

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Retinal vein occlusion (RVO), differentiated into central RVO (CRVO) and branch RVO (BRVO), is one of the most common and sight-threatening retinal vascular diseases.12345 The pathogenesis of RVO is not yet clear; multifactorial causes are known to be involved. The compression of the retinal vein by the atherosclerotic retinal artery is a well-known etiological process involved in the development of RVO. The rigid retinal artery, caused by hypertensive atherosclerosis, compresses the retinal vein at the level of the lamina cribrosa (CRVO) or the arteriovenous crossing site (BRVO); this can cause hemodynamic alterations, and subsequent thrombus formation.6789101112 In addition, hematologic abnormalities, such as inflammatory diseases and thrombophilia, may also contribute to the development of RVO.61013
End-stage renal disease (ESRD), requiring dialysis due to irreversible decline in renal function, is a significant global public health problem. The prevalence of ESRD is increasing in developed and developing countries; this is due to the increased incidence of diabetes mellitus (DM) and the aging population.141516 In South Korea, the increasing proportion of elderly and DM patients has led to a rapid increase in the number of patients with ESRD.17 RVO and ESRD are both microvascular diseases related to arteriolar narrowing, hypercoagulation, and pro-inflammatory mediators.918 Further, the well-known risk factors for RVO (e.g., hypertension, DM, hyperlipidemia, congestive heart failure, and coronary artery disease) can be risk factors for ESRD.192021 Therefore, the incidence of RVO might be increased in patients who have undergone dialysis.
Few population-based studies have reported the association between patients undergoing dialysis for ESRD and the incidence of RVO.222324252627 However, a large-scale nationwide long-term cohort study of the Korean population has not been implemented. As hemodynamic changes might be different according to the method of dialysis,2829 the RVO incidence could be different according to the method used (hemodialysis [HD] vs. peritoneal dialysis [PD]). There were also no population-based cohort studies evaluating the incidence of RVO according to the method of dialysis. Therefore, we examined the incidence and risk of RVO in a large population of patients undergoing dialysis using Korean National Health Insurance Service (KNHIS) data and the propensity score matched cohort study design. Further, we evaluated the incidence of RVO according to the method of dialysis.
METHODS
Database
We used data from the KNHIS (a compulsory health insurance plan, covering over 97% of the Korean population). The database contains demographic information, dates of treatments, principal diagnoses, comorbidities (using the International Classification of Disease 10th revision [ICD-10]), prescriptions, and medical or surgical procedures. It also includes records of reimbursements to all Korean medical institutions; we used this information to create our dialysis cohorts. The data for the control group were obtained from the KNHIS National Sample Cohort (KNHIS-NSC) 2002–2013 database. This database was provided by KNHIS in 2015 for research purposes; it includes data from approximately 1,000,000 randomly selected South Koreans, extracted by sampling in 2002 (2.2% of the total Korean population of 46 million) and resampled until 2013 by KNHIS. Thus, this longitudinal database can represent the South Korean population.
Study population
We included ESRD patients in the dialysis cohort who began dialysis between 2004 and 2013, without being diagnosed with RVO, based on their visit date. Patients who underwent dialysis were identified using claims for any procedures or materials associated with HD or PD. This was based on the Korean electronic interchange codes (treatment codes: O7020 for HD, O7061 for PD); patients were considered eligible if they had received dialysis for more than 3 months. We excluded cases diagnosed with ESRD who had used medical services during the first year of the study (2003), based on the assumption that they already had chronic ESRD on dialysis.
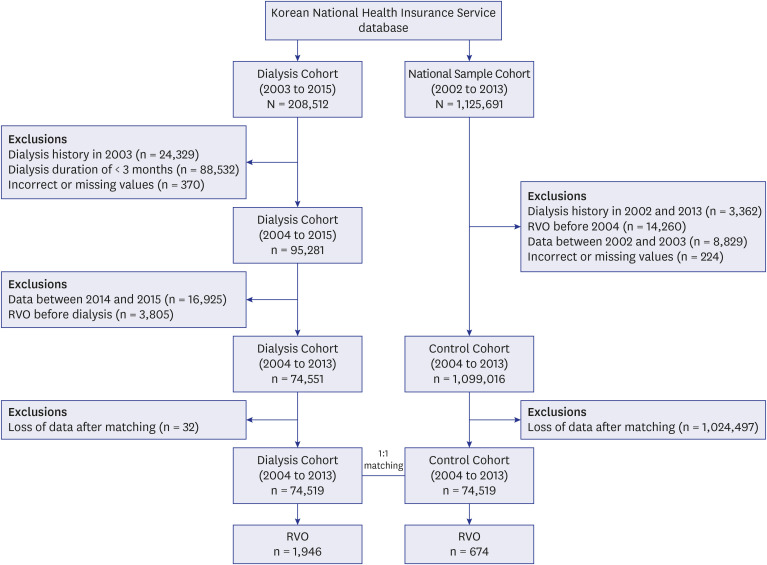
For each ESRD patient, one propensity score matched control without ESRD was selected from the KNHIS-NSC database to create the control cohort. Propensity score matching was performed using the nearest neighbor method to identify similar individuals in the dialysis and control cohorts. The propensity scores were estimated using logistic regression for each patient based on age, sex, income level, and comorbidities. We identified the incidence of RVO from 2004 to 2013 using the Korean Classification of Disease (6th Edition), a modified version of the ICD-10 adapted for the Korean health care system (diagnostic code: H34.8). We excluded patients diagnosed with RVO before beginning dialysis from the dialysis cohort, and dialysis patients, patients who had RVO before 2004 from the control cohort. Renal transplantation patients were excluded from both cohorts (Fig. 1).
Co-variables
Factors that might influence the incidence of RVO, such as age, sex and comorbidities (e.g., hypertension, DM, hyperlipidemia, congestive heart failure, stroke, myocardial infarction, and atrial fibrillation) were used as independent variables in univariable and multivariable Cox regression analysis. Comorbidities were identified based on the ICD-10 codes as DM (E10–E14), hypertension (I10–I15), hyperlipidemia (E78), congestive heart disease (I50), stroke (I60–I64), myocardial infarction (I21–I22), and atrial fibrillation (I48). Data associated with co-variables were available for the dialysis and control cohorts, using the KNHIS database.
Statistical analysis
Proportional differences in the demographic characteristics and comorbidities between the dialysis and control cohorts were compared using the Wald χ2 test. The incidence of RVO was defined as the number of newly diagnosed RVO cases per 100,000 person-years (PY). The incidence rate ratio (IRR) of ESRD, relative to the controls, was calculated with a 95% confidence interval (CI). We applied a multivariable Cox proportional hazards model to all independent variables after combining the two cohorts to determine the dialysis-related risk of developing RVO; this was reported as a hazard ratio (HR) with a 95% CI. The follow-up period started on the first date of dialysis for the ESRD patients and on random visit dates for the controls that corresponded to the calendar year of the start of dialysis for their matched ESRD patients. The follow-up period ended at the first date of RVO diagnosis or the date of last follow-up visit. Cumulative RVO incidence curves were generated using the Kaplan-Meier method. Differences in the cumulative-incidence rate curves were analyzed using the log-rank test. We divided the ESRD patients into two subgroups, HD and PD, to evaluate whether dialysis modalities would influence the incidence of RVO. SAS software (version 9.4; SAS Institute, Inc., Cary, NC, USA) and R software (version 3.4.3; R Foundation for Statistical Computing, Vienna, Austria) were used in this study.
Ethics statement
This retrospective, nationwide, propensity score matched cohort study was approved by the institutional review board of the Chungbuk National University Hospital and the requirement for informed consent was waived (2019-04-009). All patient records from the KNHIS have been anonymized to ensure patient confidentiality.
RESULTS
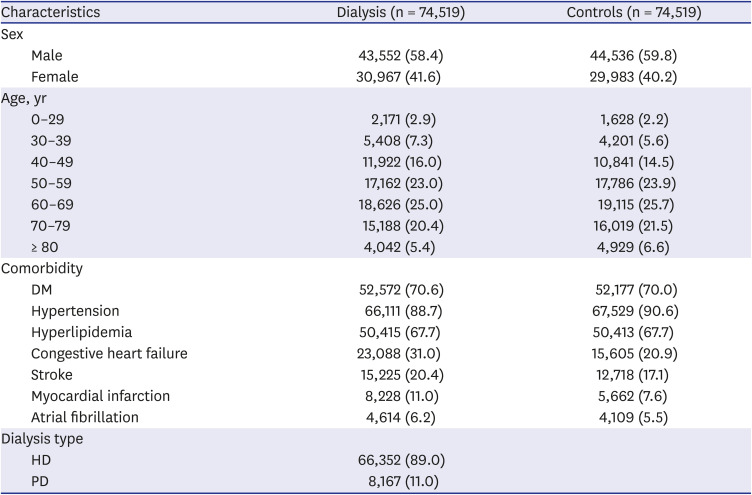
Between 2004 and 2013, we selected 74,551 ESRD patients for the dialysis cohort and a matching number of individuals for the control cohort, after excluding ineligible subjects. The mean follow-up periods for the ESRD patients on dialysis and the controls were 3.59 ± 2.70 and 4.77 ± 2.80 years, respectively. Table 1 summarizes the demographic characteristics and comorbidities of the study population. Comparable distributions of age, sex, and comorbidities were obtained due to individual matching between the dialysis and control cohorts.
Table 1
Demographic characteristics and comorbidities in the dialysis and control groups
Incidence of RVO in patients in the dialysis cohort
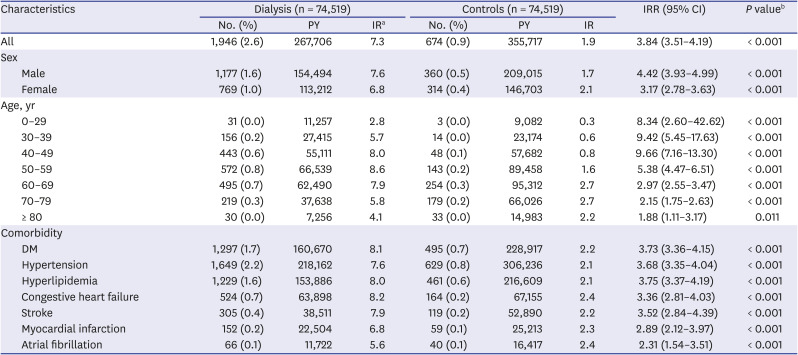
During the 10-year study period, 1,946 patients in the dialysis cohort (2.6%) and 674 patients in the control cohort (0.9%) developed RVO (Table 2). There was a significant difference in the incidence of RVO between the 2 groups (patients on dialysis: 7.3/1,000 PY; control: 1.9/1,000 PY; P < 0.001). The IRR between the dialysis and control cohorts was statistically significant (3.84, 95% CI, 3.51–4.19, P < 0.001; Table 2). In subgroup analysis related to sex, the IRR of RVO in the dialysis cohort increased for both males and females, compared to the control cohort. In the age-related subgroup analysis, ESRD patients on dialysis who were 40 to 49 years old had the highest IRR (9.66, 95% CI, 7.16–13.30; P < 0.001), followed by the 30–39 age group (9.42, 95% CI, 5.45–17.63, P < 0.001), and the 0–29 age group (8.34, 95% CI, 2.60–42.62, P < 0.001). With other comorbidities, the dialysis cohort had a significantly increased IRR of RVO than the control cohort (Table 2).
Table 2
Characteristics of RVO cases in the dialysis and control groups
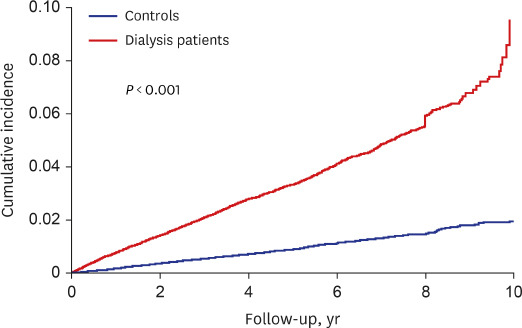
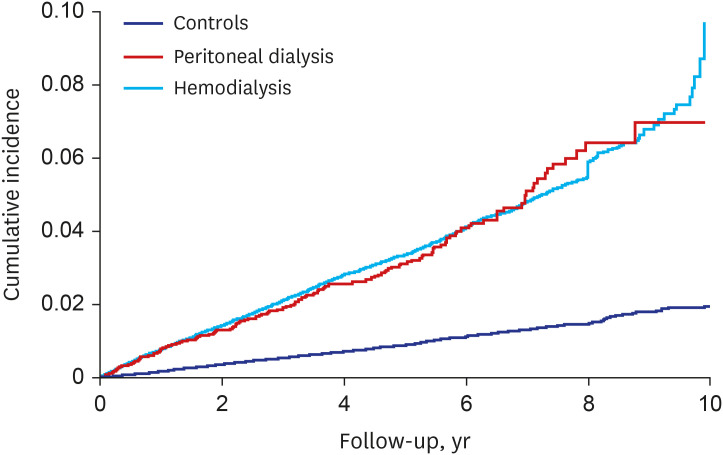
The Kaplan-Meier survival analysis revealed that the cumulative-incidence of RVO was significantly higher in the dialysis cohort than the control cohort (P < 0.001; log-rank test; Fig. 2). For the subgroup analyses regarding dialysis modalities, similar results were obtained for both HDs and PD (both P < 0.001; log-rank test; Fig. 3). Between the HDs and PD subgroups, the risks of RVO were not significantly different (P = 0.550; log-rank test). Regardless of the method of dialysis, the RVO incidence rapidly increased with an increase in the duration of dialysis.
Fig. 2
Kaplan-Meier curve of the cumulative-incidence of RVO in end-stage renal disease patients undergoing dialysis and controls, during the follow-up period. The cumulative-incidence of RVO was significantly higher in the dialysis cohort than in the control cohort (P < 0.001; log-rank test), and the cumulative-incidence of RVO in the dialysis cohort increased rapidly after 8 years of follow-up.
RVO = retinal vein occlusion.
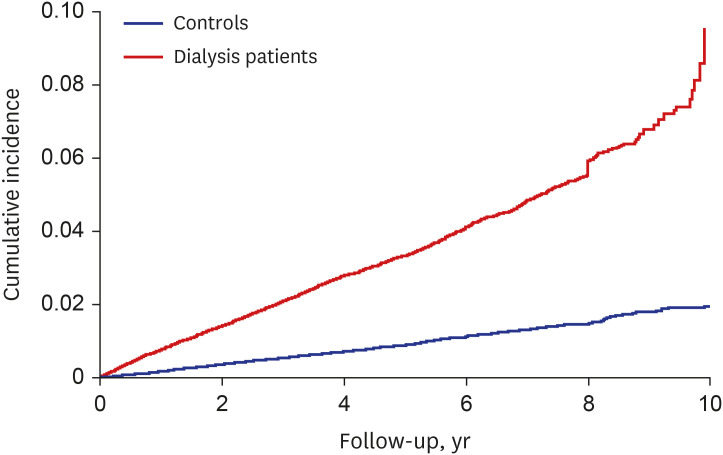
Fig. 3
Kaplan-Meier curve of cumulative-incidence of RVO in end-stage renal disease patients undergoing dialysis and controls, during the follow-up period, according to the type of dialysis. Both hemodialysis and peritoneal dialysis subgroups showed a higher cumulative-incidence of RVO than the control cohort (both P < 0.001; log-rank test). Regardless of the method of dialysis, the incidence of RVO rapidly increased with an increase in the duration of dialysis.
RVO = retinal vein occlusion.
HRs for RVO
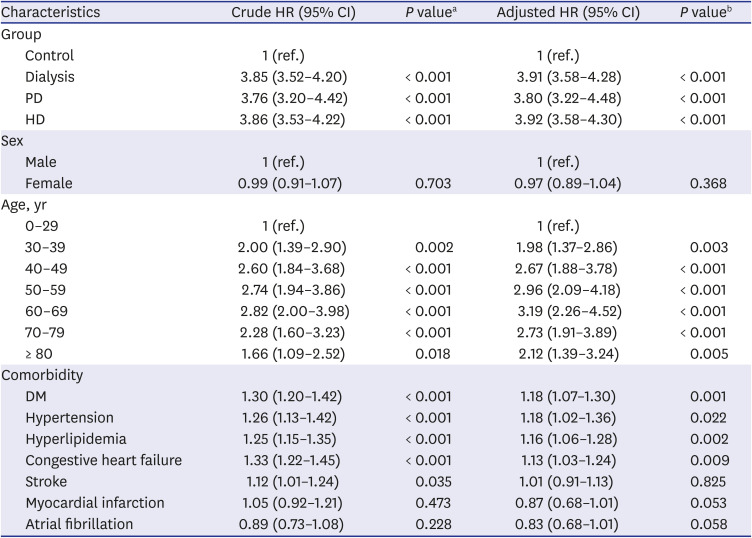
Table 3 provides the crude and adjusted HRs for RVO development, according to the univariable and multivariable Cox regression analyses. After adjusting for sex, age, and comorbidities, ESRD patients on dialysis had an independently elevated risk of RVO (adjusted HR, 3.91, 95% CI, 3.58–4.28). Elevated risks of RVO were independently associated with HD (adjusted HR, 3.92, 95% CI, 3.58–4.30) and PD (adjusted HR, 3.80, 95% CI, 3.22–4.48). In all age groups above 30, the association with RVO was higher than in the 0–29 age group (Table 3). Among the comorbidities, DM (adjusted HR, 1.18), hypertension (adjusted HR, 1.18), hyperlipidemia (adjusted HR, 1.16), and congestive heart failure (adjusted HR, 1.13) showed significant associations with RVO. However, stroke, myocardial infarction, atrial fibrillation were not independent risk factors for RVO.
Table 3
Univariable and multivariable Cox regression analyses of risk factors for RVO
DISCUSSION
We previously reported several nationwide cohort studies, and we found that dialysis patients exhibited a higher incidence of malignancy than controls, also, patients receiving dialysis for ESRD had an elevated risk of active TB.3031 This nationwide cohort study investigated the association between RVO incidence and dialysis. The primary finding of this study was that the incidence rate of RVO in ESRD patients on dialysis was 3.84 times higher than in controls. Additionally, the relative risk of RVO for dialysis patients with ESRD was 3.91 times higher in HD and PD dialysis groups after adjusting for age, sex, and other comorbidities. The incidence of RVO was not different according to the method of dialysis (HD vs. PD). Regardless of the method, the incidence rate of RVO rapidly increased as the duration of dialysis increased.
In East Asia, Korea and Taiwan are the only countries where a nationwide database has been established. Few studies about the association between ESRD and RVO using these databases have been reported in Korea and Taiwan.232427 Chang et al.23 investigated the risk of RVO following ESRD in Taiwan. They included 92,774 patients in the ESRD group, reporting an adjusted HR of 3.05 for RVO development in ESRD patients; this is similar to the results of the present study. However, they did not analyze the incidence of RVO according to the method of dialysis without a washout period and the study duration was relatively short. Additionally, Lee et al.27 reported the association between ESRD and subsequent RVO development in Korean patients. This study demonstrated that the incidence of RVO was higher in the ESRD group than in the comparison group (3.95% vs. 2.17%); the ESRD patients produced an adjusted HR for RVO development of 2.12. However, that study was not a long-term cohort study with dialysis patients. They included subjects using chronic kidney disease diagnosis codes (ICD-10, N18), not dialysis treatment codes (O7020 for HD, O7061 for PD). Further, the included number of patients with ESRD was relatively small (n = 988) because the database contained data from 1,025,340 randomly selected patients extracted by sampling from 2002 only. In contrast to previous studies, our study is based on a nationwide, long-term, population-based dataset, including a large sample of patients with ESRD on dialysis (n = 74,519) from a population of 48-million over a long period. Therefore, this current study has high statistical power, increased precision in risk appraisal, and could represent the entire South Korean population accurately.
In this population-based, long-term study, the incidence rate of RVO in ESRD patients on dialysis was significantly increased, compared with the control group. This increased incidence of RVO in dialysis patients could be attributed to several reasons. First of all, RVO and ESRD have a common pathogenic mechanism, as the inner retina and glomerular filtration barrier have a homologous developmental pathway32 and have similar structural features.33 Arteriosclerosis is a major factor; many studies have reported an association between retinal microvascular abnormalities and renal dysfunction. Further, retinal arteriolar narrowing and arteriovenous nicking result from arteriosclerosis; these are risk factors for RVO and are frequently observed in ESRD patients.3435 Therefore, RVO incidence could be increased in ESRD patients.
In addition, inflammation may also contribute to the development of RVO. Elevated pro-inflammatory mediators and the reduction of anti-inflammatory cytokines can play a role in the pathogenesis and propagation of RVO.613 Chronic inflammation is highly prevalent in dialysis patients. Dialysis-specific factors (e.g., central venous or PD catheters) can induce the continuous non-specific stimulation of immune cells (e.g., monocytes). In addition, chronic bio-incompatible reactions to the dialysis membrane, back filtration of bacterial lipopolysaccharide particles, and dialysate or water contamination with endotoxin are mechanisms that can trigger inflammatory reactions to dialysis.36
Another reason why dialysis can increase RVO incidence is related to oxidative stress (OS). OS appears in ESRD, and is worsened by HD due to the accumulation of oxidative products, and the loss of antioxidant molecules.37 Additionally, OS is also accelerated by PD due to the composition of the PD solutions.38 OS can increase chronic inflammation and atherogenesis in the vessel; this may contribute to the development of RVO. Therefore, ESRD patients undergoing dialysis are at a higher risk of RVO due to the aforementioned reasons. Evidently, dialysis patients should undergo regular retinal examinations to identify RVO or other retinal diseases.
In the current study, the incidence rate of RVO increased as the duration of dialysis increased, regardless of the method of dialysis. In the Kaplan-Meier plot, the cumulative-incidence of RVO in the dialysis cohort increased rapidly after 8 years of follow-up (Fig. 2). These results suggest that long-term dialysis may rapidly increase the incidence of RVO in patients on dialysis. This finding had not been observed in previous national-wide population-based studies.232427 Unlike previous studies, we have been able to find this rapid increase of RVO incidence because we have analyzed the incidence over a long period of time. Considering this rapid increase in the incidence of RVO with an increase of dialysis duration, the necessity of regular retinal examinations of dialysis patients is emphasized. Further, studies to determine whether other systemic or retinal vascular diseases can be rapidly increased as dialysis period increases could be needed.
In this study, several well-known comorbidities (e.g., DM, hypertension, hyperlipidemia, and congestive heart failure) were found to be significantly associated with the risk of RVO. Many previous studies have reported that hypertension is a risk factor for RVO,1223242739 however, there have been discrepancies between studies reporting if DM, hyperlipidemia, and congestive heart failure are risk factors. Chang et al.23 demonstrated that DM was a protective factor. Differences in demographics (e.g., sex ratio, population, or race) may explain the disparities between results from previous studies and the current study. In contrast, we expected stroke, myocardial infarction, and atrial fibrillation to be related to the development of RVO; however, they were not significantly associated with the risk of RVO. A possible explanation is that patients with these comorbidities may be prescribed medication (e.g., anticoagulants or blood circulation-improving agents) that could prevent the development of RVO.
A notable strength of our study is that this study is based on a nationwide, population-based dataset, using a large sample to compose the dialysis cohort; this elevates the power of statistics and allows better generalizability. Furthermore, both cohorts were designed by an epidemiologist and the dialysis cohort, in particular, was created using patients with a nephrologist-confirmed diagnosis of ESRD. To our knowledge, it is the first study to observe a rapid increase of RVO incidence in patients on dialysis as a result of an increase in the duration of dialysis. However, this study had the following limitations: 1) From this study, it is difficult to know whether ESRD itself or the hemodynamic changes associated with dialysis increased the incidence of RVO. Considering the rapid increase of the incidence of RVO as the duration of dialysis increased, dialysis alone could affect the development of RVO. 2) We used data that was based on diagnostic codes and insurance claims; therefore, disease misclassification may have occurred. Additionally, we could not include asymptomatic patients, bilateral or recurrent cases. These factors may have led to the underestimation of the incidence of RVO in Korea. Furthermore, the frequency or duration of delayed diagnoses cannot be determined; this may have influenced cumulative-incidence. 3) The insurance claims data did not include information on laboratory data. Therefore, it was not known whether the dialysis patients had compliance with dialysis or if uremia was controlled. This may have affected the reliability of the dialysis cohort. 4) Since the diagnostic codes for CRVO and BRVO are not separated, we could not classify the RVO cases, assessing them together as a single-disease group. Despite these limitations, this study uniquely analyzed the RVO incidence in patients on dialysis using a national-wide, population-based data set and the incidence of RVO, according to the method of dialysis.
In conclusion, the present study revealed epidemiological evidence that receiving dialysis for ESRD was associated with an increased risk of developing RVO. We also found a rapid increase in the incidence of RVO with a longer dialysis period. There was no difference in the incidence of RVO according to the type of dialysis. These results suggest that regular retinal examinations are a necessity for ESRD patients on dialysis to identify RVO and other retinal diseases. Further, more active efforts to control systemic risk factors should be taken to prevent the development of RVO in the Korean population.
 XML Download
XML Download