and current medication history for those diseases were also available from the general health examination that had been obtained through a personal medical interview. Lifestyle habits, such as smoking, alcohol consumption, and physical activity level, were also accessible from the general health examination.11 The body mass index (BMI), waist circumference (WC), and systolic/diastolic blood pressure were taken for all the patients. Laboratory data, including blood glucose, creatinine (used for glomerular filtration rate [GFR] calculation), aspartate transaminase (AST), alanine transaminase (ALT), triglyceride and gamma-glutamyl transferase (GGT), were obtained from a serum sample in the fasting state during general health examination.11
NAFLD definition (exposure)
Patients were divided according to the three types of NAFLD definition. Pre-existing NAFLD was regarded when one of the following criteria was satisfied: 1) hepatic steatosis index (HSI) ≥ 36, 2) fatty liver index (FLI) ≥ 60, or 3) claim-based definition indicated by the International Classification of Diseases, 10th revision (ICD-10) (K75.8 and K76.0), with at least one claim within the observation period.19 HSI was calculated based on AST, ALT, BMI, female sex, and diabetes mellitus using the following formula20: HSI = 8 × ALT/AST ratio + BMI (+2, if diabetes mellitus; +2, if female). FLI was calculated based on BMI, WC, GGT, and triglyceride level by the following formula20:

We calculated the BARD score to estimate the degree of fibrosis of NAFLD patients. The BARD score was calculated using BMI, AST, ALT, and presence of diabetes mellitus; NAFLD patients were categorized as those without advanced fibrosis (0–1) or those with advanced fibrosis (2–4).21
We generated three cohorts using these definitions to support the robustness and generalization of our results: 1) adaptation of HSI for NAFLD definition (HSI-NAFLD cohort), 2) adaptation of FLI for NAFLD definition (FLI-NAFLD cohort), and 3) adaptation of claim-based NAFLD definition (claim-based NAFLD cohort).
Outcomes
The study subjects were linked to the national COVID-19-related registers from the KDCA. The main outcomes were the positive laboratory SARS-CoV-2 tests, severe clinical COVID-19 illnesses (requirement of oxygen therapy, administration of mechanical ventilation, international care unit admission, COVID-19-related death),1622 and COVID-19-related deaths.
Statistical analysis
In this nationwide cohort, pre-existing NAFLD was defined as the “exposure” and positive SARS-CoV-2 tests or COVID-19-related outcomes were defined as the “outcomes”. We generated three exposure-driven propensity score matched cohorts to provide the robustness and generalization of our results. First, we performed 1:1 ratio of the exposure-driven propensity score matching using a “greedy nearest-neighbor” algorithm to balance the baseline and demographic covariates of the two groups and to reduce potential confounders from the predicted probability of 1) patients with HSI-NAFLD vs. those without HSI-NAFLD (HSI-NAFLD cohort), 2) patients with FLI-NAFLD vs. those without FLI-NAFLD (FLI-NAFLD cohort), and 3) patients with claim-based NAFLD vs. those without claim-based NAFLD (claim-based NAFLD cohort). We selected the following matching covariates: age (20–39, 40–59, and ≥ 60 years), sex, region of residence (Seoul Capital Area, Daegu/Gyeongbuk area, and other areas), past medical history/comorbidities (tuberculosis, stroke, cardiovascular disease, hypertension, and dyslipidemia), systolic and diastolic blood pressure, fasting blood glucose, GFR (≥ 90, 60–89, ≤ 59 mL/min), household income (low, middle, and high), smoking (never, ex-, and current), alcoholic drinks (< 1, 1–2, 3–4, ≥ 5 days per week), sufficient aerobic activity (more than 500 metabolic equivalent task min/week), and current medication for hypertension, dyslipidemia, diabetes mellitus, and cardiovascular disease. We excluded the adjusted variables used in HSI, FLI, and BARD score (history of diabetes mellitus, WC, BMI, serum triglyceride, GGT, AST, and ALT) to avoid over-adjustment.
Subsequently, we used Firth logistic regressions to reduce the small sample bias, presented by adjusted odds ratios (aORs) with 95% confidence intervals (CIs) after adjusting for the potential confounders. We performed the main analyses from 1) HIS-NAFLD matched cohort (n = 34,842); 2) FLI-NAFLD matched cohort (n = 39,450); and 3) claims-based NAFLD matched cohort (n = 17,660). To investigate the severity-dependent relationship, we performed further analyses from the fully unmatched cohort, which were re-categorized as severity according to the BARD score (none vs. NAFLD without advanced fibrosis vs. NAFLD with advanced fibrosis).
Standardized mean differences (SMDs), score densities, and score distributions were used for determining adequacy of propensity score matching. An SMD of less than 0.1 was considered to have no major imbalance between matched pairs; a two-sided P value of less than 0.05 was considered statistically significant. Statistical analyses were performed in SAS (version 9.4; SAS Institute Inc., Cary, NC, USA) and R software version 3.6.1 (R Foundation, Vienna, Austria).
RESULTS
Descriptive overview
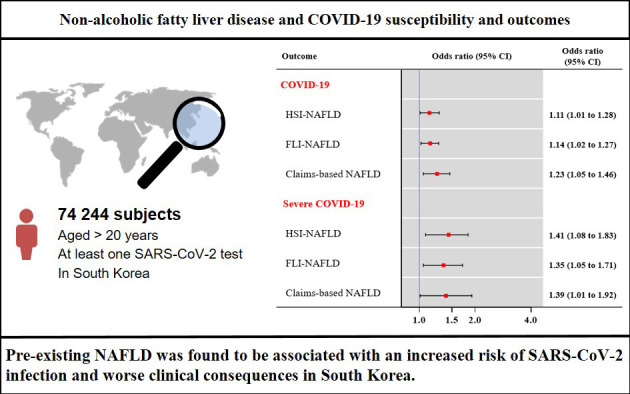
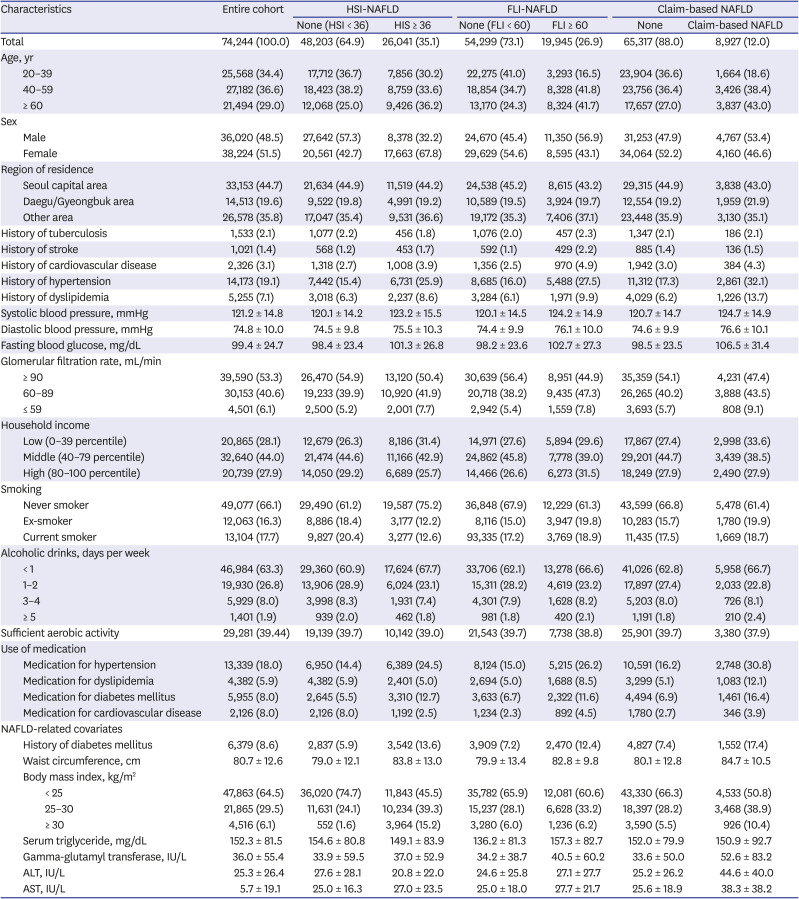
Baseline characteristics of subjects are summarized in Table 1. Among 74,244 adults (age groups: 34.4% [20–39 years], 36.6% [40–59 years], and 29.0% [≥ 60 years], 36,060 were male [48.5%], and 26,041 (35.1%), 19,945 (26.9%), and 8,927 (12.0%) subjects had HSI-NAFLD, FLI-NAFLD, and claims-based NAFLD, respectively (Table 1 and Fig. 1). During the observation period (Fig. 2), 2,251 (3.0%) tested positive for SARS-CoV-2, 438 (0.6%) had severe COVID-19 illness, and 45 (0.06%) suffered COVID-19-related deaths.
Table 1
Baseline characteristics of subjects who performed the SARS-CoV-2 testing in the Korean nationwide cohort (n = 74,244)
HSI-NAFLD cohort
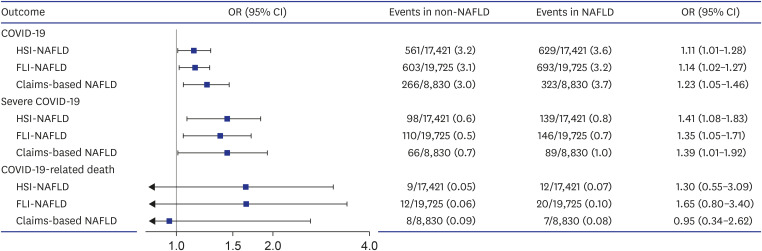
After 1:1 propensity score matching in HSI-NAFLD cohort (17,241 for patients without HSI-NAFLD vs. 17,241 for those with HSI-NAFLD), there was no distinct imbalance between the baseline characteristics (Supplementary Table 1, Fig. 3, and Supplementary Fig. 1; all SMDs < 0.09). In the matched cohort, subjects with HSI-NAFLD had a high risk of COVID-19 infection (3.2% for subjects without HSI-NAFLD vs. 3.6% for those with HSI-NAFLD; aOR, 1.11; 95% CI, 1.01–1.28) and severe COVID-19 disease progression (0.6% vs. 0.8%; aOR, 1.41; 95% CI, 1.08–1.83).
Fig. 3
The association between NAFLD and positive SARS-CoV-2 test results, severe COVID-19 illness, and COVID-19-related death in nationwide cohort of South Korea.
The x-axis indicates a log-scale; horizontal bars denote 95% CIs for each of the results; and blue dots indicate propensity score matched results. Severe COVID-19 comprised requirement of oxygen therapy, admission to the intensive care unit, invasive ventilation, or death. The figure was generated from our previous research and made further advance.15
COVID-19 = coronavirus disease 2019, HSI = hepatic steatosis index, FLI = fatty liver index, NAFLD = non-alcoholic fatty liver disease, OR = odds ratio, CI = confidence interval, SARS-CoV-2 = severe acute respiratory syndrome coronavirus 2.
FLI-NAFLD cohort
Results showed consistent tendency after 1:1 propensity score matching, with 19,725 pairs produced. There were no major imbalances of baseline characteristics (Supplementary Table 2, Fig. 3, and Supplementary Fig. 2; all SMDs < 0.05). In FLI-NAFLD group, COVID-19 infection (aOR, 1.14; 95% CI, 1.02–1.27) and progression to severe COVID-19 (aOR, 1.35; 95% CI, 1.05–1.71) were more commonly observed on patients with FLI-NAFLD than those without FLI-NAFLD.
Claim-based NAFLD cohort
After 1:1 propensity score matching as 8,830 pairs without major imbalance (Supplementary Table 3, Fig. 3, and Supplementary Fig. 3; all SMDs < 0.07), confirmed COVID-19 infection (aOR, 1.23; 95% CI, 1.05–1.46) and severe COVID-19 illness (aOR, 1.39; 95% CI, 1.01–1.92) were more commonly observed in NAFLD patients.
Severity-dependent analysis
In the full unmatched cohort after stratifying the subjects with NAFLD according to the estimated degree of fibrosis using BARD score (Table 2), subjects in advanced fibrosis group tended to be more infected with COVID-19 (HSI-NAFLD aOR, 1.20; 95% CI, 1.06–1.34; FLI-NAFLD aOR, 1.32; 95% CI, 1.11–1.59; and claims-based NAFLD aOR, 1.26; 95% CI, 0.98–1.61) compared to those without NAFLD. Severity steadily trended upward. Similar severity-tendency was observed in experiencing severe COVID-19 and COVID-19 related death. Subjects having pre-existing NAFLD with advanced fibrosis had a risk for their COVID-19 disease to progress severely (HSI-NAFLD aOR, 1.79; 95% CI, 1.37–2.30; FLI-NAFLD aOR, 1.89; 95% CI, 1.33–2.70; and claims-based NAFLD aOR, 2.60; 95% CI, 1.77–3.89) and a higher risk for COVID-19 related death (HSI-NAFLD aOR, 4.42; 95% CI, 2.27–8.61; FLI-NAFLD aOR, 7.06; 95% CI, 3.49–14.70; and claims-based NAFLD aOR, 5.12; 95% CI, 2.23–12.95).
Table 2
Severity-dependent association between risk of the COVID-19-related outcomes and NAFLD by BARD scoring system in the Korean nationwide cohort (total n = 74,244)
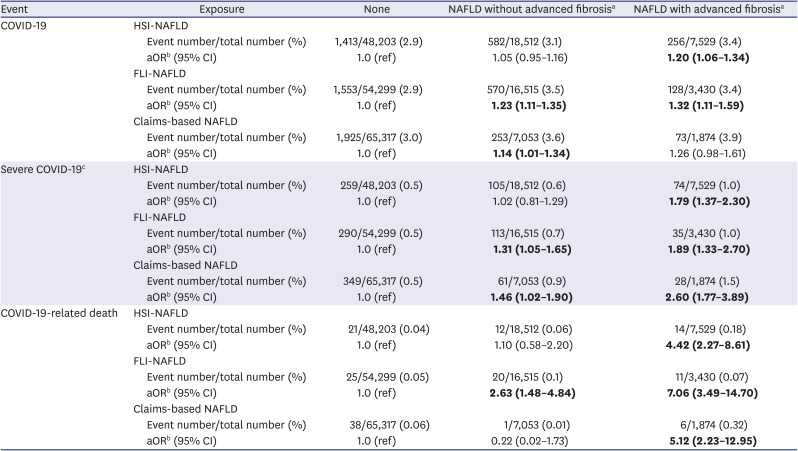
Numbers in bold indicate significant differences (P < 0.05).
COVID-19 = coronavirus disease 2019, NAFLD = non-alcoholic fatty liver disease, FLI = fatty liver index, HSI = hepatic steatosis index, aOR = adjusted odds ratio, CI = confidence interval.
aWe were categorized as severity of liver fibrosis according to the BARD score (0–1, no advanced fibrosis; 2–4, advanced fibrosis); bAdjusted for age (20–39, 40–59, and ≥ 60 years); sex; region of residence (Seoul Capital Area, Daegu/Gyeongbuk area, and other areas); past medical history/comorbidities (tuberculosis, stroke, cardiovascular disease, hypertension, and dyslipidemia); systolic and diastolic blood pressure (continuous); fasting blood glucose (continuous); glomerular filtration rate (≥ 90, 60–89, and ≤ 59 mL/min); household income (low, middle, and high); smoking (never, ex-, and current); alcoholic drinks (< 1, 1–2, 3–4, ≥ 5 days per week); sufficient aerobic activity; current medication for hypertension, dyslipidemia, diabetes mellitus, and cardiovascular disease; cSevere outcomes of COVID-19 comprised requirement of oxygen therapy, admission to the intensive care unit, invasive ventilation, or death.
DISCUSSION
Through a large-scale, population-based, nationwide cohort study, we investigated the potential association between the presence of NAFLD and risk of SARS-CoV-2 test positive and COVID-19 severity and mortality. We identified that the presence of NAFLD affected the increased SARS-CoV-2 infectivity and COVID-19 severity among 74,244 subjects underwent SARS-CoV-2 testing in South Korea. Additionally, these results found that the severity-dependent association between NAFLD severity and aforementioned COVID-19-related outcomes become more pronounced as liver fibrosis advances. Regarding the robustness and generalization of our results, we performed several sensitivity analyses using the alternative definitions, such as FLI-NAFLD, HSI-NAFLD, and claims-based NAFLD, which were consistent with our main results.
Since the novel pandemic of COVID-19, many researchers have studied the epidemiologic features of COVID-19 (especially severity), focusing on severe liver disease including chronic liver disease,6 liver cirrhosis,4 and transplant recipients.5 Although NAFLD is a hepatic manifestation of metabolic syndrome and the most common cause of chronic liver disease,22 there are some available studies with relatively small sample sizes23 for patients with NAFLD on the disease course of COVID-19 and still remains unclear: predictive factors24 associated with COVID-19 severity in USA (n = 351), China (n = 202), and Israel (n = 71), and non-relevant factors in USA (n = 589),23 U.K.(n = 193),25 China (n = 280),26 and Mexico (n = 432).27 Most recent data has focused on whether underlying hepatic steatosis has an impact on the clinical course of the patients with COVID-19, which may not identify the SARS-CoV-2 infectivity of the patients having underlying NAFLD.24 To the best of our knowledge, this the first study to investigate the association between the likelihood of testing positive for SARS-CoV-2 and pre-existing NAFLD, which may indicate that the natural course of SARS-CoV-2 infection is exacerbated and mediated by systemic and chronic inflammation of pre-existing NAFLD. Previous studies that demonstrated the association between pre-existing NAFLD and COVID-19 severity had limitations due to the cohort size, non-representative sampling (sample number, 70 to 600), and naïve NAFLD definition using only HSI or hepatic steatosis measurement using concurrent computed tomography (CT) scan.2324252627 In a COVID-19 patient, it is difficult to distinguish the concomitant liver injury using a CT scan; therefore, it is difficult to evaluate their baseline liver steatosis before SARS-CoV-2 infection. Additionally, insufficient response effort as important potential confounders (i.e., smoking status, physical activity, and alcohol consumption) and selection bias from retrospective clinic-based sampling and using non-sophisticated statistical techniques.2324252627 Thus, these findings were difficult to use in the evaluation of the direct effects of underlying NAFLD and may be less generalizable and reliable. For these reasons, there was a demand for large-scale and well-designed research to clarify the implications for pre-existing NAFLD. In our study, we founded that pre-existing NAFLD was associated with severe COVID-19 illness and death, similar to previous studies24; additionally, pre-existing NAFLD was found to be associated with an increased risk of COVID-19 infectivity.
Our results for the increased risk of COVID-19-related death was significant only in the fully unmatched cohort. Taking into consideration that the association between COVID-19 severity and pre-existing NAFLD was significant, the insignificant relationship between COVID-19-related death and pre-existing NAFLD was caused by the lack of sample number; there were only 45 (0.06%) COVID-19-related deaths.
The precise disease interaction mechanism has not been clearly identified, but it is thought to be related to the assumptions as follows: firstly, patients with NAFLD has dysregulated innate immunity,3 which may induce the increased release of proinflammatory cytokines such as tumor necrosis factor alpha and interleukin-6.28 These upregulations trigger cytokine storm, a state that may contribute to severe disease progression of COVID-19.28 Additionally, several NAFLD-related mechanisms such as sterol regulatory element binding protein-2 activation, altered lipid synthesis, and liver X-receptor activation may increase the inflammatory immune response, which may lead cytokine storm in SARS-CoV-2 infection.29 In addition to these immune responses, the polarization of Kupffer cells could alter the inflammation, promoting M1 to inflammation-suppressing M2; this results in the virulence of SARS-CoV-2, and could therefore induce the uncontrolled viral replication and cellular damage of the organs.3
Secondly, NAFLD has increased hepatic expression of critical entry points. SARS-CoV-2 may enter the cells through angiotensin-converting enzyme 2 receptors (ACE2), which is mainly expressed in cholangiocytes and hepatocytes.30 Upregulation of hepatic ACE2 was observed in patients with chronic liver disease; thus, these could affect the SARS-CoV-2 infectivity and COVID-19 severity in NAFLD patients.530 As severe Middle East respiratory syndrome or severe acute respiratory syndrome-1 showed liver injury upon post-mortem biopsies, many cases of SARS-CoV-2 showed similar liver injury.331 The liver injury, which is a common finding in patients with severe COVID-19 illness, is most likely caused by immune-mediated systemic inflammation.3 Dysregulated immunity caused by NAFLD could make more the patient more susceptible to COVID-19 associated liver injury. Liver damage induced by pre-existing NAFLD and SARS-CoV-2 might share the immunologic mechanism and occur synergistically. This could be a plausible explanation for why patients with NAFLD are more vulnerable to SARS-CoV-2 infection and severe COVID-19 outcomes.
There are several limitations to this study. Firstly, we defined NAFLD based on the combination of clinical data, lab data, and ICD code in insurance claims-based data. Our data did not include information from imaging modalities (i.e., ultrasonography, CT, shear wave elstography) or pathologic data. However, we defined NAFLD using the three classifications (HSI, FLI, and ICD-10 code), and each of them showed consistent association with COVID-19. Recent data also suggested that they showed high diagnostic performance, with their c-statistics being 0.85 for FLI and 0.75 for HSI.32 Adopting three definitions for NAFLD reduced the risk for overestimation or underestimation.
Secondly, the progressive form of NAFLD (nonalcoholic steatohepatitis) was not fully evaluated, and most of the surrogate serum markers for fibrosis (NAFLD fibrosis score, Fibrosis-4 score, European Liver Fibrosis, or FibroTest) could not be calculated because the nationwide data did not include platelet count or apolipoprotein A1. Instead, we calculated the BARD score to measure NAFLD fibrosis to overcome this issue.21 Further studies with detailed analyses for fibrosis on this group of patients are warranted. Thirdly, although we used the national level dataset, this dataset did not include the individual data of viral loads and contact tracing; therefore, the SARS-CoV-2 test positive results should be interpreted carefully. Finally, our results reflected the initial COVID-19 pandemic in South Korea, and the generalization of our results should be taken with a grain of salt since the COVID-19 vaccine is now available.33
The preliminary results of our research have been published previously.15 Previous results published crude cohort research in short letter format,15 this study have investigated using sophisticated statistical techniques (strict exposure-driven propensity score matching method).
Despite these limitations, the main strengths of our study include the use of a nationwide cohort with a representative sample size (n = 74,244 subjects), several NAFLD definitions, strict exposure-driven propensity score matching (three matched cohorts), and various potential confounding factors from the general health examination records (i.e., physical activity, alcohol consumption, smoking status, household income). Our nationwide study provides the first evidence of the contribution of pre-existing NAFLD to an increased likelihood of SARS-CoV-2 infection and severe COVID-19 outcomes.
In conclusion, through large-scale, population-based, nationwide cohort study, we investigated the potential association between the presence of NAFLD and risk of an increased likelihood of SARS-CoV-2 infection and severe COVID-19 outcomes. Pre-existing NAFLD was found to be associated with an increased risk of SARS-CoV-2 infection and worse clinical consequences in South Korea. These associations between positive SARS-CoV-2 tests and COVID-19 severity and mortality become more pronounced as liver fibrosis progresses. Our study provides an advanced insight of the contribution to pre-existing NAFLD and COVID-19 pathogenesis. Our results suggest that physicians should exercise extra care and give more attention to COVID-19 patients with pre-existing NAFLD.
 XML Download
XML Download