

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The American College of Cardiology (ACC), American Heart Association (AHA), and European Society of Cardiology (ESC) have developed evidence-based guidelines for the treatment of heart failure (HF) based on the best available evidence for improved clinical outcomes. Numerous studies have documented the evidence-based benefits of angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor II blockers (ARBs), β-blockers, mineralocorticoid receptor antagonists (MRAs), angiotensin receptor neprilysin inhibitors, and ivabradine on HF outcomes. Although such benefits include reduced ejection fraction (HFrEF) and normal sinus rhythm, outcomes for preserved ejection fraction in patients with HF (HFpEF) have not improved over the last few decades, and current international guidelines acknowledge the lack of evidence-based strategies for treating patients with HFpEF.1234
Atrial fibrillation (AF) is common in patients with HF because they share common risk factors and are closely associated pathophysiologically.5 Even in patients with HFrEF and AF, there are limited data supporting the benefits of individual HF therapy. However, better adherence to guidelines has been associated with prognosis, and accumulation of individual HF therapy has been shown to improve prognoses in patients with HFrEF and AF.6 Nonetheless, there is no convincing evidence that disease-modifying HFrEF therapies can reduce morbidity or mortality associated with HFpEF. Despite this, there is some evidence that β-blockers, MRAs, and ARBs can reduce hospitalization, and several studies have reported that patients treated using these therapies exhibit a trend towards a reduction in combined cardiovascular mortality and hospitalization.789 There is an unmet need for an evaluation of the comprehensive effects of disease-modifying HFrEF therapies in patients with HFpEF.10 Therefore, this study aimed to evaluate the relationship between the degree of adherence to guidelines for HFrEF and relevant 60-day and 1-year clinical outcomes in patients with HFpEF with or without AF.
METHODS
Study population
The Korean Acute Heart Failure (KorAHF) registry includes the data of 5,625 hospitalized patients with acute HF treated at 10 tertiary hospitals in Republic of Korea between March 2011 and February 2014.11 This registry included hospitalized patients who had signs or symptoms of HF and at least one objective sign of lung congestion or objective findings of left ventricular systolic dysfunction or structural heart disease. The only exclusion criterion of this registry was the withdrawal of consent.11 For this study, we only selected patients with HFpEF with 1 year of follow-up data. HFpEF was defined as a left ventricular ejection fraction ≥ 50%. AF was defined based on electrocardiographic confirmation of AF at admission or history of AF.
Assessment of guideline adherence
To assess adherence to the guidelines, we adopted and modified the QUality of Adherence to guideline recommendations for LIFe-saving treatment in heart failure surveY (QUALIFY) international survey.612 A global guideline adherence score, QUALIFY, was constructed based on physicians' adherence to guidelines for prescriptions of the following classes of medications: ACC/AHA/ESC guidelines recommended ACEIs, ARBs, β-blockers, MRAs, and ivabradine, for patients with HFrEF with normal sinus rhythm, unless contraindicated or not tolerated.461213 However, ivabradine was not included from this study because it was not available in South Korea during the study period. Additionally, anticoagulation therapy was included as a guideline-recommended therapy since anticoagulation is an established therapeutic strategy to reduce the risk of stroke in AF patients.1415 In addition to reducing the risk of stroke, anticoagulants markedly reduce the risk of death.16 The adherence was defined as the actual prescription of guideline recommended therapy that should have theoretically been prescribed for each of ACEIs or ARBs, β-blockers, MRAs, and an oral anticoagulant (if indicated). Only guideline-recommended β-blockers (including bisoprolol, carvedilol, sustained-release metoprolol succinate, and nebivolol) were recognized as adherence to guidelines. The non-adherence was defined as non-prescription of therapy in the absence of specified contraindications. Non-prescription of the recommended therapies because of specific contraindications or intolerance was also scored for adherence to guidelines.12 Additionally, non-prescription of anticoagulation for a CHA2DS2-VASc score < 2 was defined as adherence to guidelines. The level of adherence was defined as good for use of more than half of the indicated medications and poor for use of ≤ 50% of the indicated medications.61217
Clinical outcomes
In this study, the outcomes were defined as all-cause mortality, rehospitalization due to aggravated HF, and a composite endpoint of mortality and HF rehospitalization at 60 day and 1 year. The attending physicians collected follow-up data. For the patients who were not directly followed by, the outcome data were ascertained via transtelephonic monitor or using the National Death Records database. All clinical events were monitored and verified by a Clinical Event Committee comprising independent experts on HF who did not participate in the patient enrollment part of this study.11
Statistical analyses
Data are presented as the mean ± standard deviation for continuous variables and as numbers and frequencies for categorical variables. For comparison between groups, χ2 test was used for categorical variables and the unpaired Student t-test was used for continuous variables. To address the systematic differences between the two groups, we used inverse probability of treatment weighting (IPTW) analyses to reduce imbalances in measured confounders.18 The propensity score was estimated using a logistic regression model with the following covariates: sex; type of HF (acute decompensated HF or de novo HF); New York Heart Association functional class; history of hypertension, diabetes, ischemic heart disease, chronic obstructive pulmonary disease, chronic kidney disease, or cardiovascular accident; etiology of HF; right bundle branch block; left bundle branch block and corrected QT time on electrocardiogram; systolic blood pressure; diastolic blood pressure; serum sodium level; hemoglobin level; creatinine level; and left ventricular ejection fraction. The estimated propensity scores were used to calculate the inverse probability of the level of adherence for each patient. Weighting by the inverse probability of treatment results in an artificial population in which baseline covariates are independent of treatment status. Post-weighting balance in covariates between treatment groups was evaluated using the standardized difference approach. The balance between the treatment groups was assessed using weighted standardized mean differences (SMDs). An SMD value ≤ 20% was considered acceptable. The association between the degree of guideline adherence and clinical outcomes was analyzed using weighted Kaplan-Meier curves and Cox proportional hazards regression with a robust variance estimator to calculate weighted hazard ratios (wHRs) (95% confidence intervals [CIs]). Cox proportional hazards regression models were adjusted for sex; age; history of hypertension, diabetes mellitus, ischemic heart disease, and chronic obstructive pulmonary disease; type of HF (de novo vs. acute decompensated HF); New York Heart Association functional class; systolic blood pressure; heart rate; creatinine level; and left ventricular ejection fraction. In all cases, a P value ≤ 0.05 was considered statistically significant. Statistical analyses were performed using SPSS Version 23.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
The study protocol was approved by the ethics committee at each hospital and the Wonju Christian Hospital, Wonju College of Medicine, Yonsei University (Wonju, Korea; Approval No. CR311003), and was conducted according to the principles of the Declaration of Helsinki. All patients provided written informed consent for participation in the registry.
RESULTS
Of the 5,625 patients in the KorAHF registry, 4,231 were excluded because of HFrEF, in-hospital death, need for transplantation, incomplete echocardiographic or electrocardiographic data, or incomplete data for discharge medication. Of the remaining 1,394 patients with HFpEF, 707 and 687 patients were diagnosed with and without AF, respectively.
Baseline characteristics of patients without AF
In the 687 patients without AF, the median age of the cohort was 74 (interquartile range [IQR]: 63–81) years, and 58.8% of these patients were women. Modified guideline adherence was good in 53.6% and poor in 46.4% of patients. In contrast to our expectation, patients with a poorer guideline adherence had favorable clinical characteristics (Table 1). Patients with poor guideline adherence had lower systolic blood pressure at admission, less prevalent comorbidities (hypertension, diabetes mellitus, and chronic kidney disease), different etiology of HF (less likely to have ischemic heart disease and more likely to have valvular heart disease), unique laboratory characteristics (higher levels of hemoglobin and lower levels of creatinine, B-type natriuretic peptide [BNP], and troponin), and favorable echocardiographic characteristics (smaller left ventricular diastolic and systolic volume and greater preserved ejection fraction). All baseline differences were balanced after IPTW except residual borderline differences in left ventricular end diastolic volume and serum creatinine. In the poor adherence group, the guideline adherence rates were 34.8%, 11.0%, and 14.7% for ACEIs or ARBs, β-blockers, and MRAs, respectively. The prescription rate of loop diuretics was also significantly lower in the poor adherence group than in the good adherence group (Supplementary Table 1).
Table 1
Baseline characteristics of patients without atrial fibrillation for the analysis of modified guideline adherence
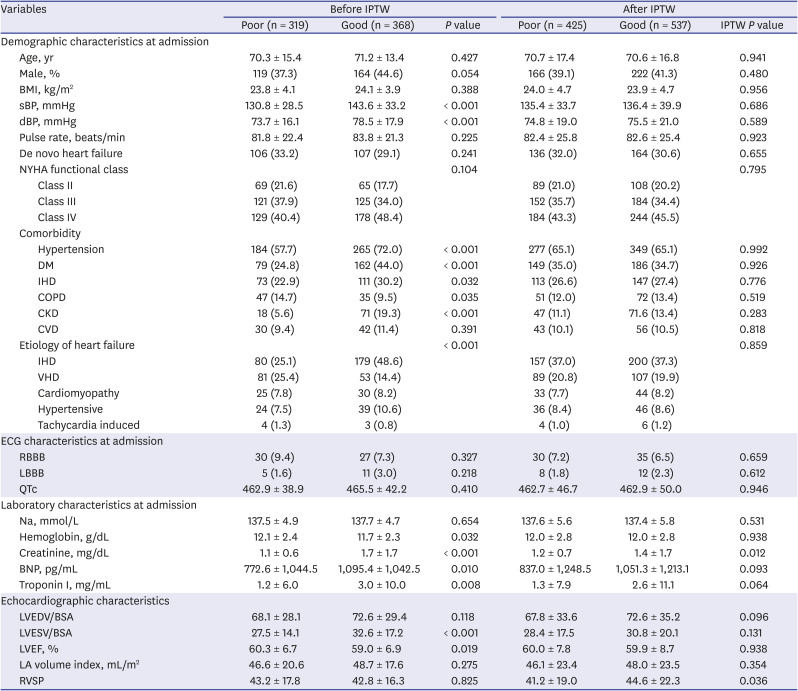
Values are presented as numbers (%) or means ± standard deviations, unless otherwise indicated.
IPTW = inverse probability of treatment weighting, BMI = body mass index, sBP = systolic blood pressure, dBP = diastolic blood pressure, NYHA = New York Heart Association, DM = diabetes mellitus, IHD = ischemic heart disease, COPD = chronic obstructive pulmonary disease, CKD = chronic kidney disease, CVD = cerebrovascular disease, VHD = valvular heart disease, ECG = electrocardiography, RBBB = right bundle branch block, LBBB = left bundle branch block, QTc = corrected QT interval, Na = serum sodium, BNP = B-type natriuretic peptide, LVEDV = left ventricular end-diastolic volume, BSA = body surface area, LVESV = left ventricular end-systolic volume, LVEF = left ventricular ejection fraction, LA = left atrium, RVSP = right ventricular systolic pressure.
Baseline characteristics of patients with AF
In the 707 patients with AF, the median age of the cohort was 76 (IQR: 69–82) years, and 62.0% of these patients were women. Modified guideline adherence was good in 33.2% and poor in 66.8% of patients. In contrast to patients without AF, the baseline clinical characteristics of patients with AF were similar according to the degree of adherence, except for the level of BNP, corrected QT interval, and bundle branch block on electrocardiogram (Table 2). All baseline differences were balanced after IPTW. In the poor adherence group, the guideline adherence rates were 42.4%, 25.0%, 32.0%, and 39.2% for ACEIs or ARBs, β-blockers, MRAs, and warfarin, respectively. The calculated equivalent doses of each medication did not significantly differ according to adherence. The prescription rate of loop diuretics was also significantly lower in the poor adherence group than in the other two groups; however, the prescription rate of other medications including amiodarone and digoxin did not significantly differ (Supplementary Table 2).
Table 2
Baseline characteristics of patients with atrial fibrillation for the analysis of modified guideline adherence
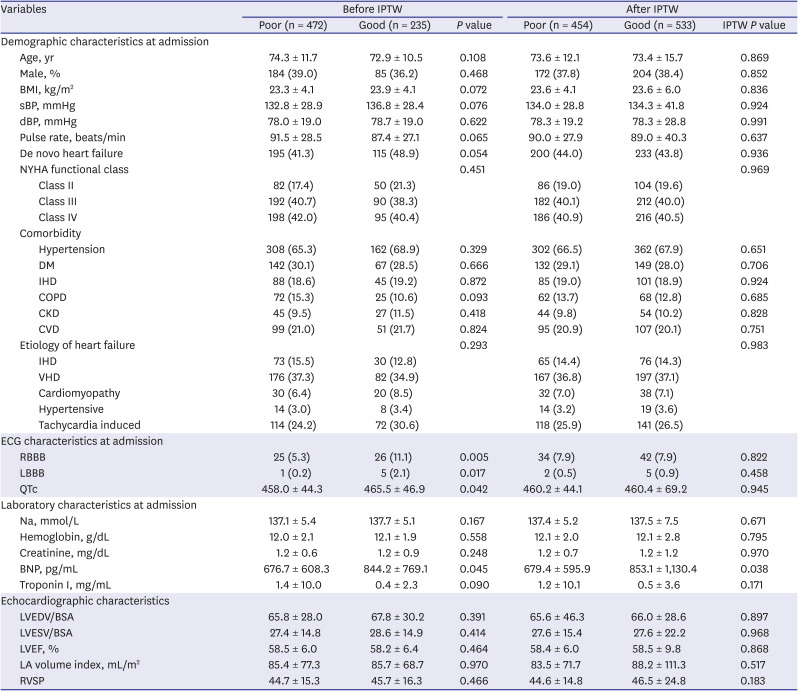
Values are presented as numbers (%) or means ± standard deviations, unless otherwise indicated.
IPTW = inverse probability of treatment weighting, BMI = body mass index, sBP = systolic blood pressure, dBP = diastolic blood pressure, NYHA = New York Heart Association, DM = diabetes mellitus, IHD = ischemic heart disease, COPD = chronic obstructive pulmonary disease, CKD = chronic kidney disease, CVD = cerebrovascular disease, VHD = valvular heart disease, ECG = electrocardiography, RBBB = right bundle branch block, LBBB = left bundle branch block, QTc = corrected QT interval, Na = serum sodium, BNP = B-type natriuretic peptide, LVEDV = left ventricular end-diastolic volume, BSA = body surface area, LVESV = left ventricular end-systolic volume, LVEF = left ventricular ejection fraction, LA = left atrium, RVSP = right ventricular systolic pressure.
Influence of guideline adherence on clinical outcomes in patients without AF
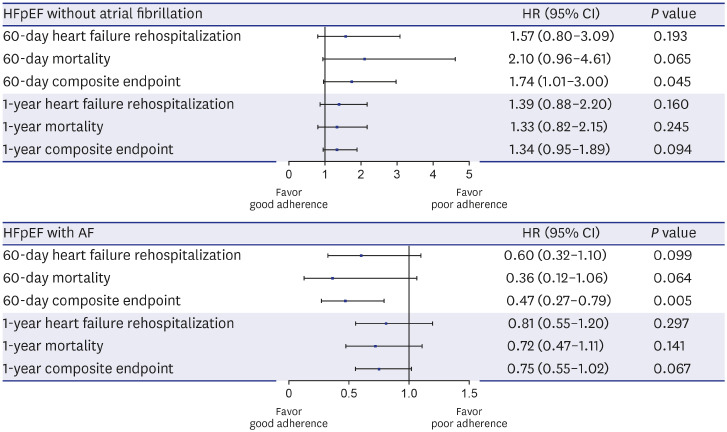
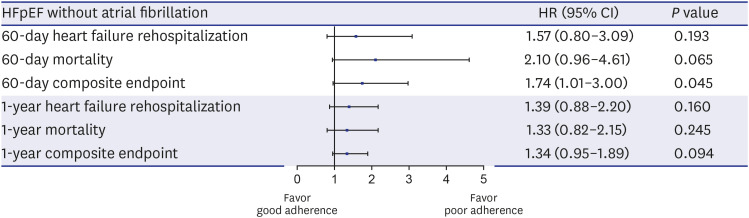
Of the 687 patients without AF, 111 (16.2%) patients died, and 98 (14.3%) patients were re-hospitalized during the 1-year follow-up period. The incidences of clinical outcomes at 60 days and 1 year did not differ according to the degree of guideline adherence (Table 3). The IPTW adjusted Kaplan-Meier survival curves demonstrated better 60-day composite endpoint-free survival in the poor adherence group (Supplementary Fig. 1). After IPTW, good adherence was associated with poor 60-day composite endpoint-free survival in the multivariable Cox model (wHR, 1.74; 95% CI, 1.01–3.00; P = 0.045). Poor adherence was not associated with any risks for 1-year outcomes when compared with moderate or good adherence (Fig. 1, Supplementary Table 3).
Table 3
Clinical outcomes according to guideline adherence in patients without atrial fibrillation
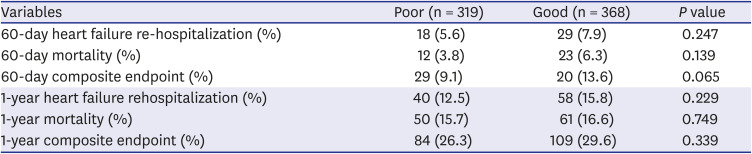
Fig. 1
Inverse probability of treatment weighting-adjusted multivariate Cox regression forest plot of clinical outcomes in patients without atrial fibrillation with good guideline adherence versus those with poor guideline adherence.
HFpEF = heart failure with preserved ejection fraction, HR = hazard ratio, CI = confidence interval.
Influence of guideline adherence on clinical outcomes in patients with AF
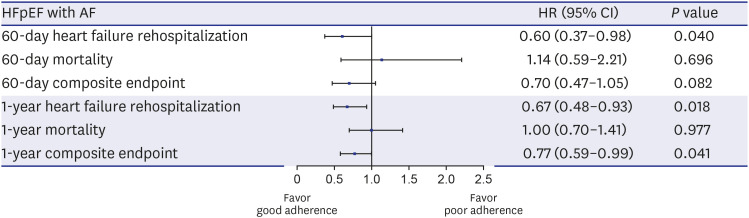
Of the 707 patients with AF, 137 (19.4%) patients were re-hospitalized, and 130 (18.4%) patients died. The incidences of mortality and the composite endpoint during the follow-up period were higher in the poor adherence group than in the good adherence group (Table 4). The IPTW adjusted Kaplan–Meier survival curves demonstrated poor event-free survival among those with poor guideline adherence in terms of 60-day mortality and the composite endpoint. Additionally, the IPTW adjusted multivariate Cox regression analysis revealed that good adherence was significantly associated with the 60-day composite endpoint (wHR, 0.47; 95% CI, 0.27–0.79; P = 0.005) (Fig. 2, Supplementary Table 4). Good adherence was not associated with 1-year clinical outcomes. In the analysis excluding warfarin, good adherence was associated with 60-day re-hospitalization (wHR, 0.60; 95% CI, 0.37–0.98; P = 0.040), 1-year re-hospitalization (wHR, 0.67; 95% CI, 0.48–0.93; P = 0.018), and the composite endpoint (wHR, 0.77; 95% CI, 0.59–0.99; P = 0.041) (Fig. 3, Supplementary Table 5).
Table 4
Clinical outcomes according to guideline adherence in patients with atrial fibrillation
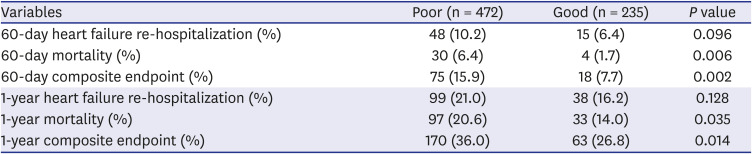
Fig. 2
Inverse probability of treatment weighting-adjusted multivariate Cox regression forest plot of clinical outcomes in patients with atrial fibrillation with good guideline adherence versus those with poor guideline adherence.
HFpEF = heart failure with preserved ejection fraction, AF = atrial fibrillation, HR = hazard ratio, CI = confidence interval.
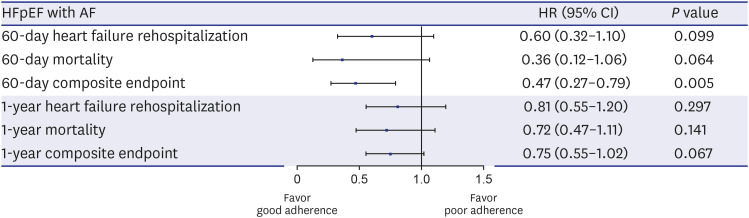
Fig. 3
Inverse probability of treatment weighting-adjusted multivariate Cox regression forest plot of clinical outcomes in patients with good guideline adherence versus those with poor guideline adherence when warfarin was excluded.
HFpEF = heart failure with preserved ejection fraction, AF = atrial fibrillation, HR = hazard ratio, CI = confidence interval.
DISCUSSION
In this study, we investigated the association between the degree of adherence to guidelines for HFrEF and relevant 60-day and 1-year clinical outcomes in patients with HFpEF with or without AF. Our analysis revealed that good adherence to guidelines for HFrEF was associated with a better 60-day composite endpoint in patients with HFpEF with AF. In the analysis excluding warfarin, good adherence was associated with 60-day re-hospitalization, 1-year re-hospitalization, and the 1-year composite endpoint. However, good adherence was associated with a poor 1-year composite endpoint in patients with HFpEF with normal sinus rhythm.
The current guideline recommendation is based on clinical trials that demonstrated an improvement in the outcomes of patients with HFrEF. Traditional pharmacotherapies inhibiting the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system are the cornerstone of treatment for patients with HFrEF without AF. However, HF therapies that reduce mortality and morbidity in patients with HFrEF do not have the same effect in patients with HFpEF. Indeed, several studies have demonstrated that drugs that inhibit RAAS lack efficacy in patients with HFpEF.9192021 In a meta-analysis, RAAS inhibition was not associated with a mortality benefit or reduced HF-related hospitalization when compared with the placebo.22 Additionally, the efficacy of beta-blocker therapy in patients with HFpEF remains elusive.72123
The mechanisms underlying the failed efficacy of RAAS and sympathetic nervous system blockade in patients with HFpEF remain unclear.24 The discordant outcomes of similar pharmacological therapies suggest that the signal transduction cascades driving myocardial remodeling differ in patients with HFpEF and patients with HFrEF. Patients with HFpEF have concentric LV remodeling, while patients with HFrEF have eccentric LV modeling.25 In up to one third of patients with HFpEF, neurohormonal blockade with β-blockers and RAAS inhibitors appears to be less prominent and hence may not be beneficial.2627 This observation may explain the neutral results of trials that tested the role of traditional RAAS inhibitors in patients with HFpEF. Moreover, the underlying pathophysiology of HFpEF is heterogeneous and is associated with different phenotypes, including diverse concomitant cardiovascular diseases and non-cardiovascular diseases.3 In addition, HFpEF has a significantly higher burden of noncardiac comorbidities and hospitalization than HFrEF, and death in patients with HFpEF is more likely to be non-cardiovascular. The increased number of comorbidities has also been associated with an increase in all-cause hospitalizations.28 This finding underlines the importance of comorbidity management for reducing overall morbidity in patients with HFpEF. It is possible that disease-modifying HFrEF therapies in patients with HFpEF may not be able to improve outcomes that are largely driven by competing noncardiac comorbidities.2428 This notion is further supported by the fact that clinical trials adopting a “one-size-fits-all” approach in patients with HFpEF have yielded disappointing results and that treatment modalities applied to a large, undifferentiated group of patients with HFpEF have failed to achieve desirable outcomes.24 In this study, patients with poor clinical characteristics exhibited better guideline adherence, suggesting that patients with more co-morbidities required more extensive therapeutic intervention. We hypothesize that differences in baseline characteristics may neutralize the positive prognostic effects of disease-modifying therapeutics and that good adherence may be associated with poor outcomes in patients with HFpEF without AF.
Aside from anticoagulation therapy, there are no significant remedies for patients with HFrEF or patients with HFpEF and AF.34 The added consequences of AF may also neutralize the mortality benefit of other therapies.29 Although therapies for HFrEF, including RAA and sympathetic blockage, have failed to improve prognostic outcomes in patients with HFpEF, it is possible that accumulating the weak positive prognostic effects of these therapies could exert a significant positive effect in patients with HFpEF.6 The accumulation of traditional HF therapies was represented as a degree of guideline adherence in this study. Guideline adherence indicates the proportion of patients whose physicians have prescribed medication in accordance with established guidelines.17 Furthermore, the non-prescription of recommended medications because of specific contraindications or intolerance was scored as adherence to the guidelines.430 The guideline adherence in this study strictly assessed whether physicians adhered to the guideline recommendations for each patient. The degree of guideline adherence in patients with HFpEF and AF correlated with a favorable prognosis. In the analysis excluding warfarin, guideline adherence was also associated with prognosis.
This study has a few limitations. First, the KorAHF registry was not a randomized control study, but a prospective cohort study. Thus, the prescription of HF therapy was entirely under the control of attending physician, which leads to the possibility of selection bias. Second, the target dose of each recommended medication was not integrated to adherence because physicians usually escalated dose during the follow-up period after stabilization. Third, there may have been changes in HF medication during the patients' follow-up period, and this change may have influenced clinical outcomes. However, the purpose of this study was to evaluate whether adherence to guideline at the time of discharge had prognostic implications. Fourth, AF-specific information was limited, as AF diagnoses were based on electrocardiography findings at admission and past medical history, which may have led to an underestimation of the prevalence of AF in our study cohort.
In conclusion, good adherence to guidelines for HFrEF was associated with 60-day and 1-year clinical outcomes in patients with HFpEF and AF but not in patients with HFpEF without AF. Further investigations are required to aid in the development of optimal therapeutic strategies.
 XML Download
XML Download