

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Recent advances in stent technology, anti-thrombotic agents, and anti-atherosclerotic agents have contributed to the decrease in ischemic events after percutaneous coronary intervention (PCI), but the risk of bleeding from antiplatelet agents is still high. Bleeding complications are strongly associated with poor clinical outcomes. Therefore, it is imperative to assess and predict the future bleeding risk in patients who undergo PCI and select the optimal strategy for antiplatelet therapy. Based on literature review and clinical consensus, the Academic Research Consortium for High Bleeding Risk (ARC-HBR) group recently defined HBR as a Bleeding Academic Research Consortium (BARC) 3 or 5 bleeding risk of at least 4% at 1 year or an intracranial hemorrhage (ICH) risk of at least 1% at 1 year in patients undergoing PCI.1
Many studies have reported that ticagrelor increased the bleeding risk without reducing ischemic events in East Asian patients with acute myocardial infarction (AMI).23456 However, whether there is a difference in the bleeding risk with ticagrelor depending on HBR in East Asian patients remains unclear.
Therefore, our study aimed to determine whether there is a difference in the efficacy and safety of ticagrelor in Korean AMI patients, with or without HBR.
METHODS
Study population and definition
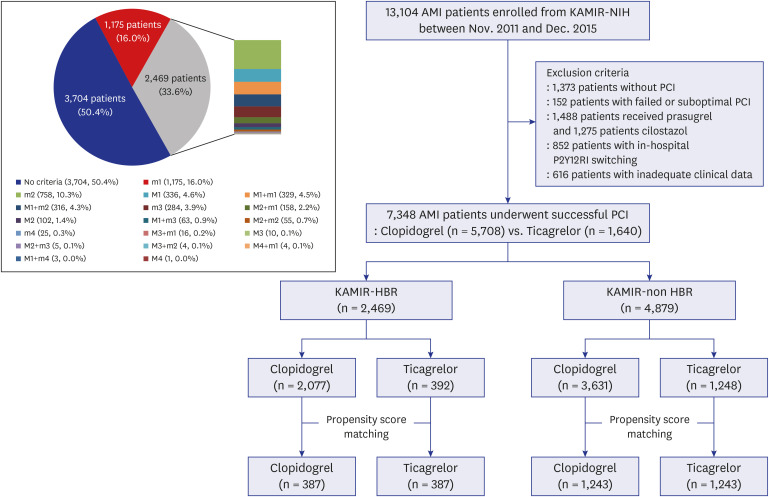
We selected all patients with AMI undergoing successful PCI from the Korea Acute Myocardial Infarction Registry-National Institute of Health (KAMIR-NIH), which is a prospective, multi-center, web-based observational cohort study from 20 centers in South Korea.7 We excluded patients without PCI, those with failed or suboptimal PCI, those who received prasugrel or cilostazol, those with in-hospital P2Y12 receptor inhibitor (RI) switching, and those with inadequate clinical data. Then, we identified a major or minor criterion at the time of PCI, corresponding to the criteria of HBR defined by the ARC-HBR group. Some criteria of ARC-HBR that could not be identified in KAMIR-NIH were inevitably excluded. The estimated glomerular filtration rate (eGFR) was calculated using the Cockcroft-Gault formula for all patients. Patients who had already taken oral anticoagulants before admission or who had atrial fibrillation at admission were considered to have anticipated the use of oral anticoagulants. The patient was considered to be at “KAMIR-HBR” if at least 1 major criterion or 2 minor criteria were met and was considered to be at “KAMIR-non HBR” if no major criteria and 0 or 1 minor criterion were met. To assess the risk of adverse clinical events based on the number of HBR criteria, the KAMIR-HBR scores were calculated by adding two points for any major criterion and one point for any minor criterion for convenience. Standardized definitions of all variables were determined by the steering committee board of the KAMIR-NIH. In other words, we divided the enrolled patients into the KAMIR-HBR and the KAMIR-non HBR groups, and each group was subdivided into clopidogrel and ticagrelor treatment regimens and subjected to comparison (Fig. 1).
Fig. 1
Flow chart of study and a bar of pie chart showing the combination of ARC-HBR major and minor criteria in all patients.
ARC = Academic Research Consortium, HBR = high bleeding risk, AMI = acute myocardial infarction, KAMIR-NIH = Korea Acute Myocardial Infarction Registry-National Institute of Health, PCI = percutaneous coronary intervention, RI = receptor inhibitor, KAMIR = Korea Acute Myocardial Infarction Registry, m = minor criterion for ARC-HBR, M = major criterion for ARC-HBR.
Intervention and medications
The choice of antiplatelet agents (clopidogrel or ticagrelor), anti-thrombotic therapy, the timing of invasive strategies (primary or early or delayed), vascular access site, pre- or post-dilatation, type of stents, and use of periprocedural glycoprotein IIb/IIIa inhibitors were freely decided by a physician at each center based on the clinical status of patients with AMI. Anti-platelet agents were administered to all patients prior to PCI, with 300 mg loading dose (LD) of aspirin and 300 or 600 mg LD of clopidogrel, or 180 mg LD of ticagrelor. PCI was simultaneously performed in a standard and conventional manner. After the intervention, all patients were required to take one of the following three P2Y12RIs along with aspirin 100 mg for at least 1 year, which included a maintenance dose (MD) of clopidogrel 75 mg once a day, or 90 mg ticagrelor twice a day. It was customary to continue dual antiplatelet therapy (DAPT) for at least 12 months in our registry, if possible. Other medical treatments based on standard therapies for AMI patients were also used without restriction, considering the patient's clinical condition.
Study endpoints
The primary efficacy endpoints were major adverse cardiovascular events (MACEs), defined as a composite of cardiac death, non-fatal MI, or stroke during hospitalization. The primary safety endpoint was the incidence of the thrombolysis in myocardial infarction (TIMI) major bleeding during hospitalization. The secondary endpoints were net adverse cardiovascular events (NACEs), defined as a composite of cardiac death, non-fatal MI, stroke, or TIMI major bleeding during hospitalization, and MACEs and a composite of MACEs or repeat revascularization at the 6-month follow-up, and its individual components including all-cause death, definite stent thrombosis, or TIMI major or minor bleeding during hospitalization. Repeat revascularization was defined as unplanned repeat PCI or bypass surgery that occurred after discharge from the index hospitalization.
Statistical analysis
Categorical variables were expressed as frequencies and percentages, and continuous variables as mean ± standard deviation (SD). Categorical variables were analyzed using the χ2 test or Fisher's exact test, as appropriate, and continuous variables were assessed by the Student's t-test.
To minimize the effect of selection bias between clopidogrel and ticagrelor, first, a multivariate logistic regression model with an “enter” method was performed using the independent variables for all individual outcome components. Only variables with a P value < 0.20 in the univariate analysis were included in the multivariate model. It was also used to identify independent predictors of in-hospital TIMI major bleeding in both the KAMIR-HBR and the KAMIR-non HBR groups. Second, the propensity score (PS) was estimated using a multivariable logistic regression model, wherein ticagrelor therapy was checked in reverse on all baseline clinical, angiographic, and procedural characteristics and in-hospital medications. Thereafter, the patients treated with clopidogrel were one-to-one matched with those treated with ticagrelor as per the PS using the nearest neighbor matching within a caliper width of 0.2 of the SD of the logit of the PS. The balance between the two groups after PS matching was assessed by calculating the standardized mean difference (SMD). The SMD was calculated by dividing the difference in means or proportions by standard error and was considered an imbalance if the absolute value was greater than 0.10.
Cumulative clinical events of 6-month and landmark analysis from 30 days were analyzed and compared between clopidogrel and ticagrelor by a Kaplan-Meier survival curve using a log-rank test. Hazard ratios and 95% confidence interval (CI) for 6-month clinical outcomes were calculated using Cox proportional hazard regression models with all variables in the univariate analysis with a P value of < 0.20.
The odds ratio (OR) for in-hospital TIMI major bleeding with the associated 95% CI for clopidogrel versus ticagrelor at each level of the exploratory subgroup and overall patients were presented in the forest plots, together with the incidence rates per treatment group within the subgroup and the treatment-by-subgroup interaction P values. A P value for the interaction of less than 0.1 indicated a statistically significant subgroup effect.
All statistical tests were two-tailed, and a P value < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS (Statistical Package for Social Science, SPSS Inc., Chicago, IL, USA) for Windows, version 27.0.
Ethics statement
The study protocols were approved by the ethics committee at each participating center and followed the principles of the Declaration of Helsinki, revised in 2013. Written informed consent was obtained from all patients for participation in the KAMIR-NIH registry. The approval number was CNUH-2011-172 of Chonnam National University Hospital. Trained study coordinators at each participating institution collected all the data using a formalized form.
RESULTS
Baseline characteristics of all patients
Between November 2011 and December 2015, 7,348 patients with AMI who underwent successful PCI were analyzed from the KAMIR-NIH registry. As per the HBR definition of the ARC-HBR, 2,469 patients (33.6%) were classified into the KAMIR-HBR group and 4,879 patients (66.4%) were classified into the KAMIR-non HBR group. The KAMIR-HBR group included 758 patients (10.3%) with 2 minor criteria, 336 patients (4.6%) with 1 major criterion, and 329 patients (4.5%) with 1 major and 1 minor criterion. The KAMIR-non HBR group comprised 1,175 patients (16.0%) with 1 minor criterion and 3,704 patients (50.4%) without any major or minor HBR criterion (Fig. 1). Hemoglobin < 11 g/dL (654 patients; 8.9%) was the most common major criterion and moderate chronic kidney disease (1,985 patients; 27.0%) was the most common minor criterion in all patients. Clopidogrel and ticagrelor were administered to 2,077 (84.1%) and 392 (15.9%) patients in the KAMIR-HBR group and 3,631 (74.4%) and 1,248 (25.6%) patients in the KAMIR-non HBR group, respectively (Table 1 and Supplementary Table 1).
Table 1
Major baseline clinical characteristics between clopidogrel and ticagrelor in all patients
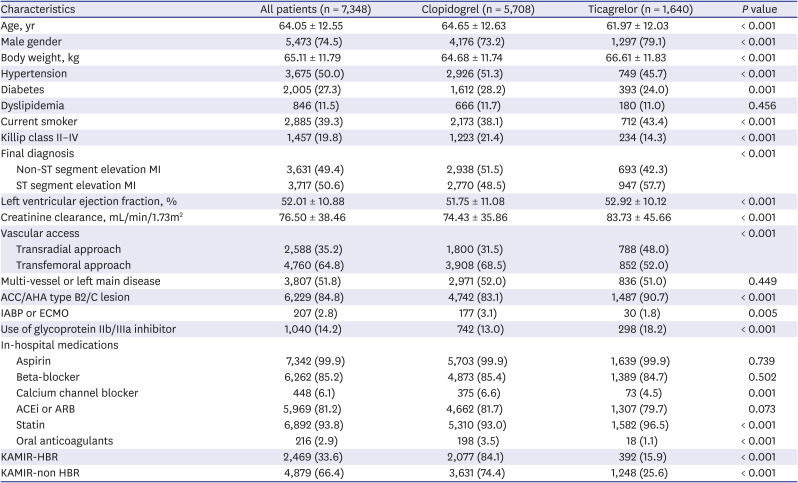
Values are shown as mean ± standard deviation or number (%).
MI = myocardial infarction, ACC = American College of Cardiology, AHA = American Heart Association, IABP = intra-aortic balloon pump, ECMO = extracorporeal membrane oxygenation, ACEi = angiotensin converting enzyme inhibitor, ARB = angiotensin II receptor blocker, KAMIR = Korea Acute Myocardial Infarction Registry, HBR = high bleeding risk.
KAMIR-HBR vs. KAMIR-non HBR in all patients
The KAMIR-HBR group had significantly worse baseline clinical, angiographic, and procedural characteristics and lower prescription rates of in-hospital medications than the KAMIR-non HBR group (Table 2 and Supplementary Table 2). Overall, 1,375 (55.7%) and 1,094 (44.3%) patients from the KAMIR-HBR group had KAMIR-HBR scores ≥ 3 points and 2 points, respectively, and 1,175 (24.1%) and 3,704 (75.9%) patients from the KAMIR-non HBR group had KAMIR-HBR scores of 1 and 0 points, respectively (Supplementary Table 1).
Table 2
Major baseline clinical characteristics between clopidogrel and ticagrelor in both the KAMIR-HRB and the KAMIR-non HBR groups
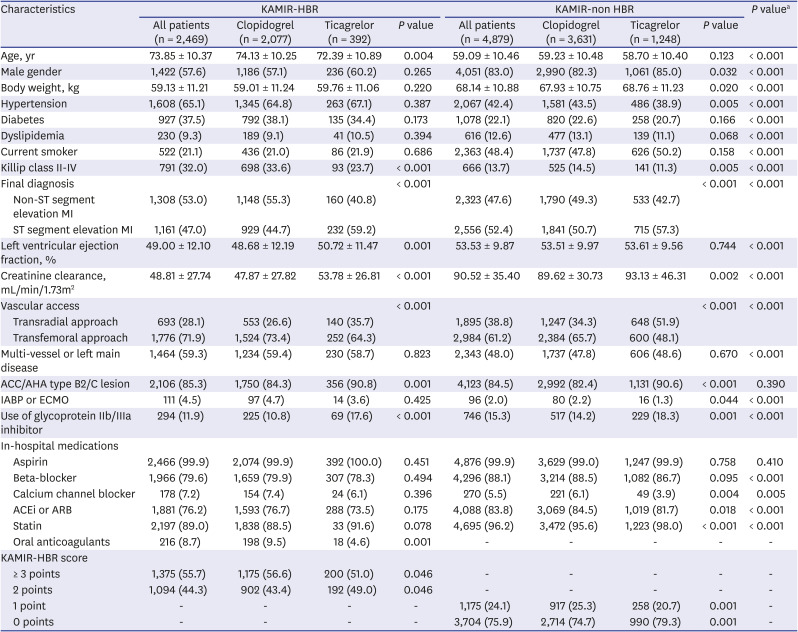
Values are shown as mean ± standard deviation or number (%).
KAMIR = Korea Acute Myocardial Infarction Registry, HBR = high bleeding risk, MI = myocardial infarction, ACC = American College of Cardiology, AHA = American Heart Association, IABP = intra-aortic balloon pump, ECMO = extracorporeal membrane oxygenation, ACEi = angiotensin converting enzyme inhibitor, ARB = angiotensin II receptor blocker.
aComparison of the difference between the KAMIR-HBR and the KAMIR-non HBR groups.
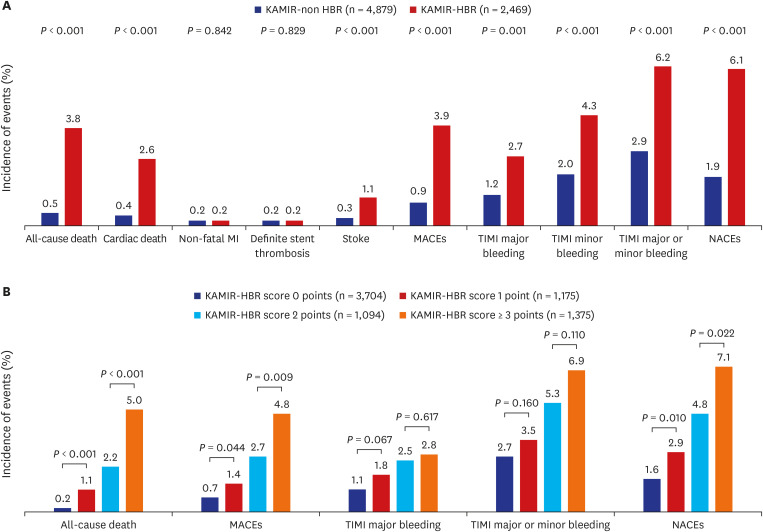
In the unadjusted clinical outcomes during hospitalization, the KAMIR-HBR group had significantly higher incidences of MACEs and TIMI major bleeding than the KAMIR-non HBR group (Fig. 2A). Ischemic and bleeding events tended to gradually increase with an increase in the KAMIR-HBR score. Patients with a KAMIR-HBR score ≥ 3 points in the KAMIR-HBR group and 1 point in the KAMIR-non HBR group had significantly higher incidences of all-cause death, MACEs, and NACEs than those with a score of 2 points in the KAMIR-HBR group and 0 points in the KAMIR-non HBR group (Fig. 2B).
Fig. 2
In-hospital clinical outcomes (A) between the KAMIR-non HBR and the KAMIR-HBR groups, and (B) among 4 groups classified according to KAMIR-HBR scores.
KAMIR = Korea Acute Myocardial Infarction Registry, HBR = high bleeding risk, MI = myocardial infarction, MACEs = major adverse cardiovascular events, TIMI = thrombolysis in myocardial infarction, NACEs = net adverse clinical events.
Clopidogrel vs. ticagrelor in all patients, the KAMIR-HBR, and the KAMIR-non HBR groups
Before PS matching, the patients treated with clopidogrel tended to be older and female, and have more cardiovascular risk factors, worse Killip class, and lower creatinine clearance than those treated with ticagrelor in each of the three groups. They were also more likely to be treated using the transfemoral approach and less likely to use a glycoprotein IIb/IIIa inhibitor (Tables 1, 2 and Supplementary Tables 1, 2).
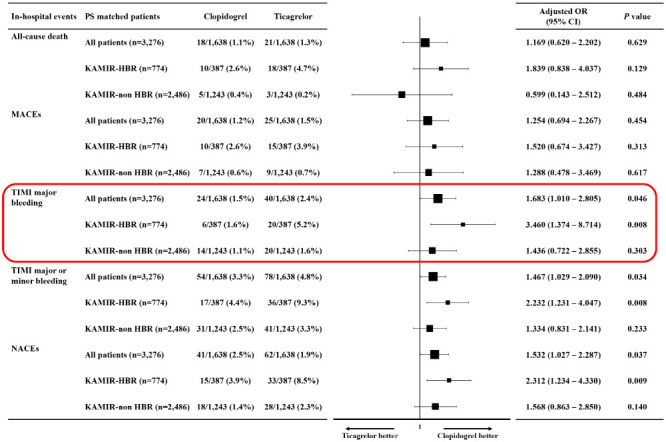
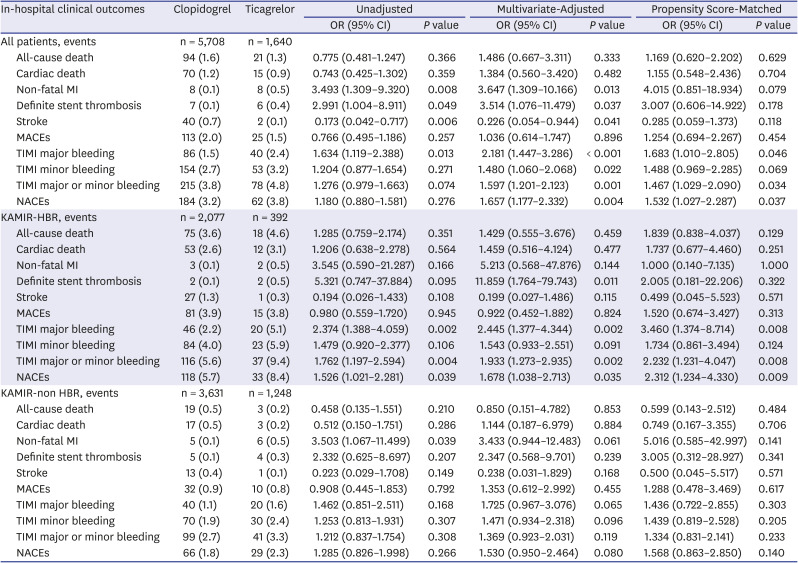
After PS matching in each of the three groups (Supplementary Tables 3 and 4), there was no difference in the incidence of MACEs between patients taking clopidogrel and those taking ticagrelor during hospitalization. Patients on ticagrelor had a higher incidence of TIMI major bleeding and NACEs than clopidogrel regardless of bleeding risk (OR, 1.683; 95% CI, 1.010–2.805; P = 0.046 and OR, 1.532; 95% CI, 1.027–2.287; P = 0.037) in all patients. In addition, higher incidences of TIMI major bleeding and NACEs in patients taking ticagrelor compared to those taking clopidogrel were observed in the KAMIR-HBR group (OR, 3.460; 95% CI, 1.374–8.714; P = 0.008 and OR, 2.312; 95% CI, 1.234–4.330; P = 0.009). However, there were no significant differences in TIMI major bleeding and NACEs between patients on clopidogrel and those on ticagrelor in the KAMIR-non HBR group (OR, 1.436; 95% CI, 0.722–2.855; P = 0.303 and OR, 1.568; 95% CI, 0.863–2.850; P = 0.140). These results were consistent with the multivariate logistic regression analysis of all the confounding variables (Table 3).
Table 3
In-hospital clinical outcomes between clopidogrel and ticagrelor in both the KAMIR-HBR and the KAMIR-non HBR groups
The independent predictors of in-hospital TIMI major bleeding were TFI vs. TRI, glycoprotein IIb/IIIa inhibitor, and use of IABP or ECMO in both the KAMIR-non HBR and the KAMIR-HBR groups. However, ticagrelor was an independent predictor of in-hospital TIMI major bleeding in the KAMIR-HBR group (OR, 2.445; 95% CI, 1.377–4.344; P = 0.002) but not in the KAMIR-non HBR group (OR, 1.725; 95% CI, 0.967–3.076; P = 0.065) (Table 4).
Table 4
The independent predictors of in-hospital TIMI major bleeding in both the KAMIR-HRB and the KAMIR-non HBR groups
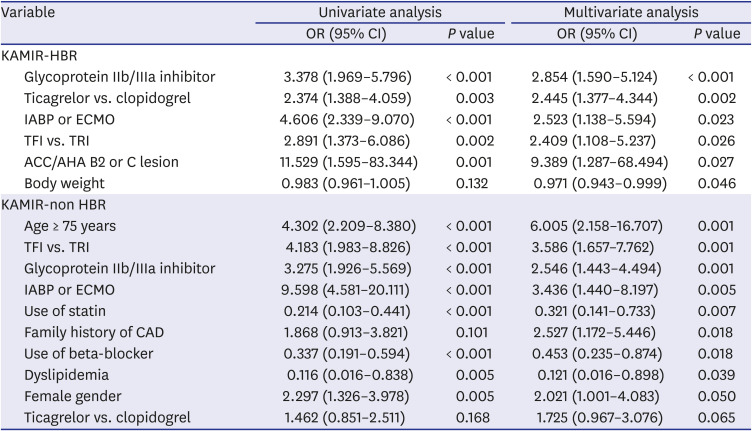
TIMI = thrombolysis in myocardial infarction, KAMIR = Korea Acute Myocardial Infarction Registry, HBR = high bleeding risk, OR = odds ratio, CI = confidence interval, IABP = intra-aortic balloon pump, ECMO = extracorporeal membrane oxygenation, TFI = trans-femoral intervention, TRI = trans-radial intervention, ACC = American College of Cardiology, AHA = American Heart Association, CAD = coronary artery disease.
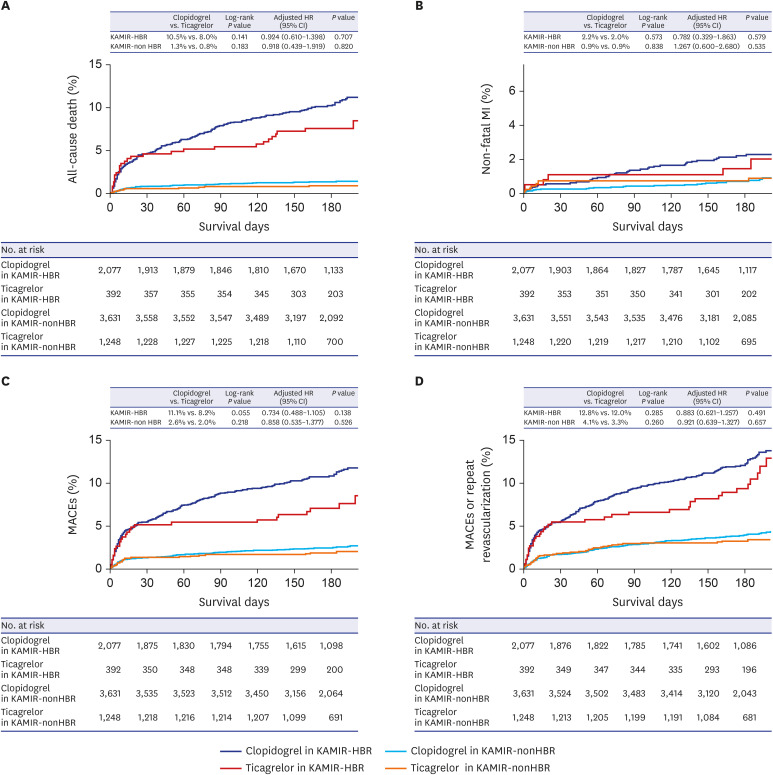
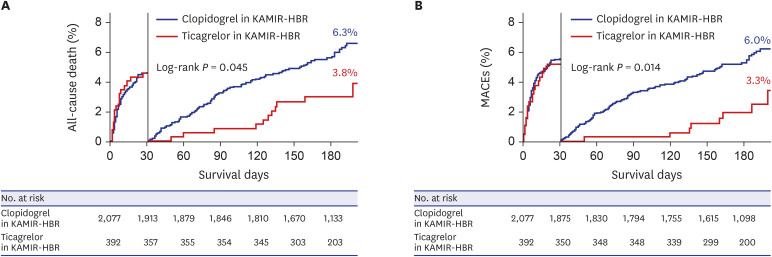
In the Kaplan-Meier survival curve at the 6-month follow-up, the cumulative risk of MACEs tended to be higher in patients on clopidogrel than in those on ticagrelor in the KAMIR-HBR group, however, the significance was diminished in the multivariable Cox proportional hazard regression model (Fig. 3). However, landmark analysis from 30 days in the KAMIR-HBR groups showed that there were significant differences in all-cause death and MACEs between patients on clopidogrel and those on ticagrelor (Fig. 4).
Fig. 3
Kaplan-Meier events-free survival curve between clopidogrel and ticagrelor in both the KAMIR-HBR and the KAMIR-non HBR groups. (A) All-cause death, (B) non-fatal MI, (C) MACEs, and (D) MACEs or repeat revascularization.
KAMIR = Korea Acute Myocardial Infarction Registry, HBR = high bleeding risk, HR = hazard ratio, CI = confidence interval, MI = myocardial infarction, MACEs = major adverse cardiovascular events.
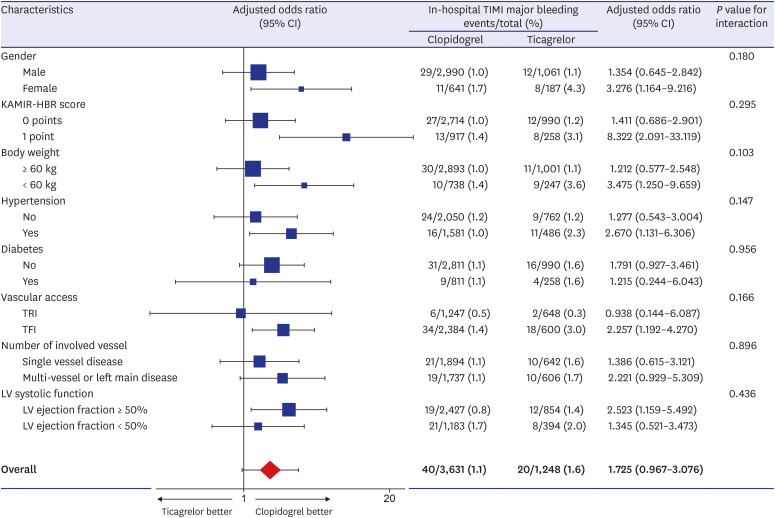
Subgroup analyses in the KAMIR-non HBR group
An exploratory subgroup analysis of the KAMIR-non HBR group illustrated the OR for the incidence of in-hospital TIMI major bleeding between patients on clopidogrel and those on ticagrelor in subgroups as well as overall. The disfavoring treatment effect of ticagrelor as compared to that of clopidogrel was consistent across all exploratory subgroups without statistically significant treatment-by-subgroup interactions (Fig. 5).
Fig. 5
Forest plot of exploratory subgroup analyses between clopidogrel and ticagrelor for in-hospital TIMI major bleeding in patients without HBR.
TIMI = thrombolysis in myocardial infarction, HBR = high bleeding risk, CI = confidence interval, KAMIR = Korea Acute Myocardial Infarction Registry, TRI = trans-radial intervention, TFI = trans-femoral intervention, LV = left ventricular.
DISCUSSION
This study was conducted to assess the efficacy and safety of ticagrelor in Korean patients with AMI without HBR. It is well known that ticagrelor is associated with a high risk of bleeding without reducing ischemic events in East Asian patients who underwent PCI. The main difference of our study from previous studies is that we classified all patients according to the ARC-HBR definition and analyzed each group. The major findings of our study confirmed that ticagrelor use was still associated with a higher incidence of in-hospital bleeding than clopidogrel use in all patients and the KAMIR-HBR group. However, there was no significant difference in the incidence of in-hospital bleeding events between patients on clopidogrel and those on ticagrelor in the KAMIR-non HBR group. The bleeding risk of ticagrelor was attenuated in Korean patients with AMI without HBR.
The definition of ARC-HBR has been well validated for the prediction of bleeding risks in several registries and randomized studies in both East Asian and Western populations.8910 In our study, in-hospital TIMI major bleeding was 4.3% in the KAMIR-HBR group and 2.0% in the KAMIR-non HBR group. These results are quite high compared to other studies. They may be due to the specific type of patients enrolled in our study. Our sample included only East Asian patients with AMI who underwent PCI. These patients were well known for their high bleeding risks. Moreover, many patients had multiple ARC-HBR criteria.
The HBR definition for ARC-HBR groups must consider ethnicity and the presence of acute coronary syndrome (ACS). It tends to underestimate the bleeding risk of these groups, especially in East Asian patients with ACS. Nevertheless, using the definition of ARC-HBR in our study to classify the patients into HBR vs. non-HBR groups, it was possible to sufficiently identify and predict the future bleeding risk and apply it to Korean patients who underwent PCI.
Recently, ticagrelor has been reported to increase bleeding risks without reducing ischemic events in East Asian patients. East Asians have a higher risk of bleeding than Westerners because their responses to antiplatelet agents are different due to racial differences in intrinsic thrombogenicity.11 Our study shows that ticagrelor also had significantly higher risks of major bleeding and NACEs than clopidogrel in all Korean patients with AMI. Therefore, it is imperative to determine ways to apply a potent P2Y12RI strategy without increasing the bleeding risk of East Asian patients.
Our study is the first to show that there was no significant difference in the incidence of in-hospital bleeding complications between ticagrelor and clopidogrel use in East Asian patients without HBR. This suggests that the appropriate selection of patients for potent P2Y12RIs is actually one of the important factors in reducing the bleeding risk in clinical practice. Ticagrelor may be safely used in Korean patients with AMI without HBR. Nevertheless, East Asian patients without HBR would have a higher risk of bleeding than Western patients without HBR because of ethnic differences. Therefore, when using potent P2Y12RIs in East Asian patients, even in patients without HBR, careful attention should be still paid to the occurrence of bleeding events.
Our study also showed that patients with HBR had significantly higher ischemic and bleeding risks than those without HBR, and that patients with multiple HBR criteria were associated with more adverse clinical events. Therefore, a patient with HBR by the ARC-HBR definition tends to have a high ischemic risk as well as a high bleeding risk and the risk of bleeding and ischemia tends to increase gradually as the number of HBR criteria increases.
Although ticagrelor is well known to reduce mortality and ischemic events over clopidogrel in ACS patients,1213 the superiority of ticagrelor over clopidogrel remains controversial in some recent studies.4614 Our study also showed that the 6-month cumulative incidences of ischemic events did not differ between patients on ticagrelor and those on clopidogrel, regardless of HBR. This could be caused by differences in study design or study population, use of second-generation drug eluting stents or high-potency statin, or drug compliance. Therefore, we believe that a large-scale randomized controlled trial is necessary to confirm the efficacy of ticagrelor in Korean AMI patients.
However, additional landmark analysis from 30 days in patients with HBR showed significant differences in all-cause death and MACE between the two groups. Nevertheless, we have to be careful in interpreting this result. It must also be demonstrated by a large randomized controlled trial due to several issues, such as significant differences in baseline characteristics between two groups and switching, discontinuation, or compliance of ticagrelor during the follow-up period, and must also be checked for bleeding events during the follow-up period. In any case, ticagrelor would be very effective in reducing ischemic events, even in AMI patients with HBR, if ischemic risk was higher than bleeding risk. Recently, ticagrelor has been reported to have pleiotropic effects such as an improvement of left ventricular remodeling,15 and reduction of neointimal formation, endothelial dysfunction, and peri-strut inflammation1617 in addition to the antiplatelet effect. For that reason, we believe that the use of ticagrelor might be beneficial for AMI patients with a high risk of ischemia or a low risk of bleeding. Therefore, the choice of P2Y12RI should be carefully considered and appropriately determined depending on the characteristics of the patient and the clinical situation.
Patients with and without HBR have different risk factors, clinical outcomes, and predictors of in-hospital bleeding, therefore, we need to treat them differently and P2Y12RI strategies should be chosen differently. The use of potent P2Y12RIs in patients with HBR could increase the risk of bleeding rather than reducing the risk of ischemia. Accordingly, it seems more appropriate to carry out the de-escalation strategies of potent P2Y12RI to reduce the risk of bleeding when using a potent P2Y12RI in patients with HBR. To date, the de-escalation strategies of potent P2Y12RI have been studied and developed to safely use potent P2Y12RIs, such as reducing the maintenance dosage,1819 shortening the duration of DAPT,2021 administering monotherapy by omitting aspirin,22232425 and switching to clopidogrel after a potent P2Y12RI only for a short period initially.2627 Conversely, our findings suggest that the de-escalation strategies of potent P2Y12RI are not necessarily required in patients without HBR. Therefore, above all, assessing the status of HBR in patients underwent PCI may enable a more personalized antiplatelet strategy, such as the choice of optimal antiplatelet agent, optimal de-escalation strategy, or optimal duration of DAPT to reduce ischemic risk without increasing bleeding risk in the future.
Our study had several limitations. First, as this was a post-hoc analysis of an observational registry study, we were unable to identify any HBR criteria that had not been previously investigated, such as chronic bleeding diathesis, liver cirrhosis with portal hypertension, active malignancy, nondeferrable major surgery on DAPT, recent major surgery or major trauma within 30 days before PCI, and long-term use of nonsteroidal anti-inflammatory drugs or steroids. Therefore, HBR could be underestimated and non-HBR could be overestimated in our study. However, a recent study has shown that the prevalence of the criteria that we could not identify was very low,28 therefore, our study does not seem to misrepresent the current clinical situation of Korean patients with AMI. Second, our study was based on a non-randomized, prospective, and observational registry, therefore, selection bias could not be completely avoided while comparing clopidogrel to ticagrelor, although it was partially compensated by multivariate logistic regression and PS-matched analysis. Third, our registry, in principle, recommended continuing DAPT for at least 12 months, but it was not possible to force DAPT to continue, and to determine the frequency of switching or discontinuation, or compliance of ticagrelor during follow-up treatment after discharge because of the major limitation of the observational registry. Therefore, it was unclear how directly ticagrelor affected the occurrence of clinical events during the follow-up period. Fourth, we could not exactly identify and evaluate the bleeding events during the follow-up due to the limitations of registry data. Fifth, our registry was able to evaluate only the bleeding criteria defined by the TIMI but not by the BARC criteria.
In conclusion, our study demonstrated that ticagrelor use is still associated with a higher incidence of in-hospital bleeding events compared to clopidogrel use in all patients and in the KAMIR-HBR group. However, there was no significant difference in the incidence of in-hospital bleeding events between clopidogrel and ticagrelor in the KAMIR-non HBR group. Therefore, the bleeding risk of ticagrelor was attenuated in Korean patients with AMI without HBR. These findings suggest that appropriate patient selection could reduce in-hospital bleeding complications of ticagrelor in Korean patients with AMI who underwent successful PCI. Further large-scale, randomized controlled trials are warranted to determine the optimal antiplatelet therapy strategy according to HBR in East Asian patients with AMI who underwent PCI.
 XML Download
XML Download