

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Management of the coronavirus disease 2019 (COVID-19) pandemic is a major public health concern in many countries. Although individuals are recommended to adhere to preventive measures such as wearing of face mask and social distancing, prescreening of those who are likely to be infected with COVID-19 before entry is often implemented in public places, such as shopping centers, schools, and places of worship.1 Hospitals are particularly at a high risk of transmission of COVID-1923; thus, most hospitals have established a prescreening process for all patients and accompanying guardians in emergency departments as well as in outpatient clinics. Prior to entering a hospital building, individuals are assessed to identify whether they have been exposed to COVID-19 or have symptoms indicative of COVID-19. Individuals with any exposure history or symptoms indicative of COVID-19 are not allowed to enter the hospital and are instead requested to visit an outside screening center (OSC).45 However, cases might be missed during the prescreening process for various reasons; for example, some individuals are not honest about their medical history, or the infrared thermo-scanning camera might not detect fever.6 A COVID-19 case missed at prescreening could result in nosocomial transmission.
In Eunpyeong St. Mary's Hospital, in Korea, a two-level COVID-19 prescreening process was established in the outpatient clinic. The first level was a prescreening process at the entrance of the outpatient clinic (PPEO). For those who passed the PPEO and entered the hospital building, a second prescreening process was repeated in each department. Hospitals have an emergency code process (such as a code blue for a patient in cardiac arrest) for a COVID-19 suspect. If a COVID-19 suspected individual is found in the second prescreening, a “code apple” process alerts the medical staff, the identified person was escorted to the OSC by medical and security personnel using a designated aisle and elevator. Once in the OSC, the identified person was asked to undergo diagnostic testing for COVID-19.7
In this study, we aimed to analyze the cases missed by the PPEO that caused a code apple to be applied retrospectively. Information obtained from this study can provide insights or recommendations in improving prescreening processes in healthcare facilities.
METHODS
Study site
This study was conducted at an 808-bed regional referral university hospital in Korea. This hospital serves as a major medical facility for more than 900,000 people in northwest Seoul, Korea, and it has been designated as a COVID-19 treatment hospital. The hospital handles 2,500–3,000 outpatients and 500–700 inpatients daily, with 2,500 employees, including doctors, nurses, support personnel, administrative staff, and aides.
Prescreening process
The prescreening process for the hospital is illustrated in Fig. 1.
Fig. 1
Two-level prescreening process in the outpatient clinic to detect patients and accompanying guardians with suspected COVID-19. Criteria: temperature ≥ 37.5°C or ≥ 38°C (the cutoff temperature was decided according to the number of newly confirmed COVID-19 cases in Korea).
COVID-19 = coronavirus disease 2019, OSC = outside screening center.
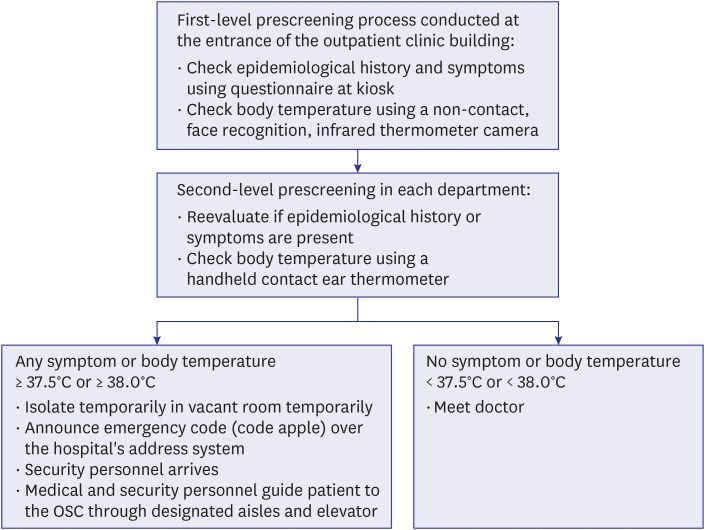
In the outpatient clinic, the first level of the prescreening process, PPEO, was placed at the entrance of the main lobby. All patients and visitors of the outpatient clinic must complete a questionnaire available at the kiosk; the questionnaire was prepared in accordance with patient evaluation defined by the Korea Disease Control and Prevention Agency (KDCA).8 The questionnaire contained items about epidemiological history (exposure to COVID-19 patients within 2 weeks, visits to places with COVID-19 outbreaks within 2 weeks, or a history of overseas travel within 2 weeks). Individuals were also asked whether they had symptoms indicative of COVID-19, including fever (≥ 37.5°C), cough, sore throat, respiratory distress, chills, myalgia, headache, anosmia, or ageusia. After visitors completed the questionnaire at a kiosk, their body temperature was measured using a non-contact, face recognition, infrared thermometer camera, Smart PassTM (AHA Information & Communication Co., Ltd., Gimpo, Korea), which was certified as a medical device by the Ministry of Food and Drug Safety (MFDS) of Korea. During use, the target person stands in front of the camera, with their forehead aimed toward the lens at a 5–8-cm distance. If the body temperature of the target person is < 37.5°C, a green backlight appears with a soft beep sound. If the body temperature of the target person is ≥ 37.5°C, a red backlight appears with an urgent beep sound. Individuals who answered yes to any of the questions at the kiosk or had a body temperature ≥ 37.5°C (the threshold defined by the KDCA) were not allowed to enter the hospital building; instead, they were guided to the OSC.
The second level prescreening process occurred at the entrance to each department. Nurses reevaluated each patient and accompanying guardian by asking again for their epidemiological history and about any symptoms indicative of COVID-19, and they manually measured visitors' body temperature using a handheld, contact ear thermometer, a Braun ThermoScan® PRO 6000 (Braun Co., Melsungen, Germany), that is also certified as a medical device by MFDS of Korea. The probe of the thermometer was placed snugly in the ear canal, and the temperature appeared on the display after the nurse pressed a button. The temperature was measured once in each ear, and the higher temperature was regarded as the target person's body temperature. If individuals reported an epidemiological history or symptoms that suggested COVID-19, or if their body temperature was ≥ 37.5°C or ≥ 38°C (the threshold varied during the study period, as explained below), the nurse implemented the code apple emergency process (Fig. 1) for that individual. Upon implementation of that code, the individual was temporarily isolated in a vacant room in the clinic. Code apple was announced over the hospital's address system, and medical and security personnel guided the individual to the OSC using a designated aisle and elevator to minimize contact with healthcare workers (HCWs), other patients, and visitors. The individual was then asked to undergo both nasopharyngeal and throat swabs in the OSC, and polymerase chain reaction (PCR) testing for COVID-19 was performed.
The body temperature criterion that triggered the emergency code process was ≥ 37.5°C or ≥ 38°C, as decided by the hospital's infection control unit to accommodate the COVID-19 dynamics in Korea at that time: ≥ 37.5°C from March 9–25, 2020; ≥ 38°C from March 26–December 28, 2020; ≥ 37.5°C from December 29, 2020. In March 2020, Korea experienced the first wave of the COVID-19 pandemic,9 and the initial criterion for the emergency code was set at ≥ 37.5°C. In late March 2020, newly confirmed COVID-19 cases decreased below 10,000 per month, which lasted from April to November,9 and by that time, HCWs were compliant in wearing personal protective equipment (PPE); thus, the criterion for the emergency code was raised to ≥ 38°C from March 26–December, 28, 2020. However, Korea experienced its third wave of the COVID-19 pandemic and newly confirmed cases surpassed 10,000 in December 20209; therefore, the criterion for the emergency code was returned to ≥ 37.5°C beginning December 29, 2020.
Study design
In this study, we reviewed data from the infection control unit of the hospital to analyze the cases missed by the PPEO that required the emergency code process to be implemented. We examined all cases from March 9, 2021 (the first day the emergency code was applied) to April 30, 2021. To improve the prescreening process (i.e., to select when or whom to pay higher attention), we investigated the incidence of cases missed by the PPEO per 1,000 outpatients and compared visits between days of the week (Monday–Tuesday versus Wednesday–Saturday, Monday–Wednesday versus Thursday–Saturday, and Monday–Thursday versus Friday–Saturday), opening hours (morning versus afternoon), and first-time visitors (had not previously received any medical service at Eunpyeong St. Mary's Hospital) versus those visiting for the second time or more (had previously received any medical service at Eunpyeong St. Mary's Hospital; also referred to as returning visitors).
Statistical analysis
Demographic characteristics, hospital visit information, and the clinical characteristics of cases missed by the PPEO are presented as frequencies with percentages for categorical variables. To compare differences in the incidence of cases missed by the PPEO between days of the week, hours visited (morning versus afternoon), and first-time and returning visitors, we also considered the number of outpatients in each category. The incidence of cases missed by the PPEO per 1,000 outpatients was calculated as the number of cases missed by the PPEO at a specific time or visit/total number of outpatients at a specific time or visit * 1,000 with a 95% confidence interval (CI). Two-proportion Z tests were used to compare proportions of cases missed by the PPEO per 1,000 outpatients. All statistical analyses were performed using Stata version 16 (Stata Corporation, Release 16, College Station, TX, USA). For all statistical analyses, P < 0.05 was considered significant.
Ethical statement
Data on cases missed by the PPEO and causing an emergency code to implemented were collected by the infection control unit of the hospital as part of its infection control practice during the COVID-19 pandemic. The use of those data in this study was approved by the Institutional Review Board of the study hospital (PC21RISI0099).
RESULTS
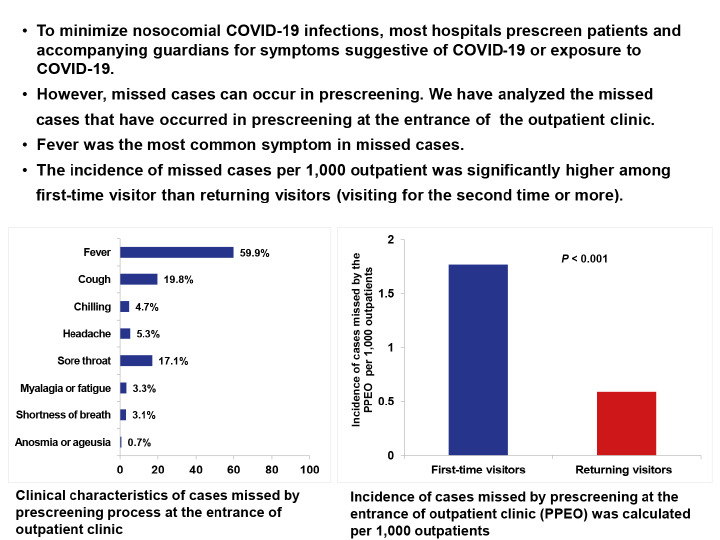
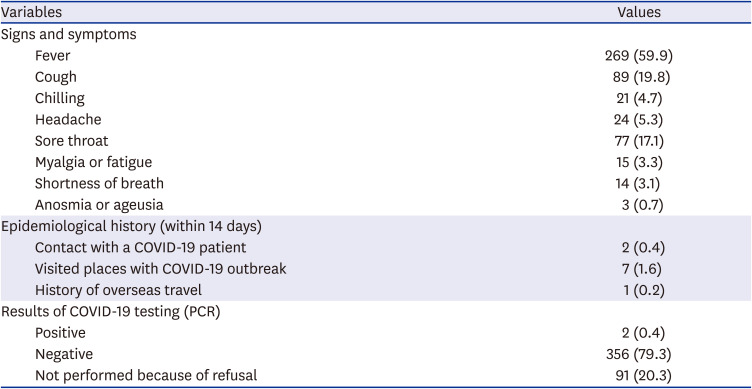
During the study period, 449 cases missed by the PPEO were recorded. Table 1 displays the demographic data and hospital visiting information for those cases. The cases were most frequently reported by otorhinolaryngology (20.7%), followed by gastroenterology (11.6%), urology (5.8%), and dermatology (5.8%). Table 2 presents the clinical characteristics of the cases missed by the PPEO. Of the 449 cases, fever was the most common symptom (59.9%), followed by cough (19.8%), sore throat (17.1%), and headache (5.3%). Ten of the missed cases had an epidemiological history (two patients had contact with a COVID-19 patient, seven had visited places with a COVID-19 outbreak, and one had a history of overseas travel). A COVID-19 PCR test was performed in 358 individuals; the test was refused by the remaining 91 individuals. Two patients had a positive COVID-19 PCR test.
Table 1
Demographic and hospital information for cases missed by the PPEO, which caused the emergency code to be applied in the hospital building (n = 449)
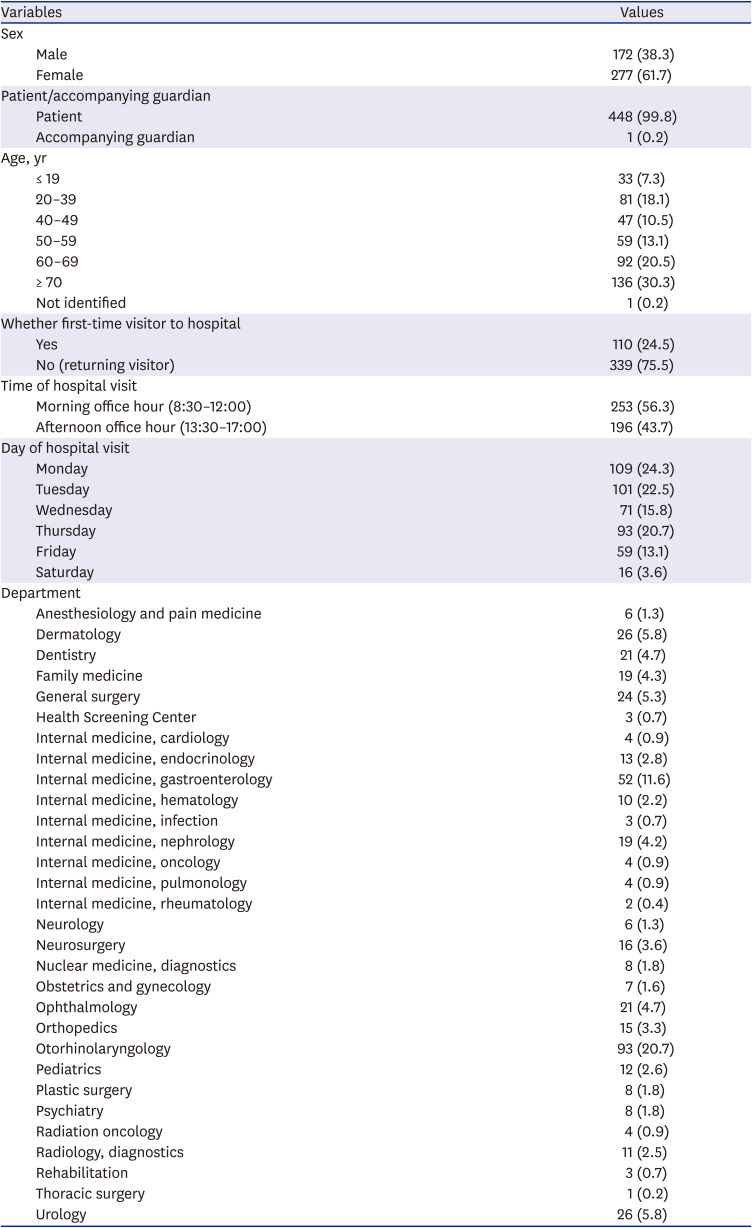
Table 2
Clinical characteristics of cases missed by the PPEO, which caused the emergency code to be applied in the hospital building (n = 449)
During the study period, the outpatient clinic was open for 339 working days, and 641,039 outpatients visited the clinic. During those working days, the two-level prescreening process was performed in the outpatient clinic to detect potential COVID-19 patients, and the emergency code process was implemented for all cases missed by the PPEO. Among the 641,039 outpatients, 62,078 were first-time visitors, and 578,961 were returning visitors. The incidence of missed cases in the PPEO per 1,000 outpatients was significantly higher among first-time visitors than among those visiting for the second time or more (1.77 [CI, 1.44–2.10] vs. 0.59 [CI, 0.52–0.65], respectively; P < 0.001) (Fig. 2A). Among the 641,039 outpatients, 381,484 visited in the morning, and 259,555 outpatients visited in the afternoon. No significant difference was observed in the incidence of cases missed by the PPEO between morning office hours and afternoon office hours (0.66 [CI, 0.58–0.74] vs. 0.76 [CI, 0.65–0.86], respectively; P = 0.172) (Fig. 2B).
Fig. 2
The incidence of cases missed in the prescreening PPEO was calculated per 1,000 outpatients. (A) Comparison between first-time visitors and returning visitors. (B) Comparison between those visiting in the morning and those visiting in the afternoon. (C) Comparison between the days of the week.
PPEO = prescreening process at the entrance of the outpatient clinic.
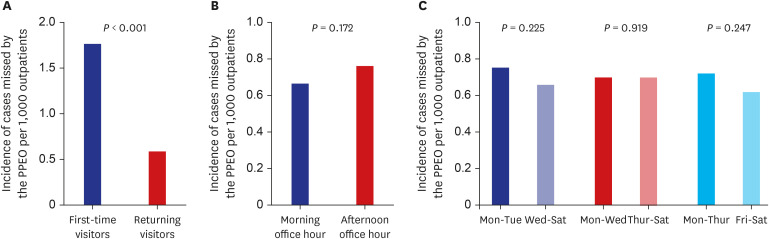
The distribution of the 641,039 outpatients according to the days of the week was as follows: 143,792 on Monday, 137,815 on Tuesday, 118,079 on Wednesday, 120,575 on Thursday, 97,727 on Friday, and 23,051 on Saturday. No significant differences were observed in the incidence of cases missed by the PPEO per 1,000 outpatients between weekdays: Monday–Tuesday versus Wednesday–Saturday (0.75 [CI, 0.65–0.85] vs. 0.66 [CI, 0.58–0.75], respectively; P = 0.225); Monday–Wednesday versus Thursday–Saturday (0.70 [CI, 0.62–0.79] vs. 0.70 [CI, 0.59–0.80], respectively; P = 0.919); Monday–Thursday versus Friday–Saturday (0.72 [CI, 0.65–0.79] vs. 0.62 [CI, 0.48–0.76], respectively; P = 0.247) (Fig. 2C).
DISCUSSION
To prevent the transmission of COVID-19 among patients and HCWs, outpatient clinics need a prescreening process. Departments such as otorhinolaryngology, pulmonary, and pediatrics provide care to patients with respiratory diseases. Face-to-face communication occurs in doctors' offices, and some procedures performed in outpatient clinics generate aerosols (e.g., nasal endoscopy, gastroendoscopy, and transesophageal echocardiogram). Furthermore, procedures such as gastroendoscopy can induce intra-procedural coughing, sneezing, or choking, and HCWs can also be contaminated by body fluid during procedures such as blood sampling.1011 The large number of outpatients in a busy clinic can often make it difficult to maintain social distancing. Because many people with COVID-19 infections are asymptomatic, pre-symptomatic, or exhibiting atypical symptoms,12 no prescreening process can identify all COVID-19 infected individuals. Even though HCWs wear PPE properly, and patients and guardians wear facemasks, exposure to cases of COVID-19 should be minimized. Therefore, procedures to prevent people likely to have COVID-19 from entering the building should be continued.
In this study, we found that fever was the most common symptom in people allowed through the PPEO but flagged in the second-level prescreening. Among the 449 cases caught at the second level, more than 20% and 10% of cases were reported by the otorhinolaryngology and gastroenterology departments, respectively. The likelihood that a case would be missed by the PPEO was significantly higher among first-time visitors than returning visitors.
Various factors could contribute to a case being missed by the PPEO; however, because fever was the most common symptom, we presume that the non-contact infrared thermometer camera was not as sensitive as the handheld contact ear thermometer for detecting fever. Non-contact infrared thermometers that read a person’s temperature from the forehead or wrist have been widely implemented in public places during the pandemic. Those instruments have certain advantages: because they do not require physical contact, the cross contamination risk is low; they measure the surface skin temperature faster than the contact checking method; and they are less costly than human resources. However, studies have reported their low sensitivity and susceptibility to the environmental temperature.1314 In this study, the non-contact infrared thermometer camera in the PPEO might have missed febrile cases. Additionally, symptoms of COVID-19 might have developed abruptly (i.e., emerged inside the building after passing the PPEO).
Our hospital runs a safety clinic aside from the outpatient clinic for adult and pediatric patients with respiratory symptoms unrelated to COVID-19. That safety clinic uses a different entrance from the outpatient clinic and might explain the relatively low incidence of cases missed by the PPEO that were reported by pulmonology and pediatrics. However, respiratory disease patients still visited our otorhinolaryngology department. In addition, procedures that can generate aerosols (e.g., nasal endoscopy and gastroendoscopy) are often performed in the otorhinolaryngology and gastroenterology departments, which might have raised awareness of the HCWs in those departments about patients with COVID-19 symptoms and led to their high frequency of reporting.
Missed cases in the PPEO were more likely to occur among first-time visitors than returning visitors to the hospital; this may be because first-time visitors are unfamiliar with the hospital’s systems, such as answering questionnaires at the kiosk. Additionally, there have been reports that people tend to conceal COVID-19 symptoms so that they do not have to undergo COVID-19 testing or because they are afraid of the hospital refusing treatment.15 This may be more obvious in those who have not visited the hospital previously.
Among the 449 cases missed by the PPEO, only two had a positive COVID-19 PCR test, and they were both gastroenterology patients. The first patient confirmed to have COVID-19 was reported on December 4, 2020, which was while Korea was experiencing exponential growth of COVID-19 cases. The first patient was a 78-year-old woman who visited gastroenterology due to constipation and reported no epidemiological history or symptoms indicative of COVID-19 in the PPEO. She visited the hospital during afternoon office hours, and she was a returning visitor. Her fever was not identified by the non-contact infrared thermometer camera in the PPEO, but at the gastroenterology department, her temperature according to the handheld contact ear thermometer was 39°C. The second case occurred on April 2, 2021, which was also a period in which Korea had a sharp increase in COVID-19 cases. That patient was a 68-year-old woman who visited gastroenterology due to abdominal discomfort and reported no epidemiological history or symptoms indicative of COVID-19 in the PPEO. She visited the hospital during afternoon office hours, and she was a first-time visitor to the hospital. Her fever was not identified by the non-contact infrared thermometer camera in the PPEO, but at the gastroenterology department, it was 40°C as measured by the handheld contact ear thermometer.
Although respiratory symptoms predominate in the clinical manifestations of COVID-19, gastrointestinal symptoms have been observed alone or with respiratory symptoms. Among gastrointestinal symptoms, vomiting, diarrhea, and abdominal pain/discomfort are prevalent, and constipation is less prevalent.1617 Older people and immunocompromised patients are particularly likely to present with atypical symptoms, including gastrointestinal symptoms.12 In this study, the two COVID-19 patients were both older than 65, and fever was not detected in the PPEO but was found in the second-level prescreening at the department. They were both gastroenterology patients, which was a department that frequently reported cases missed by the PPEO, had no respiratory symptoms. One patient was a first-time visitor to the hospital, and the other had visited previously. If these patients were not identified through second-level prescreening, whether they could lead to nosocomial infection or not is uncertain. However, similar cases are possible and could occur in other healthcare facilities. These two COVID-19 positive cases suggest that gastroenterology is one of the departments that may significantly benefit from adopting a two-level prescreening process.
This study has certain limitations. First, it was conducted at a single institution, so its findings might not be generalizable to other healthcare facilities. Second, cases might have been missed by both the PPEO and second-level departmental prescreening. Most of the departments in the outpatient clinic were overcrowded, and nurses might have not have reevaluated all patients and guardians for the presence of COVID-19 symptoms; they usually focused on the patients. Among the 449 patients identified in the second-level screening, only one was accompanying guardian. Third, this study has all the limitations associated with any retrospective design. In addition, some date were not collected, particularly data on patients or guardians who were identified as potential COVID-19 patients by the PPEO and sent to the OSC. Those patients were prevented from entering the hospital building to prevent nosocomial infections. Therefore, their data were not collected by the infection control unit. Fourth, the criterion for the emergency process was changed from 37.5°C to 38.0°C and then back to 37.5°C. We found that 2.30 cases were reported per day when the criterion was 37.5°C, whereas 0.79 cases were reported per day when the criterion was 38.0°C. The criterion might therefore have influenced the number of cases. The emergency process was implemented to prevent nosocomial infections in the outpatient clinic, and varied according to the number of newly confirmed cases in Korea. The lack of consistent application of this criterion is a limitation of the retrospective nature of the study.
Despite those limitations, to the best of our knowledge, this was the first study to analyze data about cases missed by the PPEO. Our results indicate that effort is needed to accurately identify individuals with a fever in the PPEO. Higher attention should be given to first-time visitors. Additionally, it appears that the two-level prescreening process should be continued in otorhinolaryngology and gastroenterology, which reported the most and second-most cases missed by PPEO, respectively, including two patients who tested positive for COVID-19.
During the study period, our outpatient clinic had 641,039 visits, and our second-level prescreening process at the departments identified 449 cases that were missed by the PPEO. Among those 449 cases, two patients tested positive for COVID-19. There might thus be controversy about whether our two-level prescreening process is effective. We implemented the two-level prescreening and emergency code because we had nosocomial COVID-19 infections in late February 2020. To prevent in-hospital transmission, the hospital was closed for 17 days, and COVID-19 PCR was performed for all inpatients and employees. That was the first time a university hospital was closed because of nosocomial COVID-19 infections.18
Whether a hospital should implement a two-level prescreening process in all departments, a few departments, or not at all will depend on factors such as its size, patient characteristics (i.e., age, comorbidities, and whether immunocompromised or not), and executive's decision. Although mass vaccination has begun in many countries, COVID-19 outbreaks continue in both communities and healthcare facilities.19 The delta variant is very transmissible, and the emergence of new variants and breakthrough infections is being reported continually.202122 Thus, prescreening in outpatient clinics cannot be stopped during the ongoing COVID-19 pandemic. Our experience and findings can serve as a reference for other healthcare facilities making decisions about their prescreening processes in outpatient clinics during the ongoing COVID-19 pandemic.
 XML Download
XML Download