

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a pulmonary disorder characterized by irreversible airflow limitation, with a partially reversible component.1 COPD is caused by airway and pulmonary parenchymal damage, which can be prevented and treated. Notably, COPD has a high prevalence and mortality rate worldwide, such that it represents a very large socioeconomic burden.234 The Global Burden of Disease, revised in 2010, reported that 300 million people worldwide have COPD; moreover, 3 million deaths worldwide occur each year, due to COPD.56 The reported prevalence of COPD significantly differs among studies; however, according to research using the Global Initiative for Obstructive Lung Disease guidelines and forced expiratory volume in 1 sec/forced vital capacity (FEV1/FVC) < 0.7, the overall prevalence is 10%.
A biomarker is a measurable substance or molecule that reflects the state and course of a disease.7 Suitable biomarkers can be used to identify patients early and improve the diagnosis of acute or chronic diseases.89 FEV1 is relatively easy to determine in patients with COPD; it is also highly repeatable and is used to track health outcomes. However, FEV1 is difficult to change during treatment, does not reflect disease activity, and is not adequately related to mortality and hospitalization; thus, it is not an ideal biomarker.10 Accordingly, there is an ongoing effort to identify meaningful biomarkers in patients with COPD. However, no ideal biomarkers have been identified.
Word embedding is a method for learning a vector representation of all words in a given corpus. Inferences are added by measuring the similarity among multiple words and performing vector calculations by vectorizing the semantics. In the present study, we investigated the relationships of COPD with its potential biomarkers by using word embedding models, such as Canonical Correlation Analysis, Word2vec, and Global Vector (GloVe).1011
A few studies have attempted to identify new biomarkers for COPD from the literature.12 Word embedding offers the possibility of identifying new biomarkers that may exhibit robust associations with COPD, in addition to known biomarkers. However, word embedding cannot be used to verify the usefulness of a biomarker, because of the lack of clinical trials. In the present study, potential biomarkers were selected using word embedding, then measured in patients with COPD and assessed to determine their correlations with various COPD parameters.
METHODS
Cohort
Patients and controls were selected from the COPD in the Dusty Areas study cohort, which was established to observe the clinical outcomes of patients living near cement plants. The design of this cohort has been detailed in other previous studies.1314 Registered patients were assessed by medical interview, physical examination, spirometry, laboratory testing, and computed tomography. COPD was defined as FEV1/FVC < 0.7 after bronchodilator aspiration.15 COPD grade was defined as grade 2 (50% ≤ FEV1 < 80%), grade 3 (30% ≤ FEV1 < 50%), or grade 4 (FEV1 < 30%), according to the 2017 Global Initiative for Obstructive Lung Disease rating system.
Patients and study design
The COPD and control groups were matched for age, sex, and smoking history. In total, 130 patients were enrolled by one-to-one matching in the cohort; they were classified as 65 patients with COPD and 65 controls (Table 1). The blood concentrations of biomarkers identified by word embedding were examined. Eight patients in the COPD and control groups were excluded because of insufficient blood samples. Thus, 63 patients with COPD and 59 controls were included in the analysis.
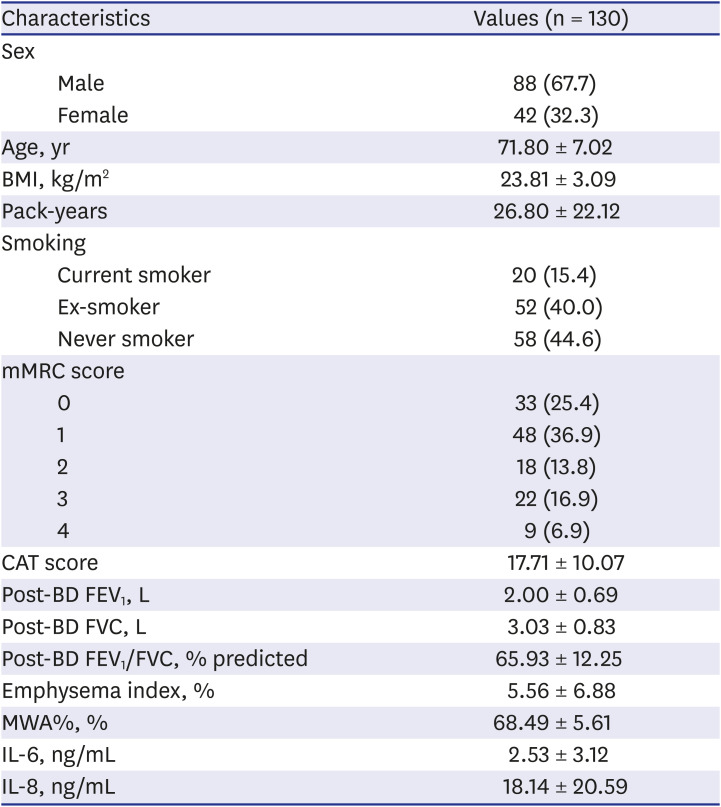
Table 1
Basic characteristics of the participants in this study
The following variables were recorded for the included patients: age, sex, height, weight, smoking history, modified Medical Research Council Dyspnea Scale (mMRC) score, COPD Assessment Test (CAT) score, emphysema index (EI), and mean wall area% (MWA%).
Word embedding and Cyfra 21-1 measurements
To determine the degrees of similarity between COPD and its biomarkers, 26 biomarkers known to be associated with respiratory diseases were selected (Supplementary Table 1).1617 It was difficult to set the criteria for selecting these biomarkers to find new biomarkers of COPD, so we searched the papers for biomarkers related to other lung diseases and chronic disease. And we randomly selected 26 biomarkers for the word embedding. Information related to the biomarkers was extracted from Google searches. Similarities between several words were measured and vector computations with vectorized semantics were performed to enable additional inferences. Relationships between COPD and respective biomarkers were investigated using the Canonical Correlation Analysis, Word2vec, and GloVe word-embedding models. To replace the clinical evaluation, the titles and abstracts of papers retrieved from Google Scholar were analyzed and quantified to estimate the performance of the word embedding models.12
Serum Cyfra 21-1 concentrations were determined using the Cyfra 21-1 enzyme-linked immunosorbent assay kit (Demeditec Diagnostics GmbH, Kiel, Germany), in accordance with the manufacturer’s protocol. Enzyme-linked immunosorbent assay plates were analyzed using a microplate reader (Molecular Devices, Sunnyvale, CA, USA).
Quantitative analysis of CT was performed using an Aview® system (Coreline Soft Inc., Seoul, Korea). Emphysema index was calculated as the volume fraction (%) of the lung below −950 HU at full inspiration. MWA% [defined as WA/(WA + lumen area) × 100], were measured near the origin of the right apical and left apicoposterior segmental bronchi.
Statistical analysis
Statistical analysis was performed using Pearson's χ2 test and the t-test to compare characteristics between the COPD and control groups. Correlation analysis was used to determine the relationships of respective variables with the serum Cyfra 21-1 concentration. Multivariate logistic regression analysis was used to calibrate each variable, including age, sex, smoking, and body mass index (BMI); the correlation between serum Cyfra 21-1 concentration and EI was independently assessed. A P value < 0.05 was considered statistically significant. Data analysis was performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Table 1 summarizes the characteristics of the 130 participants in this study. The proportion of men in the cohort was twofold greater than the proportion of women (67.7% vs. 32.3%). The mean age was 71.8 years, mean BMI was 23.81 kg/m2.
Table 2 shows the similarities between markers with the highest correlation values to COPD in the Word2vec 100 and GloVe 100 dimensions. ‘Title_both’ is the frequency at which the biomarker (eg, ‘CC-16’) appears simultaneously with COPD in the title of a medical paper. And ‘Abs_both’ is the frequency at which the biomarker (e.g., ‘CC-16’) appears simultaneously with COPD in the abstract of a medical paper. The Clara cell secretory protein (recommended by Word2vec) and adiponectin and leptin (recommended by GloVe) were involved in large amounts of research related to COPD. In contrast, eotaxin-1 and Cyfra 21-1 (recommended by Word2vec) and carcinoembryonic antigen and serum amyloid A (recommended by GloVe) were not involved in large amounts of research related to COPD. Notably, Cyfra 21-1 had a high correlation with COPD, but has had minimal research interest.
Table 2
Biomarkers exhibiting highest similarities with chronic obstructive pulmonary disease
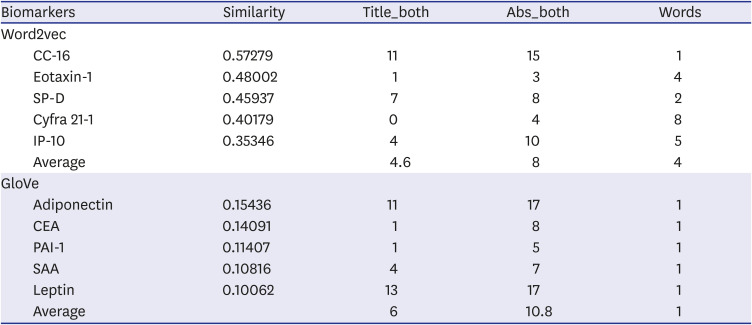
Table 3 shows the demographic and clinical characteristics of the matched COPD and control groups. Significant differences between the two groups were observed in the mMRC score, CAT score, post-bronchodilator (post-BD) FEV1, EI, and MWA. The mMRC and CAT scores were higher in the COPD group than in the control group; the EI and MWA were also significantly higher in the COPD group. No differences were found in the serum levels of interleukin-6 or interleukin-8. No significant differences were detected in serum levels of Cyfra 21-1 (4.3 ± 5.9 vs. 3.9 ± 3.6, P = 0.611) between the COPD and control groups.
Table 3
Basic characteristics of participants in COPD and control groups
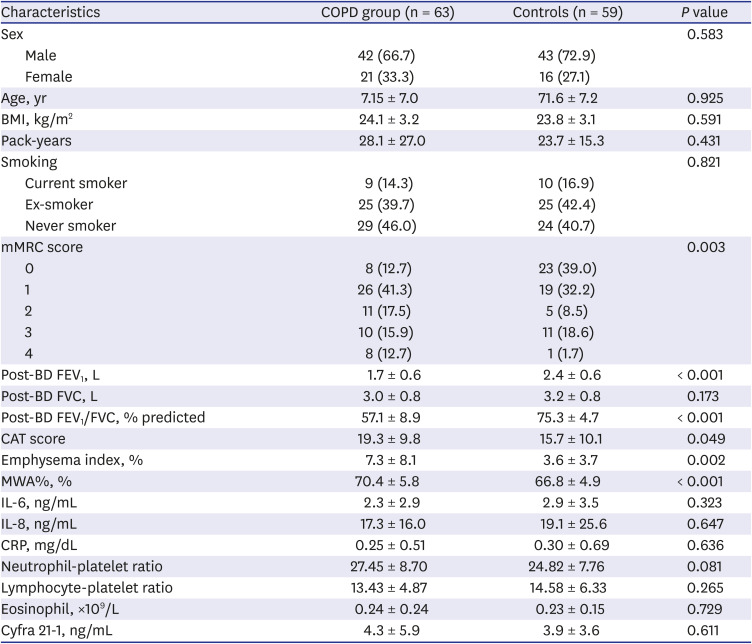
Data are shown as number (%) or mean ± standard deviation.
P value from Pearson's χ2 test.
The neutrophil-platelet ratio was calculated by neutrophil count (×109/L) ×1,000/platelet count (×109/L).
The lymphocyte-platelet ratio was calculated by lymphocyte count (×109/L) ×1,000/platelet count (×109/L).
COPD = chronic obstructive pulmonary disease, BMI = body mass index, mMRC = modified Medical Research Council, Post-BD = post-bronchodilator, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, CAT = COPD assessment test, MWA = mean wall area, IL = interleukin, CRP = C-reactive protein, Cyfra 21-1 = cytokeratin 19 fragment.
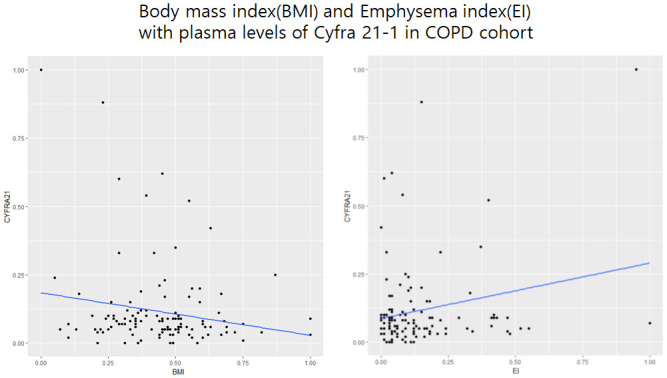
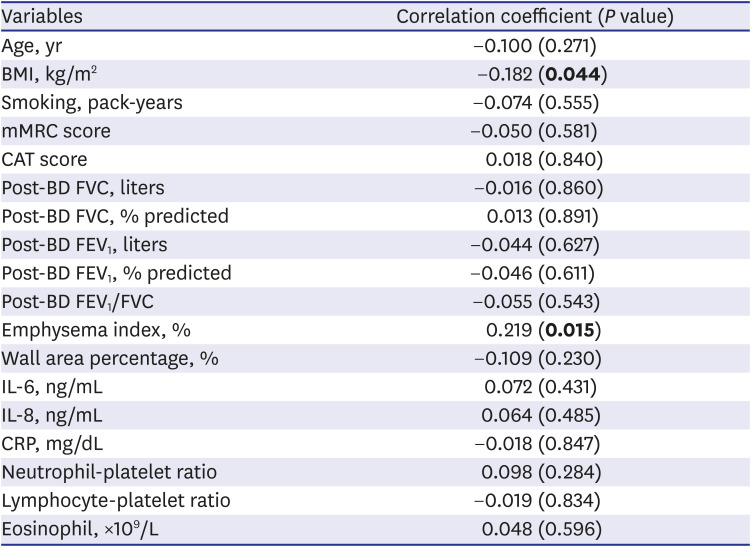
Correlations of demographic and clinical characteristics with serum Cyfra 21-1 concentration were analyzed (Table 4). BMI (P = 0.044) and EI (P = 0.015) were significantly correlated with serum Cyfra 21-1 concentration. Multivariate regression analysis confirmed these correlations: a negative correlation (B = -10.282, P = 0.030) between Cyfra 21-1 and BMI and a positive correlation (B = 8.44, P = 0.046) between Cyfra 21-1 and EI (Supplementary Table 2).
Table 4
Correlations of cytokeratin 19 fragment with clinical and demographic variables
DISCUSSION
In this study, we selected potential biomarkers using word-embedding techniques. We compared the serum concentrations of Cyfra 21-1 between a COPD group and a matched control group in the COPD in the Dusty Areas cohort, with the aim of characterizing Cyfra 21-1 as a potential biomarker for COPD. We found a higher EI and lower BMI in patients with a high serum concentration of Cyfra 21-1. Notably, we found that the serum Cyfra 21-1 concentration was not associated with other COPD clinical indicators, such as dyspnea or pulmonary function.
Word embedding is a method for digitization of a word constituting text. Word2vec was developed by Mikolov, who implemented continuous bag-of-words and Skip-Gram word embedding.10 Words can be embedded based on their meaning in the context of surrounding words. A sufficient number of documents is collected in the target field; embedding is then performed in a low-dimensional space using a representative technique (i.e., Word2vec). The embedded space is generated by reproduction of the contextual meaning of the corresponding vocabulary; if a particular word is very positive, it can be inferred that words near the corresponding word are also likely to have a positive meaning.18 Various studies have used word embedding; recent research on cancer and biomarkers has provided a new method to study potential biomarkers.19
COPD is a disease with high prevalence and mortality rates worldwide.20 Pulmonary function tests is relatively easy to determine from patients with COPD, with repeatability and ease of tracing; however, it is not an ideal biomarker because it does not reflect disease activity and is not associated with acute hospitalization, mortality, or quality of life.21 Ideal biomarkers improve patient care by allowing early detection of clinical conditions, thereby improving the diagnosis of acute or chronic diseases; they also enable prediction of patient risk, determination of optimal treatment for a given patient, observance of disease progression, and observance of the response to treatment.22 Many studies have been conducted to identify ideal biomarkers of COPD.232425
Cyfra 21-1 is a cytokeratin 19 segment that was identified as a marker of lung cancer in 1993. It has been repeatedly validated as a marker for non-small cell lung cancer.2627 The Cyfra 21-1 serum tumor marker was related to the proximity of COPD using the Word2vec technique.12 In our study, serum Cyfra 21-1 levels were significantly correlated with BMI and EI values. In a study of the clinical utility of the tumor marker Cyfra 21-1 in health assessments, factors affecting Cyfra 21-1 were age, sex, smoking status, blood pressure, diabetes, and hepatitis B infection; no analysis of height or weight was performed in that study.27
To the best of our knowledge, the present study is the first to reveal associations of Cyfra 21-1 with BMI and the EI. Thus, in addition to its role as a marker for cancer, Cyfra 21-1 constitutes a marker for benign pulmonary disease. Several studies have shown increased Cyfra 21-1 levels in patients with interstitial pulmonary fibrosis, collagen disease-associated pulmonary fibrosis, and autoimmune pulmonary alveolar proteinosis.222627
There were some limitations in our study. First, we did not consider additional variables associated with Cyfra 21-1 (e.g., hepatitis B infection, diabetes, and blood pressure), which were identified in previous studies. In particular, serum Cyfra 21-1 levels are known as adjuvants for the diagnosis and prognosis of lung squamous cell carcinoma.28 Additionally, Cyfra 21-1 has recently been reported to be elevated in idiopathic pulmonary fibrosis or head and neck squamous cell carcinoma.29 In our cohort, COPD patients did not have enough patients with underlying diseases to analyze these underlying diseases (Supplementary Table 3).30 Second, word embedding study was designed to review other potential biomarkers, in addition to Cyfra21-1. However, only one marker was identified due to research cost limitations. Third, COPD is a heterogeneous disease caused by a combination of small airway disease (chronic bronchitis) and parenchymal destruction (emphysema).31 However, there is a limitation that cannot be analyzed because there is no information according to the type of COPD in our cohort. Finally, even in the analysis based on the GOLD group, there were only 2 patients with stage 3 or higher, which could not be sufficient for analysis (Supplementary Table 4).
Our study is the first to identify a biomarker for COPD using word embedding. We measured serum Cyfra 21-1 concentrations in the COPD and control groups. Correlations of BMI and EI with Cyfra21-1, which were not identified in previous studies, were confirmed. Active research regarding the use of word embedding in various medical fields is expected to be performed in the future. Cyfra 21-1, BMI, and EI should be assessed in patients at risk of COPD, in addition to the conventional parameters of age, diabetes, cancer, and infection.
In conclusion, Cyfra 21-1 concentration was correlated with EI and BMI. Word embedding is expected to be involved in the discovery of new biomarkers for COPD and other medical conditions.
 XML Download
XML Download