

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is associated with an increased risk of ischemic stroke, and oral anticoagulants (OACs) with vitamin K antagonist (VKA), e.g. warfarin, or non-VKA OACs (NOACs), could effectively reduce the risk of AF-associated stroke.1)2) Compared to warfarin, NOACs were much safer regarding the risk of intra-cranial hemorrhage (ICH) in the pooled meta-analysis of 4 pivotal radomized trials.2) In the real-world daily practice, the annual risk of ICH of NOAC-treated patients was lower than 1% even for those aged >90 years.3) Actually, the introduction of NOACs has transformed the landscape for stroke prevention and led to a better clinical outcome in AF patients.4) For stroke prevention in AF, it is crucial to assess the stroke and bleeding risks of individual AF patients to make appropriate decisions for OAC use and achieve optimal patient care. This review article aimed to provide an overview on the correct use of CHA2DS2-VASc and HAS-BLED scores, and to update important revisions about the definitions of some of the CHA2DS2-VASc components. Also, data about the biomarkers and potential roles of AF duration and left atrial functions in the prediction of stroke in AF were also discussed.
STROKE RISK ASSESSMENT
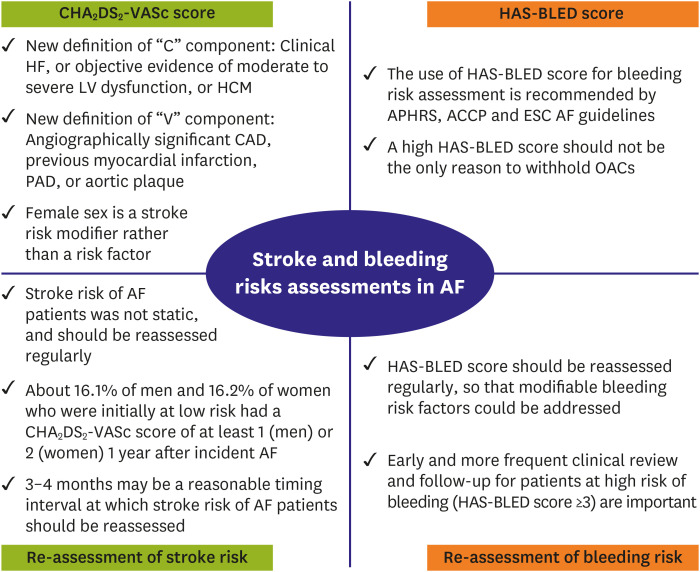
Four important international guidelines, including 2017 Asia Pacific Heart Rhythm Society, 2018 American College of Chest Physicians (ACCP), 2019 American College of Cardiology/American Heart Association (ACC/AHA)/Heart Rhythm Society and 2020 European Society of Cardiology (ESC), all recommend the use of CHA2DS2-VASc score for stroke risk assessment (Table 1).5)6)7)8)9) There were some differences regarding the definitions of “C: congestive HF” and “V: vascular diseases” components between the original version and revised version of CHA2DS2-VASc score in 2020 ESC guidelines.
Table 1
Stroke and bleeding risk assessments and the thresholds for OACs in different guidelines

| Guidelines | Recommendations for stroke prevention based on CHA2DS2-VASc score | Scoring scheme suggested for bleeding risk assessment |
|---|---|---|
| 2017 APHRS5) | OACs for patients with a score ≥1 (males) or ≥2 (females) | HAS-BLED score |
| 2018 ACCP6) | OACs should be offered for patients with a score ≥1 (males) or ≥2 (females) | HAS-BLED score |
| 2019 ACC/AHA7) | Class I recommendation: OACs for score ≥2 (males) or ≥3 (females) | No specific bleeding score was recommended |
| Class IIb recommendation: OACs for score 1 (males) or 2 (females) | ||
| 2020 ESC8) (similar to 2016 ESC guidelines) | Class I recommendation: OACs for score ≥2 (males) or ≥3 (females) | HAS-BLED score |
| Class IIa recommendation: OACs for score 1 (males) or 2 (females) |
“C” components
In the conventional version of the CHA2DS2-VASc score published in year 2010,10) the “C’ refers to congestive HF or left ventricular (LV) dysfunction, which only focused on HF with reduced LV ejection fraction (LVEF) (HFrEF). Since HF with preserved ejection fraction (HFpEF) is more and more common in the daily practice, a clear suggestion about how to treat AF patients with HFpEF regarding stroke prevention is required. In the previous study from Loire Valley Atrial Fibrillation Project reported by Banerjee et al.,11) AF patients with HFpEF were defined as those with clinical HF and LVEF ≥50%, who were more likely to be female (p<0.001), older (p<0.001), and hypertensive (p<0.001), and less likely to have prior vascular disease (p<0.001). There were no differences in rates of stroke (p=0.17) between patients with HFrEF or HFpEF.11) In a recent study from South Korea, a total of 10,780 AF patients were enrolled and divided according to HF type: no-HF (n=9,666), HFpEF (LVEF ≥50%; n=487), HF with mid-range ejection fraction (HFmrEF; LVEF 40–49%; n=263), and HFrEF (LVEF <40%; n=364).12) The stroke/systemic embolism (SE) risk was higher in the HFpEF group than in the HFmrEF and HFrEF groups (hazard ratio [HR], 3.192; p=0.043), with E/e′ value as an independent risk factor.12) Therefore, in ACCP and ESC guidelines, patients with either HFrEF or HFpEF would assigned 1 point for the “C” component.
The ESC guidelines also included hypertrophic cardiomyopathy (HCM) as the “C” component, which was similar to the recommendation of Japan Cardiology Society suggesting that OACs may be considred for patients with cardiomyopathy.13) In the Korean Nationwide study, the incidence rates of ischemic stroke were higher for OAC-naïve AF patients with HCM (n=8,946) than those without HCM (n=884,559)(6.06 per 100 person-years vs. 3.37 per 100 person-years; p<0.001).14) When there was no stroke risk factor other than HCM, the stroke risk of AF patients with HCM was greater than that of patients without HCM with a CHA2DS2-VASc score of 2.14) Most importantly, despite a higher stroke risk, OACs were prescribed in only 15.3% of AF patients with HCM at the time of AF diagnosis in the Korean cohort, suggesting that more efforts are necessary to improve the awareness of recognizing HCM as a risk factor of stroke. Furthremore, compared to warfarin, NOASc were associated with a lower risk of all-cause mortality and composite fatal cardiovascular events and should also serve as the first-line choice of OACs for AF patients with HCM.15)
“V” component
For the coronary artery disease (CAD) of “V” component, the original version of the CHA2DS2-VASc score only included patients with prior myocardial infraction, and did not clearly state about how to deal with “angiographically significant CAD”. In the study performed by Steensig et al.16) which investigated 12,690 AF patients undergoing coronary angiograpy, the presence of CAD (n=7,533; 59.4%) was an independent risk factor for the occurrence of ischemic stroke, transient ischemic attack or SE (incidence rate ratio, 1.25; 1.06–1.47) while the extent of CAD defined as 1-, 2-, 3- or diffuse vessel disease did not add additional independent risk information. The 2020 ESC AF guidelines clearly suggest that “angiographically significant CAD” should be assigned 1 point for stroke risk assessment for the “V” component,8) and how to manage these patients is clearer now.
Age
The cutoff values (65–74 years and >75 years) of age defined in the CHA2DS2-VASc scheme is mainly for the convenience of clinical use, and actually, the association between age and risk of ischemic stroke is a continuous curve. In the prior report from Taiwan AF cohort, even for AF patients aged <65 years without any risk factor components of the CHA2DS2-VASc scheme, the annual risk of ischemic stroke continuously increased from younger to older age groups.17) For Taiwanese AF patients aged 50 to 64 years of age, the annual stroke risk was around 1.78%, which may already exceed the threshold for OAC use for stroke prevention.17) The study from South Korea also demonstrated that AF patients aged 55 to 59 years with no risk factors had a similar risk of stroke (1.94/100 person-years) with patients with 1 risk score (2.06/100 person years), and the investigators suggest that lowering the current age threshold (age, ≥65 years) in the CHA2DS2-VASc score to age ≥55 years might be appropriate among Asian patients with AF.18) A modified CHA2DS2-VASc score which lowered the age threshold from 65 to 50 years has been proposed, and may be able to identify more Asian AF patients who may have benefits from OAC use.19) More studies are necessary to investigate the optimal age threshold for the use of OACs, especially NOACs, for Asian AF patients.
Female sex
The 2018 AF guidelines of Australia/New Zealand recommend the CHA2DS2-VA score—the sexless CHA2DS2-VASc score—for predicting stroke risk in AF.20) Although the CHA2DS2-VA score could be used for decision making about OAC use for AF patients, it could underestimate the stroke risk of AF females. In the Danish nationwide study, AF females with no other risk factors (CHA2DS2-VASc score of 1) have a similar stroke risk to AF males with a CHA2DS2-VASc score of 0, while women with AF consistently have significantly higher stroke risks than men in the presence of >1 non-sex stroke risk factor.21) Therefore, female sex should be regarded as a stroke risk modifier rather than a risk factor, and the inclusion of female sex in the CHA2DS2-VASc scheme would estimate the stroke risk of AF females more accurately.
BLEEDING RISK ASSESSMENT
The suggestions of the bleeding scheme used for bleeding risk assessment are listed in Table 1.5)6)7)8) Most guidelines recommend the use of the HAS-BLED score for bleeding risk assessment, while the ACC/AHA did not propose any specific bleeding risk scheme.9) HAS-BLED score has been well-validated in Asian AF patients which could predict the occurrences of major bleeding or ICH more accurately than other bleeding prediction schemes.22) A major concern about the use of bleeding schemes is that physicians may inaccurately regard a high bleeding risk score as a reason to withhold OACs. The 2020 ESC guidelines clearly stated that the HAS-BLED score should be considered to help address modifiable bleeding risk factors, and to identify patients at high risk of bleeding (HAS-BLED score >3) for early and more frequent clinical review and follow-up (class IIa recommendation)”, rather than being used to guide treatment decisions to use OAC or not (class III recommendation).8) Actually, in the mobile AF application (mAFA-II) randomized trial, HAS-BLED score was monitored prospectively using mAFA, and calculated as 30 days, days 31–60, days 61–180, and days 181–365.23) Among 1077 (60%) patients who had 4 bleeding risk assessments, incident bleeding events decreased significantly from days 1–30 to days 181–365 (1.2% to 0.2%, respectively, p<0.001), while the total OAC usage increased from 63.4% to 70.2% (p trend<0.001).23) A recent study from Taiwan also showed that for AF patients with a low bleeding risk (HAS-BLED score 0–2) who received OACs, the continuations of OACs once their HAS-BLED scores increased to >3 were associated with a lower risk of ischemic stroke (HR, 0.60) and all-cause mortality (HR, 0.88).24) All these data support the concept that a high HAS-BLED score itselft should not be the sole reason to withhold OACs for stroke prevention.
REGULAR RE-ASSESSMENT OF STROKE RISK
When assessing the stroke risk of AF patients, it is important to recognize the dynamic nature of stroke risk of AF patients.25)26)27)28) Among newly-diagnosed AF patients initially with a CHA2DS2-VASc score of 0 (males) or 1 (females) who were not indicated for OACs, around 16% of them would have a CHA2DS2-VASc score >1 (males) or >2(females) at 1 year,29) and the use of OACs once their CHA2DS2-VASc scores increased was associated with a better net clinical outcome.28) The follow-up CHA2DS2-VASc scores or its changes (delta CHA2DS2-VASc scores) were more accurate than the baseline scores in the prediction of ischemic stroke.26) Until now, there were no high-quality prospective studies investigating the optimal frequency of stroke risk re-assessment and subsequent changes of stroke prevention strategy. The only available data were reported from Taiwan AF cohort showing that for AF patients who acquired new stroke risk factors, 80% of them would acquire these co-morbidities after 4.2 months of AF diagnosis. The duration from the acquirement of incident co-morbidities to the occurrence of ischemic stroke was longer than 4.4 months for 90% of the patients.28) Therefore, 3–4 months may be a reasonable timing interval at which stroke risk should be reassessed so that OACs could be prescribed in a timely manner for stroke prevention.28) However, the optimal and reasonable frequency of stroke risk re-assessement should also incorporate compliance of patients and cost-benefit ratio which would vary widely in diverse healthy care systems. Several key points about the use of CHA2DS2-VASc and HAS-BLED scores for stroke and bleeding risk assessments are listed in Figure 1.
Figure 1
Key points about the use of CHA2DS2-VASc and HAS-BLED scores for stroke and bleeding risk assessments.
ACCP = American College of Chest Physicians; AF = atrial fibrillation; APHRS = Asia Pacific Heart Rhythm Society; CAD = coronary artery disease; ESC = European Society of Cardiology; HCM = hypertrophic cardiomyopathy; LV = left ventricular; OAC = oral anticoagulant; PAD = peripheral artery disease.
NON-VITAMIN K ANTAGONIST ORAL ANTICOAGULANTS FOR ATRIAL FIBRILLATION PATIENTS WITH SINGLE ONE STROKE RISK FACTOR BEYOND GENDER
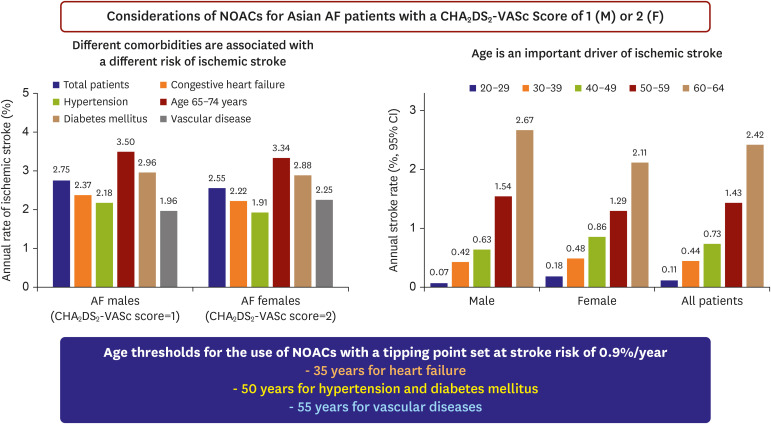
In most important international guidelines, OACs were not recommended for patients with a CHA2DS2-VASc score of 0 (males) or 1 (females), and were recommended/indicated for those with a CHA2DS2-VASc score >2 (males) or >3 (females).9) However, the recommendations about use of OACs for AF patients with single one stroke risk factor beyond gender (CHA2DS2-VASc score 1 for males and 2 for females) are different between 2020 ESC (class IIa recommendation) and 2019 ACC/AHA (class IIb recommendation) guidelines. For Asian AF patients, a more personalized approach may be helpful since these AF patients were not the homogenous population regarding their stroke risks.30) There are 2 important points should be considered before determining the use of NOACs for Asian AF patients with a CHA2DS2-VASc score 1 (males) or 2 (females). First, which kind of the non-sex stroke risk factor contributes to the CHA2DS2-VASc score and second, how old is the patient. It is well recognized that different risk factors were associated with different stroke risks,31)32) with age being as a very important determinant.17)33) Therefore, different age thresholds should be considered for the use of NOACs for patients with different comorbidities. Based on the recent report, the proposed age thresholds were as follows: age 35 years for HF, 50 years for hypertension or diabetes, and 55 years for vascular disease,30)33) which have been also mentioned in 2020 ESC guideines.8) The considerations about the use of NOACs for Asian AF patients with single one stroke risk factor beyond gender are summarized in Figure 2. These proposed age thresholds should be validated and tested in further studies from various dataset.
BIOMARKERS, IMAGING TOOLS AND ARTIFICIAL INTELLIGENCE FOR STROKE RISK PREDICTION IN ATRIAL FIBRILLATION
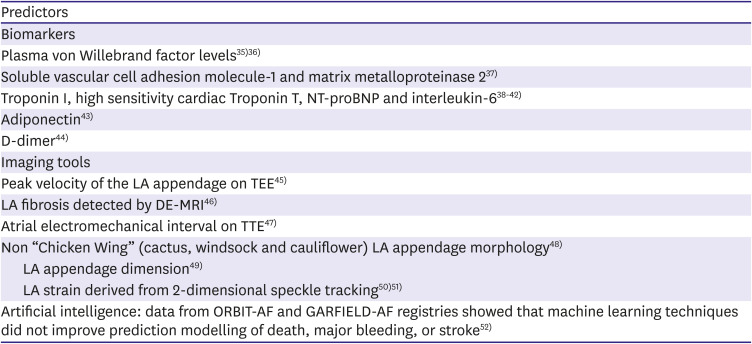
Other than the components of the CHA2DS2-VASc scheme, some biomarkers and several parameters derived from imaging tools which were reported to be associated with stroke events in AF patients are summarized in Table 2.34)35)36)37)38)39)40)41)42)43)44)45)46)47)48)49)50)51)52) A biomarker-based stroke risk score, the ABC (age, biomarkers [high-sensitivity troponin and N-terminal pro B-type natriuretic peptide; NT-proBNP], and clinical history of prior stroke/transient ischemic attack) score, has been developed to predict stroke or SE in 14,701 anticoagulated AF patients enrolled in ARISTOTLE trial, and was externally validated in 1,400 participants with AF or atrial flutter (689 on OACs) in the STABILITY trial.40) The ABC-stroke score yielded higher c-indices than the CHA2DS2-VASc score in both the derivation cohort (0.68 vs. 0.62, p<0.001) and the external validation cohort (0.66 vs. 0.58, p<0.001).40) The ABC-stroke score were subsequently validated in patients enrolled in RE-LY and ENGAGE AF-TIMI 48 trials.41)42) However, the follow-up duration was often short in the trial cohort; whether the baseline ABC-stroke score could predict long-term outcomes of patients was not clear. In a study from Spain analyzing 1,125 AF patients who were stable on VKAs and followed-up for a median of 6.5 years, the ABC-stroke score does not offer significantly better predictive performance compared with the CHA2DS2-VASc score.53) Furthermore, levels of biomarkers, such as NT-proBNP, could change significantly over time. In the nested prospective biomarker study from ENGAGE AF-TIMI 48 trial which included 6308 patients, levels of high-sensitivity troponin T (hsTnT) and NT-proBNP were measured at baseline and 12 months.54) The results demonstrated that hsTnT was dynamic in 46.9% (≥2 ng/L change) and NT-proBNP in 51.9% (≥200 pg/mL change) during 12 months, and re-assessment of ABC-stroke risk score at 12 months accurately reclassified a significant proportion of patients compared with their baseline risk (net reclassification improvement 0.50; 95% confidence interval, 0.36–0.65).54) These findings demonstrated that how biomarkers were dynamic, just like the changes of CHA2DS2-VASc scores, and should also be re-assessed. Given the costs of the measurements of biomarkers and the uncertainty of the intervals at which biomarkers should be rechecked, the CHA2DS2-VASc score should still be the clinically preferred tool for stroke risk assessment unless further studies could clearly prove that ABC-stroke score-guided OAC treatments are better than CHA2DS2-VASc score-based approach.
Table 2
Summary of reported biomarkers, imaging tools and artificial intelligence in the prediction of stroke in AF
| Predictors | |
|---|---|
| Biomarkers | |
| Plasma von Willebrand factor levels35)36) | |
| Soluble vascular cell adhesion molecule-1 and matrix metalloproteinase 237) | |
| Troponin I, high sensitivity cardiac Troponin T, NT-proBNP and interleukin-638)39)40)41)42) | |
| Adiponectin43) | |
| D-dimer44) | |
| Imaging tools | |
| Peak velocity of the LA appendage on TEE45) | |
| LA fibrosis detected by DE-MRI46) | |
| Atrial electromechanical interval on TTE47) | |
| Non “Chicken Wing” (cactus, windsock and cauliflower) LA appendage morphology48) | |
| LA appendage dimension49) | |
| LA strain derived from 2-dimensional speckle tracking50)51) | |
| Artificial intelligence: data from ORBIT-AF and GARFIELD-AF registries showed that machine learning techniques did not improve prediction modelling of death, major bleeding, or stroke52) | |
The table was modified from the table by Chao et al.34)
AF = atrial fibrillation; DE-MRI = delayed-enhanced magnetic resonance imaging; LA = left atrium; NT-proBNP = N-terminal pro-B-type natriuretic peptide; TEE = transesophageal echocardiography; TTE = transthoracic echocardiography.
Artificial intelligence (AI) is developing rapidly and may improve stroke risk stratification in AF. However, in an analysis of the ORBIT-AF and GARFIELD-AF registries including 74,792 AF patients, machine learning techniques did not improve prediction modelling of death, major bleeding, or stroke.52) More efforts are necessary to see whether more advanced AI models could improve risk prediction of AF patients and change clinical practice.
THE FUTURE: ATRIAL FIBRILLATION DURATION AND LEFT ATRIAL FUNCTION
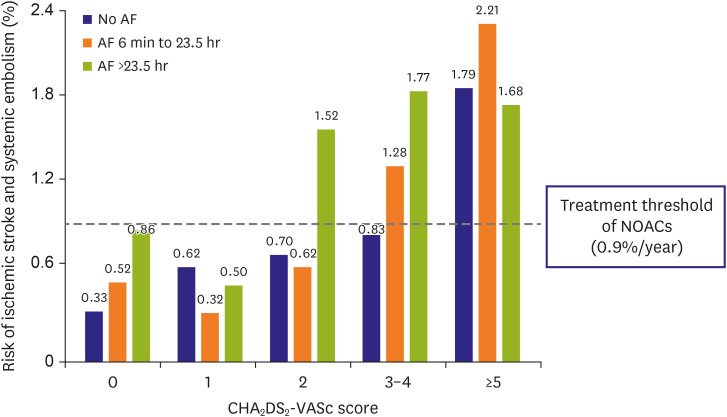
The personalized and precision evaluation of stroke risk of each AF individuals is the future of stroke prevention in AF, and the AF duration and left atrial function may play an important role. Although the current stroke risk stratification scheme did not take the duration of AF into consideration, more and more data suggesting that the stroke risk may be a function of AF duration and clinical comorbidities. In a recent study which included 21,768 non-anticoagulated patients with cardiovascular implantable electronic devices, both increasing AF duration (p<0.001) and increasing CHA2DS2-VASc score (p<0.001) were signifcantly associated with annualized risk of ischemic stroke and SE (SSE).55) When patients were categorized into 3 groups according to the maximum daily AF duration (no AF, 6 minutes to 23.5 hours, and >23.5 hours), a interaction between AF duration and CHA2DS2-VASc scores were observed, as shown in Figure 3.55) For patients with a low CHA2DS2-VASc score (0 or 1), the risk of SSE was lower than 0.9%/year even for those with a maximum AF duration longer than 23.5 hours, and therefore, NOACs were generally not necessary. On the contrary, for patients with a high CHA2DS2-VASc score (>5), NOACs should be considered even their AF burdens were low. Most importantly, information about AF duration may be able to further stratify patients with a middle-range CHA2DS2-VASc score (2 or 3–4) into different groups with a SSE rate higher or lower than 0.9%/year. Further studies should be performed to understand whether the incorporations of AF duration into the CHA2DS2-VASc score could really improve stroke risk assessment.
Figure 3
Interactions between AF duration and CHA2DS2-VASc score regarding risk of ischemic stroke and systemic embolism. Data used in the figure were adopted form the papers by Kaplan et al.55)
AF = atrial fibrillation; NOACs = non-vitamin K antagonist oral anticoagulants.
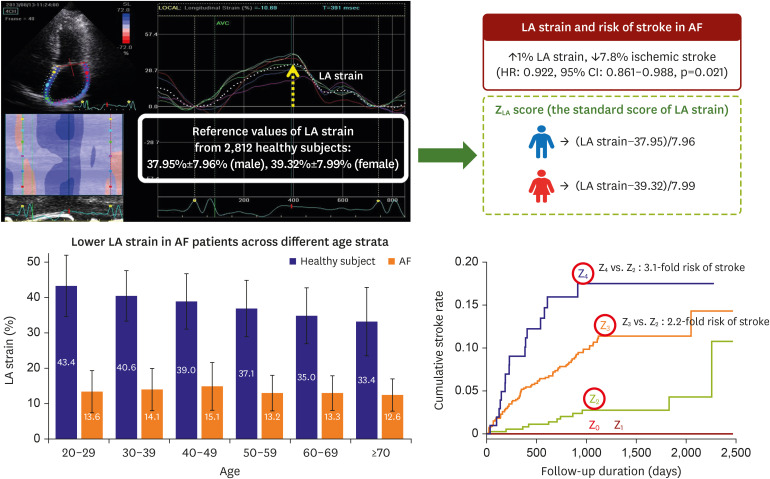
Atrial cardiomyopathy was defined as “any complex of structural, architectural, contractile or electrophysiological changes affecting the atria with the potential to produce clinically-relevant manifestations”,56)57) and left atrium (LA) could be regarded as a “target organ” which would suffer from damages due to systemic diseases (like hypertension, HF, and diabetes). Peak atrial longitudinal strain derived from 2-dimensional speckle tracking echo (LA strain) is a more sensitive marker to detect early functional remodelling than overt structural change, such as LA dilatation. Several studies regarding the potential role of LA strain in stroke risk stratifications have been published and summarized in Figure 4.50)51)58) A lower LA strain is commonly observed in AF patients irrespective of different age strata compared to normal subjects,58) and independently associated with an increasec risk of ischemic stroke (7.8% lower risk of stroke per 1% increase in LA strain).50) The degree of decrease of each AF individual's LA strain from reference values can be applied in a stratified manner as standard score for organized risk stratification.51) In the previous study performed by Liao et al.,51) AF patients with a mean LA strain lower than reference values (mean values of LA strain of healthy subjects) for more than 3 standard deviations were associated with a more than 2-fold higher risk of ischemic stroke compared to those whose LA strain was lower for only 2–3 standard deviations. Besides, the consecutive 3-beat averaged value of LA strain is a feasible and reproducible method to overcome the irregular cardiac cycle of AF and correlated well with the index-beat method and 10-second average method.50) Further integration of LA strain with current risk stratification schemes might be a potential manner for prognostication in the era of individualized precision medicine.
CONCLUSION
Stroke and bleeding risks of AF patients should be assessed using CHA2DS2-VASc and HAS-BLED scores, respectively, and should be regularly re-assessed. The AF duration and left atrial function may play an important role for personalized evaluation of individual stroke risk while more studies are necessary.
 XML Download
XML Download