

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Surge capacity refers to the ability to deal with the rapidly increasing patients who need to be admitted and use available resources in the event of a disaster or multiple injuries.12 Surge capacity can be divided into three categories: the public health system's total capacity, the community's capacity, and a specific facility's capacity according to the host.3 Individual health care institutions play the role of “the first tier” in the earliest stages of a health care disaster response.4 Emergency departments (EDs) are always faced with ensuring patient safety by managing critical supply/demand mismatch, which is the main portal into the healthcare system.5
Measurement standards for surge capacity have not yet been developed, but there is a consensus on the main components, known as “4S's” for “staff,” “stuff,” “space,” and “systems.”6 It is difficult to measure a disaster surge objectively; most previous studies have proposed conceptual calculation methods based on theory and assumptions.7 It is difficult to define hospital surge capacity standardly as various studies have reported that it can increase up to 5 to 35% of hospital beds.8 Some consensus statements recommend raising the intensive care unit (ICU) expansion goal to 200% of usual capacity during a crisis.9
Several studies have quantitatively calculated surge capacity. In these studies' early paper, an increase by 3% of the number of beds per hour was suggested as hospital treatment capacity.10 In a study that calculated the surge capacity of a specific level 1 trauma center through computer modeling, the number of critical patients who could be treated per hour rose from 4.6 to 7.1.11 In another study, surge capacity was estimated by surveying the actual number of patients treated during the same day at 133 trauma centers.12 In studies benchmarking the above quantitative studies, hospital acute care surge capacity was defined as the number of ED beds divided by the ED time (2.5 hours).13
To date, qualitative and quantitative studies on surge capacity assume that the hospital's capacity can be maximized in case of a disaster or multiple casualty incidents (MCIs). Actual surge capacity can be severely limited due to overcrowding in hospitals and EDs, as it is currently required to maintain treatment continuity for all other patients.5 Therefore, enquiring EDs in a specific region about their official surge capacity and preparedness for MCIs can help measure the entire community's actual surge capacity and capability. We investigated the surge capacity of the specific number of accommodatable patients and overall preparedness at EDs in a metropolitan city. Moreover, we tried to estimate the city's surge capacity and analyze the hospital variables that affect surge capacity.
METHODS
Study setting
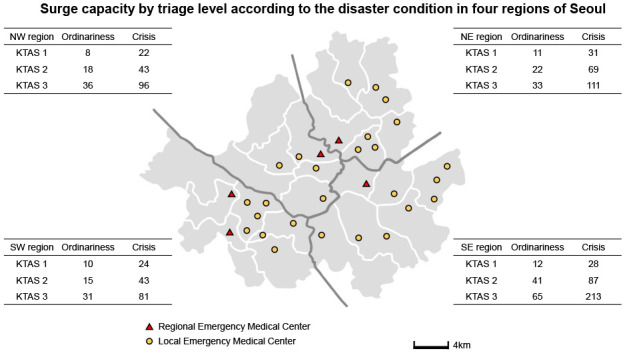
This study was conducted in Seoul, South Korea's capital, and was conducted as part of the public health division of the Seoul metropolitan government's “Development of medical response protocol for MCIs.” Seoul is a metropolitan city with about 600 square kilometers and a population of about 10 million as of 2018.14 In Seoul, there are five regional emergency medical centers (EMCs), 26 local EMCs, and 17 local emergency medical institutions (EMIs). Regional EMC provides the highest level of emergency medical care in the region. Legally, it functions as a base hospital for disaster preparedness and response. It dispatches the hospital's disaster medical assistance team (DMAT) to the site and designates an emergency treatment area for multiple casualties. However, specific budget support for this is insufficient. As of 2018, thirteen level 1 trauma centers have been designated in the entire country, but no emergency facilities have been designated as trauma centers in Seoul. Regional EMC and local EMC serve as a level 2 or level 3 trauma center. Seoul is divided into four emergency medical regions, with one regional EMC in each region, which is responsible for accommodating casualties in the event of MCIs or disasters in close cooperation with local regional EMCs. Local EMIs perform the role of accommodating patients with minor cases (Table 1). There have been no significant casualties in Seoul, except the Sampoong Department Store's collapse in 1995 that resulted in 1,399 casualties.15 However, compared to other municipalities, medium-sized MCIs frequently occurred in Seoul. Therefore, the Seoul Metropolitan Government's Public Health Division and the five regional EMCs made councils and regularly held meetings to discuss disaster preparedness and the city's medical surge capacity.

Study design
This cross-sectional study surveyed the surge capacity and disaster preparedness for all regional and local EMCs in Seoul. From September 2017, representatives of five regional EMCs in Seoul formed the regional EMC council for disaster medical preparedness and met monthly. The council decided to investigate primary data for future surge capacity planning and discussed how to measure Seoul's hospital surge capacity. It was decided upon to conduct an official survey on regional and local EMC in Seoul to evaluate the surge capacity planned by the hospital. Survey questions were developed after detailed discussions regarding international guidelines and research. The main content of the survey question is the question that confirms 4S (space, staff, stuff, and system). The questions enquired about the following: the number of EMC beds, hospital beds, and operation room (OR) beds; the number of medical staff in hospital and EMC; the specific number of accommodatable patients in the surge capacity; staff; drill and education; command and control; communication; security and safety; triage. The ED type was divided into regional EMCs (disaster-based hospital) and local EMCs, also the hospital type was divided into superior general hospital or general hospital.
The specific number of patients that could be accommodated was investigated under two conditions: “Ordinariness (or conventional)” and “Crisis”. It refers to the number of patients that EMC can accommodate within first one hour, either maintaining a usual level of care or using maximum medical resources. All EMC in Korea uses the Korean Triage and Acuity Scale (KTAS) to assess patient severity.16 Therefore, the number of acceptable patients was asked as KTAS level. KTAS is divided into five stages, from KTAS 1, which requires immediate aggressive treatment due to life-threatening conditions, to KTAS 5, which is a non-emergency visit due to chronic illness. In general, patients with KTAS 1–3 are considered emergency patients, and those with KTAS 4–5 are considered non-emergency patients. Furthermore, a survey was conducted on the number of patients requiring emergency surgery or ICU admission. Depending on each hospital's policy, KTAS 4 and 5 may not be accepted because they are non-emergency patients. The surge capacity for KTAS 4 and 5 was calculated excluding such hospitals.
After completing the survey items, a survey on regional EMC was first conducted for two months from July 2018. The survey paper was officially sent from the Seoul Metropolitan Government to the regional EMC director. After receiving the response, the survey questions were revised according to the local EMC. Local EMC surveys were conducted over two months from September 2018. After receiving all responses from the local EMCs, each center's surge capacity was reviewed by the specific region's regional EMC director, and extremely small or large numbers were adjusted to other centers.
Of the total 31 hospitals, 29 sent all survey data. Two local EMCs only sent the contents about the ability to accommodate the surge. Therefore, the accommodatable surge capacity was analyzed based on data from 31 hospitals, while another analysis was based on twenty-nine hospitals.
Calculation of surge capacity
It is necessary to define the formula of surge capacity to statistically analyze each hospital's surge capacity. Since the severity of the patient depends on KTAS level, the surge capacity cannot be expressed only as the sum of KTAS. The Emergency Medical Response Manual for Disasters in South Korea mentions that immediate (“red”) patients should be allocated three to six times more resources than delayed (“yellow”) patients.17 In this study, KTAS 1 and 2 were converted into immediate (“red”) patients,18 and KTAS 3 were converted into delayed (“yellow”) patients. Compared to KTAS 3, it is assumed that KTAS 1 and KTAS 2 requires six and three times more resources, respectively. KTAS 4 and 5 were excluded from the surge capacity calculation formula because they were non-emergency patients. According to the regional EMC council for disaster medical preparedness and response's expert consensus, the surge capacity was calculated as follows:
Surge capacity of the emergency medical facility = Number of acceptable KTAS 1 patients × 6 + KTAS 2 patients × 3 + KTAS 3 patients
We assumed that there are no differences in medical staffs' capability between regional and local EMCs.
Statistical analysis
In this study, there were no normally distributed variables examined by the Kolmogorov-Smirnov normality test owing the small sample size. The Mann-Whitney U test was used to compare the two independent groups, and the Wilcoxon signed rank test was used to compare the paired two groups. Fisher's exact test was used for categorical variables. Multivariable linear regression analysis was conducted for selected variables related to surge capacity. Variables were presented as median, 25th percentile–75th percentile due to skewed data. A P value < 0.05 was considered statistically significant. SPSS Statistics (SPSS 20.0; IBM, Armonk, NY, USA) was used for statistical analysis.
RESULTS
Surge capacity of EMCs in the Seoul Metropolitan City
It was found that when KTAS 1–3 are considered emergency patients and KTAS 4–5 are non-emergency patients, all regional and local EMCs in Seoul can accommodate 313 emergency patients and 210 non-emergency patients in ordinary situation, while 848 emergency patients and 537 non-emergency patients in crisis condition (Table 2). If this is calculated as the average value per EMC, one EMC can accommodate 1.3 patients with KTAS level 1, 3.1 with KTAS 2, and 5.7 with KTAS 3 in ordinary situation. A total of 16 EMCs responded that KTAS 4 or 5 patients could be accommodated. These EMCs also mentioned that each EMC could accommodate an average of 6.3 KTAS 4 patients and an average of 6.8 KTAS 5 patients. In crisis, the number of patients that could be accommodated per hospital was 3.4 KTAS 1, 7.8 KTAS 2, and 16.2 KTAS 3 patients. A total of 17 EMCs answered that they could accommodate four or five KTAS patients in a crisis; they could accommodate an average of 15.1 KTAS 4 and 16.5 KTAS 5 patients. Regarding availability of ICUs, 37 patients could be provided with the facility in ordinary circumstances and 31 during an emergency operation. During the crisis, this number increased to 98 and 71, respectively. According to the surge capacity calculation formula, the surge capacity of the EMC in Seoul during ordinariness and crisis was 22.9 and 59.9, respectively.
Table 2
The number of patients accommodatable by region and EMC according to the severity
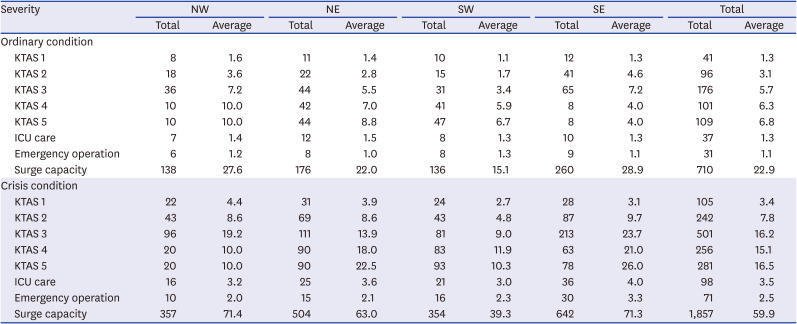
This table is the data of 31 EMC. The values presented are the total number of patients accommodatable in the region and the average number of patients per emergency medical center. The denominator of the average value is the number of EMCs responding to the survey. Surge capacity = Number of acceptable KTAS 1 patients × 6 + KTAS 2 patients × 3 + KTAS 3 patients.
EMC = emergency medical center, NW = northwest, NE = northeast, SW = southwest, SE = southeast, KTAS = Korean Triage and Acuity Scale, ICU = intensive care unit.
The comparison of the number of accommodatable patients according to the severity in ordinary and crisis conditions
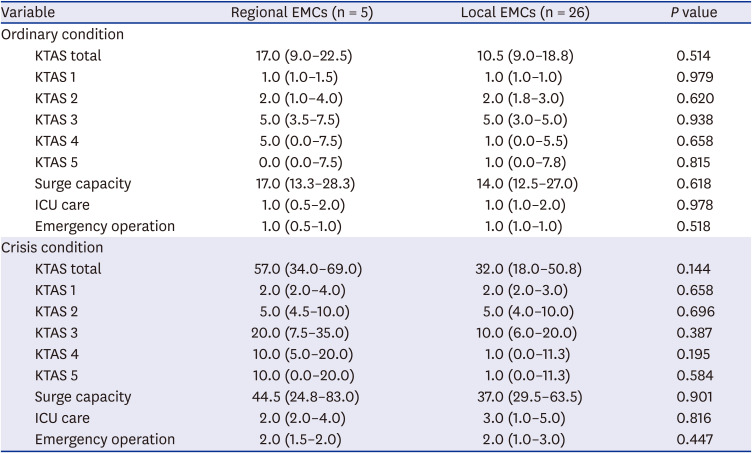
There were significant differences in surge capacity between the ordinary condition (median, 17.0; interquartile range [IQR], 13.0–27.0) and crisis condition (median, 43.0; IQR, 28.0–80.0) (P < 0.001). Moreover, there were significant differences in the ability to accommodate the number of patients regardless of KTAS classification, the number of patients classified by KTAS, and those requiring intensive care and emergency surgery (P < 0.05) (Fig. 1). However, when the subgroup analysis was performed between regional EMCs and local EMCs in ordinariness and crisis conditions, there were no significant differences in surge capacity, the accommodatable capacity according to KTAS classification, and the number of patients who needed intensive care and emergency operation (Table 3).
Fig. 1
Box plot on the overall differences of the ability to accommodate patients during ordinary and crisis condition according to the classification of severity by KTAS, surge capacity, need for ICU care, and emergency operation (n = 31).
KTAS = Korean Triage and Acuity Scale, ICU = intensive care unit.
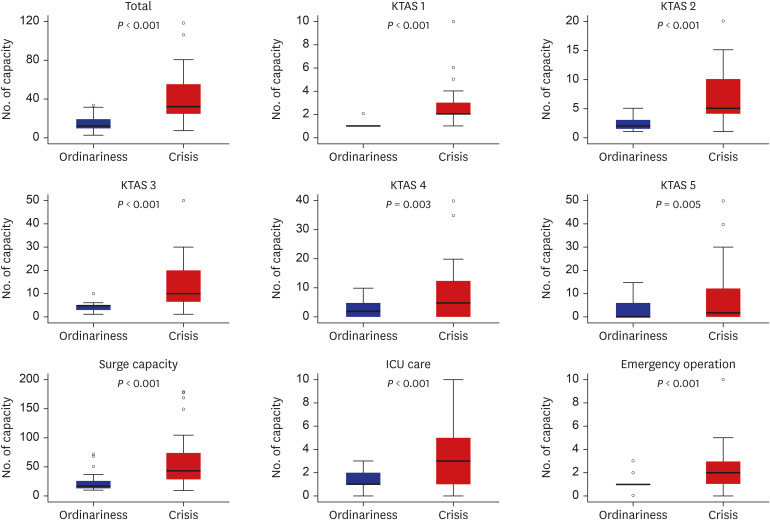
Table 3
Comparison between regional EMCs and local EMCs about the number of patients to accommodate according to the severity in ordinary or crisis conditions
The comparison of the overall medical resources and preparedness
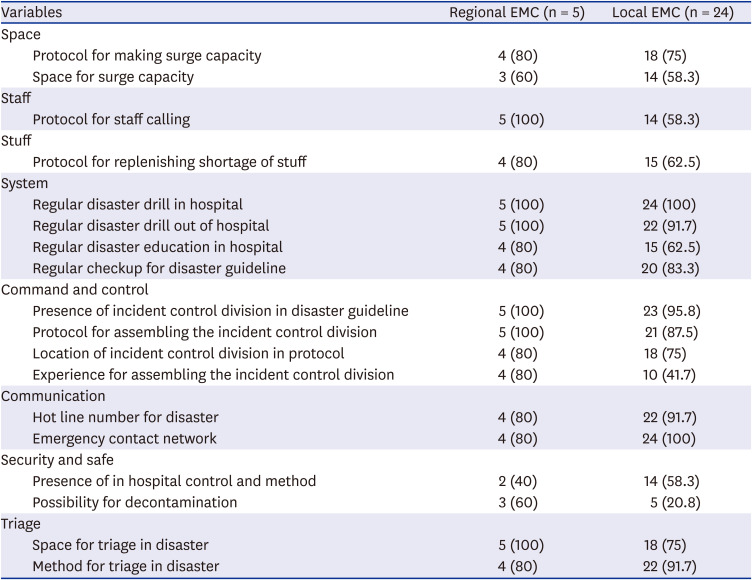
Compared with the overall medical staff and beds, including in the total hospital, ED, and operating room between regional EMCs and local EMCs, regional EMC had significantly more medical resources than local EMCs (P < 0.05). However, there was no significant difference in the number of doctors working in the ED (Fig. 2). Three regional EMCs (60%) and 14 local EMCs (58.3%) had the space available for surge capacity. However, compared with the surge capacity, regional EMCs could accommodate 150.0 ± 86.6 patients, while local EMCs had space for 26.8 ± 24.2 patients. There were no significant differences in the overall preparedness between regional and local EMCs (Table 4).
Fig. 2
Box plot on the overall differences in the number of medical staffs and beds between regional EMC (n = 5) and local EMC (n = 24).
EMC = emergency medical center, ED = emergency department, ICU = intensive care unit, OR = operation room.
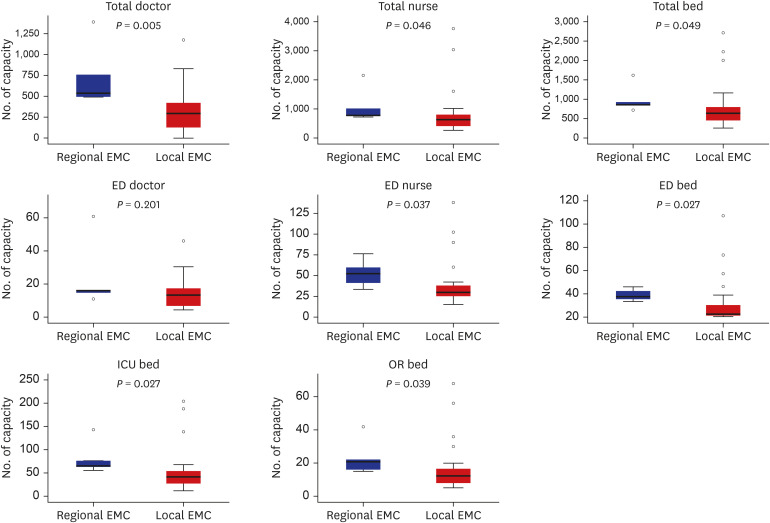
Table 4
Comparison of space, staff, stuff, and system related to the surge capacity between regional EMC and local EMC
Multivariate linear regression analysis for selected variables related to surge capacity
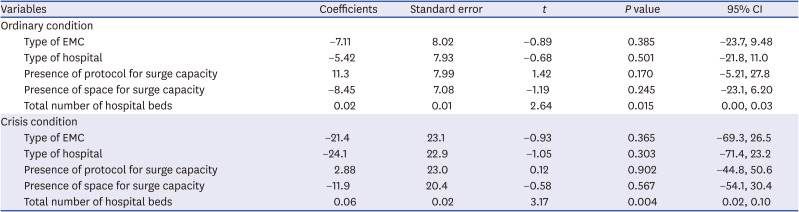
Type of EMC, type of each hospital, presence of protocol for surge capacity, space for surge capacity, and the total number of hospital beds were selected as multivariate linear regression analysis variables. The total number of ED beds, number of doctors and nurses in the ED, and hospitals were excluded from the analysis because there was a clear correlation with the total number of hospital beds. In both ordinary and crisis conditions, only the total hospital beds were significantly associated with surge capacity (Table 5).
Table 5
Multivariate linear regression model for predictors of surge capacity
DISCUSSION
In this regional survey study, 31 regional and local EMCs were asked about the number of patients that could be accommodated within one hour in case of a disaster or multiple accidents. Assuming that KTAS 1–3 were emergency patients, about 300 patients (10 per hospital) were acceptable in the conventional phase. This number increased by 2.5 times in a crisis phase, with about 850 emergency patients (25 per hospital) throughout the city. To the best of the authors' knowledge, this is the first study in South Korea to investigate the surge capacity and preparedness for each hospital in a specific region when MCI or disasters occur.
In South Korea, regional EMCs play the role of disaster-based hospitals. The main task of such hospitals is dispatching DMATs to the scene; however, there is a dearth of focus on hospital preparedness and the surge capacity of each hospital.19 The Emergency Medical Response Manual for Disasters published by the Ministry of Health and Welfare is the primary basis for the disaster medical assistance system in South Korea.17 In this manual, a chapter is devoted to the hospital disaster response. However, it does not explicitly mention the definition and calculation method of surge capacity. It remains difficult to properly implement the even transfer of multiple casualties from the field to hospitals.20 Since 2014, the Disaster Emergency Medical Services Situation Room operated by the National Emergency Medical Center has been intermediating communication between the field and the hospital. When any MCI occurs, the situation room quickly checks the capacity of hospitals around the scene. The number of patients that can be accommodated is reported by each emergency medical facility, considering various resource situations. A method of checking directly with the person in-charge of each institution was selected in this study because each EMI determines its surge capacity in the actual situation.
There were no significant differences in the number of accommodatable patients in ordinariness or crisis conditions between regional EMCs and local EMCs. Regional EMC has more resources than local EMC, but the number of ED doctors remains the same. Several studies have shown that even if there was sufficient capacity for multiple casualties and disasters, a lack of medical personnel caused a decrease in staff occupied beds.2122 Patients generally begin to arrive approximately 15 to 30 minutes at EMCs, 50% of patients arrive within approximately an hour and 80% within 90 minutes.2324 Moreover, the hospital begins to suffer from a lack of medical resources within two hours.2526 It takes some time to activate the disaster plan and convene a medical team to respond to disasters and multiple casualties. Initially, EMCs have no choice but to cope with their existing medical staff. Therefore, despite the sufficient medical resources in regional EMCs, the absence of a difference in the number of medical staff (especially doctors) working in EMCs may have caused these results. As shown in Fig. 2, regional EMCs and local EMCs have different resources. Therefore, there is a possibility that regional EMCs will have more free space. However, there was no statistically significant difference in surge capacity for at least the first hour. If a surge occurs continuously for more than several hours, regional EMCs with more free space or resources could show higher surge capacity than local EMCs.
Because of limited surge capacity within an hour to accommodatable patients, the number of KTAS 1–3 patients that each regional and local EMCs can accommodate is smaller than expected. In a crisis, all regional and local EMCs in Seoul can accommodate 848 emergency patients. Several studies showed that although Surge capacity may vary slightly depending on each hospital's situation, it can increase the number of beds by 20%–30% quickly.3132728 Initially, space is secured by moving patients in EMCs to the wards, using emergency space, and discharging patients hospitalized via the reverse triage.2829 In the United States, the Department of Health and Resources announced at least 500 beds for every one million residents for surge capacity to use in the event of a disaster.3031 In addition, the surge capacity is affected by the rate of occupied beds of the ward.303132 According to the results of the 2016 survey in Korea, the percentage of occupied beds is almost 98% on average.33 The institutions that participated in this study had 800 beds to prepare for MCIs and disasters (about 82.5 beds per million people). Therefore, these high rates of occupied bed and lack of prepared space available for surge capacity may lead to a decrease in the number of accommodatable patients.
Misclassification and misallocation at the pre-hospital level significantly impact the patient's survival rate in a crisis.3435 There is at least one regional EMC and four local EMCs in one region, Seoul. Regional EMCs accommodate a minimum of 34 patients in crisis conditions, including at least two KTAS 1 patients and two KTAS 2 patients. Local EMCs also accommodate a minimum of 18 patients in these conditions, including the same KTAS 1 and KTAS 2 patients in regional EMCs. Therefore, when there are approximately 100 or more patients, it becomes beyond one area's capacity. Since regional EMCs and local EMCs can accommodate at least two KTAS l and KTAS 2 patients to help clarify the severe patients' allocation, patients can be distributed and transferred at the pre-hospital level one by one to regional and local EMCs. In this study, the scale of multiple casualty accidents or disasters was not simulated. The surge capacity was measured based on the increase in the frequency of simple visits. It was surveyed that all hospitals in Seoul can accommodate more than 300 KTAS 1 or 2 patients in the crisis phase. Therefore, it is theoretically possible to accept all severely injured patients from very large-scale disasters in Seoul. However, this assumes that the disaster emergency medical system works ideally. The development of sophisticated guidelines for on-site patient distribution and hospital accommodation is needed to apply them to real-world situations.
Hospital resource-related variables that can affect surge capacity were analyzed through multivariate regression analysis. The total number of hospital beds was only found to be significantly related to surge capacity. The number of ED beds and the number of doctors and nurses in the ED or hospital were highly correlated with hospital beds. Therefore, it can be interpreted that the overall hospital resources and surge capacity are related. Regulations on each hospital or role of EMC in a disaster situation did not seem to correlate significantly with surge capacity. Public support is needed so that hospitals with larger surge capacity can play a more important role in a disaster, or disaster-based hospitals can accommodate more casualties.
We did not analyze the quality of care in EMCs according to the size of the patient surge. However, as the size of the patient surge increases, the quality of care may decrease due to insufficient supply, which may result in poor clinical outcomes. For example, the quality of care in ordinariness and crisis may be different. In future studies, it is necessary to consider the quality of care provided according to the size of the patient surge.
This study has several limitations. First, the participants of this study were limited to regional and local EMC in Seoul. The resource situation of local EMI in Seoul may be different. For MCIs and disasters, the ED and other departments in the hospital will respond together. Therefore, even within the same hospital, departments other than the ED may have different opinions. Second, the surge capacity was measured by the official opinion of the ED director in this study. A third party did not objectively measure the surge capacity of the institution as only little is known about how to measure surge capacity easily. In actual MCI situations, the Disaster Emergency Medical Services Situation Room uses a method of directly asking each ED about the type and number of patients acceptable. Therefore, we think that the surge capacity measured in this study was quite close to reality. We propose a simulation study method to contact all EDs within a specific area on the same day to investigate acceptable patients. Third, it is not easy to match the field severity classification (e.g., SALT or START) with the KTAS classification. The surge capacity calculation formula was proposed through expert discussion within the committee, however, additional validation is needed. Fourth, this study mainly measured the hospital's capacity and did not measure the capability of the medical staff. Capabilities between hospitals of similar size may differ. Fifth, when measuring surge capacity, the number of patients the clinical workforce can handle per hour is essential. Unfortunately, this study did not investigate this variable separately. In this study, we assumed that patients due to multiple casualties occurred simultaneously. In this scenario, all patients were transferred to the hospital within the first hour, and the on-site situation was terminated. In the case of a catastrophic surge that spans hours or days, the incident command center of the hospital should consider the hospital's ability to handle it per hour. Finally, since this study was conducted in South Korea's largest metropolitan city, it has limitations in its generalization. It may not be easy to apply this study's results to other regions of South Korea or other countries.
In conclusion, at an average level of MCI, in which less than 20 immediate casualties occur in Seoul, it can be accommodated while maintaining the standard of routine care in each region. In the event of a greater level of MCI or disaster, EDs in the region may have to enter the crisis response stage. The surge capacity of a specific area can be estimated using the method used in this study. More detailed follow-up studies are needed to prepare a surge capacity protocol in the community.
 XML Download
XML Download