

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
As coronavirus disease 2019 (COVID-19) increases in prevalence, the importance of vaccination has increased. Vaccination is essential to achieve herd immunity, and to achieve herd immunity, it is known that at least 70% of the population must be vaccinated.12 However, after vaccination, vaccine adverse events can follow, and these events can cause “vaccine hesitancy,” which is directly related to the vaccination rate.3 If inappropriate information about the adverse events of the vaccine trigger fear of the vaccine, the progress toward herd immunity can be hindered.4 To reduce vaccine hesitancy, we need to detect the possibility of an adverse effect (which is called a signal) as soon as possible by post-marketing surveillance and provide objective and reliable results to the public after prompt investigation of the detected signals.5
Post-marketing surveillance consists of two types: passive and active. Passive surveillance is based on spontaneous reporting systems,6 which are reporting systems from doctors or patients. Currently, most surveillance relies on passive surveillance,7 but this approach has several limitations such as under-reporting and reporting bias. South Korea started using passive surveillance systems in 1994, and the Communicable Disease Control Act has required healthcare professionals to report vaccine adverse events since 2001.8 In contrast, active surveillance actively searches for the adverse events of drugs or vaccines by monitoring existing data such as electronic health records910 or administrative claims data.1112 Most importantly, an active surveillance system can detect adverse events more rapidly than a passive system and it helps inform the public about the safety of vaccines.9 In South Korea, however, an active surveillance system for capturing adverse event information has not yet been established.7 In a pandemic situation like the current one, catching adverse events early after a large-scale vaccination is important, and a well-developed active surveillance system can form the basis of vaccine safety monitoring.13
Awareness of the importance of active surveillance has to the development of several algorithms on large databases,14 but these approaches still have limitations. Azadeh and Gonzalez conducted an adverse event monitoring study by analyzing the content of social media data mentioning adverse events using the association rule.15 Botsis et al.16 used adverse event reports from the Vaccine Adverse Event Reporting System to develop a text mining model that distinguishes between positive and negative reports of anaphylaxis after the H1N1 vaccination. However, adverse event studies based on unstructured text analysis have the disadvantages of being time consuming and labor intensive. To investigate each adverse event, the text must be annotated, and the supervision of a domain expert is essential.17 Therefore, this approach is not suitable in situations such as COVID-19 vaccination, which requires prompt screening of adverse event signals while overwhelming amounts of new data are generated daily.
Disproportionality analysis, one of most popularly used pre-existing data mining approaches, can be easily applied to big databases retrospectively because of its simplicity,18 but it may not consider covariates.19 The TreeScan algorithm can make adjustments to covariates like sex, age, and health plan, but it requires a predefined hierarchical tree structure for the adverse events; the International Classification of Diseases, Ninth Revision, Clinical Modification coding system was used in the previous study.20 The process that cuts the branches of the tree structure where the ratio of observed-to-expected adverse events is higher seems similar to the process of selecting important features in a decision tree model, and it inspires us to consider the possibility of using the feature importance calculated from machine learning models for screening adverse event signals.
The purpose of this study is to suggest a machine learning-based approach using feature importance for monitoring vaccine adverse events. We established our active surveillance model using elderly flu vaccination records provided by the Korea Disease Control and Prevention Agency (KDCA) and their claim data combined with data from the National Health Insurance Service (NHIS). We demonstrate the reliability of our approach by comparing the results of our model when applied on national claim data with the results of other adverse event databases and the literature for two adverse events: anaphylaxis and agranulocytosis. Moreover, to evaluate its applicability for vaccines, we evaluated the risk of flu vaccination for the elderly on the two health outcomes of interest (HOIs). Our model can be adapted to pandemic situations such as COVID-19 to quickly identify the adverse events of newly developed vaccines.
METHODS
Data description
We used a combined database that consists of a flu vaccination record database for the elderly from the KDCA and a claims database from the NHIS. First, the KDCA extracted the vaccination data and sent them to the NHIS for merging with the claim data. Because these two sets of data contained the resident registration number as the common primary key, the NHIS joined the two datasets using that key and then anonymized the identifier to avoid reidentification. Afterwards, we received the claims data joined with the vaccination records from 2015 to 2019 of this population from the NHIS with anonymized identifiers. Flu vaccination database that we used for our research consists of vaccination data for seniors who are over 65 years of age and received the flu vaccine from 2015 to 2018. The KDCA vaccination data includes the demographic information of the vaccinated and general information related to the vaccination such as the vaccine code, the vaccination time, and lot number of the vaccine. The claims data contains demographic information such as birth year and gender as well as medical treatment data such as diagnoses and prescriptions.
Data preprocessing
We selected anaphylaxis and agranulocytosis as the two HOIs. The Korean Standard Classification of Diseases (KCD-7) codes to determine each HOI are T78.0, T78.2, T80.5, and T88.6 for anaphylaxis21 and D70 for agranulocytosis.22
Data preprocessing consisted of 5 steps. We first extracted the “person identifier,” “prescription identifier,” and “diagnosis date” data for each HOI (except for ruled-out diagnoses) from the NHIS cohort. Second, from the prescription table, we obtained all prescription information for the extracted subjects: “prescription identifier,” “drug code,” and “prescription date.” For the “drug code,” the first 4 digits of the Anatomical Therapeutic Chemical (ATC) code was used. Third, we extracted personal information from the demographic table, which contains information such as the “person identifier,” “birth year,” “living area,” and “income level.” Fourth, we excluded subjects who did not have any demographic information. Finally, we extracted the “person identifier” and “vaccinated date” data for those individuals who were diagnosed with each HOI from the KDCA vaccination database.
Study design
To extract features for use as input to the machine learning model, we adopted case-crossover, which is a major epidemiological design used in vaccine research. If a patient had one HOI diagnosis during the study period, the diagnosis date was used as the index date. If a patient had multiple HOI diagnoses, we treated two consecutive diagnoses as one when the difference in the date of diagnosis was less than 31 days, and used the first diagnosis date as the index date. When the diagnoses were recurrent and more than 31 days apart, we considered recurrent diagnoses as independent HOIs. The minimum interval between diagnoses was set at least six months.
The period of 14 days before the index date was used as the risk window, and we randomly chose 14 days as control windows (excluding the days in the risk windows and washout periods). Next, we extracted all the prescription and vaccination records corresponding with each window. Windows that did not include any records in each period, we excluded from the research. If there are no prescription or vaccination records in the risk window, only the control windows were used. For anaphylaxis, 7,332 people out of 14,047 had control windows only, and for agranulocytosis, this was true for 5,712 people out of 28,005. The overall research process is summarized in Figs. 1 and 2.
Fig. 1
Flow chart of the study. (A) Anaphylaxis. (B) Agranulocytosis. Among the whole population, the numbers of people who were diagnosed with anaphylaxis or agranulocytosis at least once were 15,015 and 30,223, respectively. We selected people who did not have ruled-out diagnoses and for whom demographic information was available. After adapting exclusion criteria, the final sample size was 14,094 for anaphylaxis and 29,481 for agranulocytosis.
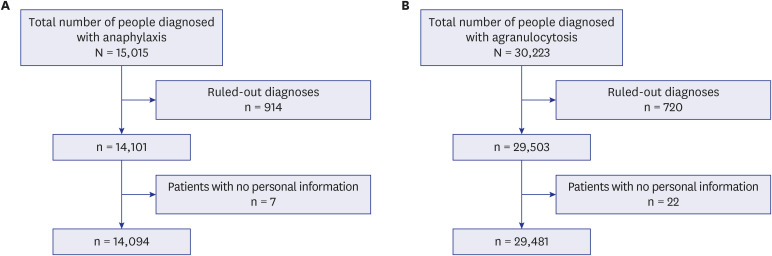
Fig. 2
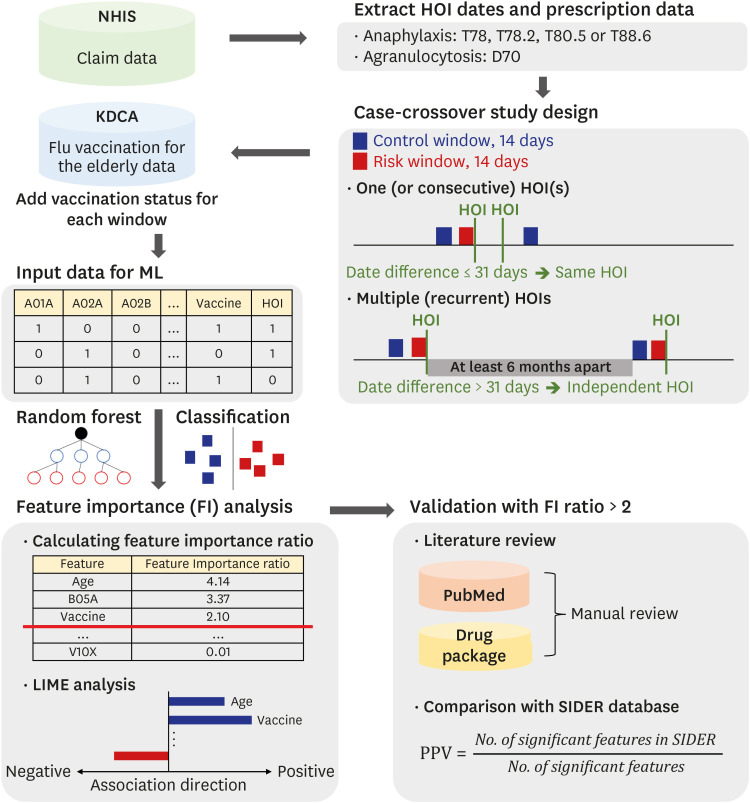
Research workflow for developing an active surveillance system. First, total HOI diagnosis dates were extracted using the NHIS claim dataset. The period of 14 days before the HOI diagnosis was set as a risk window. The control window was randomly selected for 14 days excluding the risk window and washout period. If a HOI occurred several times, the HOI that re-occurred within 31 days was considered as the same and a continuous event of the previous HOI. In order to ensure independence between HOIs, a risk window was defined only for recurrent HOI events where the interval between HOIs was more than 6 months apart. Second, the prescription and vaccination information that occurred in each window was collected. If there was no prescription and vaccination information in the window, the window was removed. At the final step, the HOI prediction model was learned using the prescription and vaccination information in each window. After that, using the feature importance ratio and LIME analysis of the model, a suspected drug or vaccine that could cause the HOI was determined.
FI = feature importance, HOI = health outcome of interest, KDCA = Korea Disease Control and Prevention Agency, LIME = Local interpretable Model-agnostic Explanation, NHIS = National Health Insurance Service, SIDER = Side Effect Resource database.
Machine learning model construction
We developed a random forest-based model for this study. The extracted prescription and vaccination records were used as the input values, and the targeted outcome was a HOI (i.e., whether the extracted information was from the risk or control window). The input dataset was randomly split into training (80%) and test (20%) sets. To avoid overfitting and obtain generalized performance results, we performed bootstrapping 100 times. Evaluations were performed on both the training and test sets. Sensitivity, specificity, the f1-score, accuracy, and the area under the curve (AUROC) were calculated as performance parameters.
Feature importance was evaluated to determine features were important for detecting each HOI. We obtained the overall feature importance values from each bootstrapping result. We defined the feature importance ratio as the ratio of each feature's average importance value to the average of all feature importance (except those with zero importance) over 100 bootstrapping trials. We treat features with a feature importance ratio of more than 2 as candidates that indicate adverse events.

Validation of the detected signals
To validate our study results, we reviewed the literature manually and compared the study results with the Side Effect Resource (SIDER) database. In the literature review, we searched for an association between the HOI and important features from our study results and calculated the ratio of the number of important features with references to the total number of important features. Using the SIDER database, we calculated the positive predictive value (PPV), which is the ratio of the number of important features that had a record in SIDER to the total number of important features.
Local interpretable Model-agnostic Explanation (LIME) analysis
LIME is a method to check which variables influenced the prediction results and how much they did so in a nonlinear machine learning prediction model, which is difficult to interpret.23 The random forest model provides the feature importance, which indicates the influence of a feature on the prediction result, but it does not indicate whether the variable has a positive or negative influence on the prediction. For example, if the feature importance of vaccination is 0.9 in a random forest model, vaccination may be informative in distinguishing people without adverse events, but there is no information whether this effect is positive or negative on the HOI. The results of LIME could provide the direction of association between the features and HOI by estimating the change in prediction results caused by changing the local values of each feature.
Software
In our study, the data preprocessing and model development scripts were written in Python version 3.6 using the scikit-learn Python package. We tuned the hyperparameters of our model using scikit-learn’s RandomForestClassifier and RandomizedSearchCV functions.24 To interpret the machine learning results, the LIME package was used.23
RESULTS
Table 1 summarizes the patients' demographic information for the total dataset and each HOI cohort at the first diagnosis. Because we analyzed flu-vaccinated elderly subjects, the mean age of each anaphylaxis and agranulocytosis cohort was 73 and 71 years, respectively, and the numbers of each HOI occurring at least once were 8,335 and 20,673, respectively. In addition, the numbers of data with vaccination in each HOI dataset were 35,536 and 17,216, respectively.
Table 1
Baseline characteristics at first HOI diagnosis

Performance
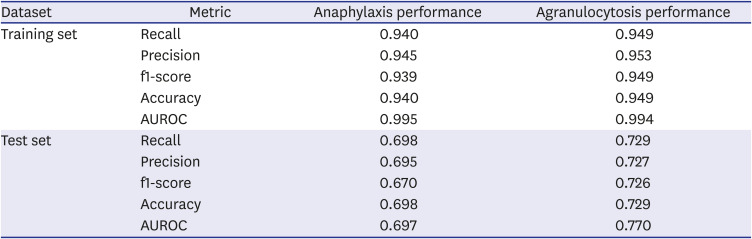
Table 2 presents the performance of the surveillance model for each HOI. On the training data, the performance metrics were all over 0.90, which means the model was trained well to predict whether each HOI would occur or not. For the test data for anaphylaxis, it scored about 0.69 in the AUROC, accuracy, recall, and precision metrics and 0.67 in f1-score on the test set. For agranulocytosis, the recall, precision, f1-score, and accuracy metrics of the model using the test set scored around 0.72.
Table 2
Performance of the machine learning model for each health outcome of interest
Feature importance list
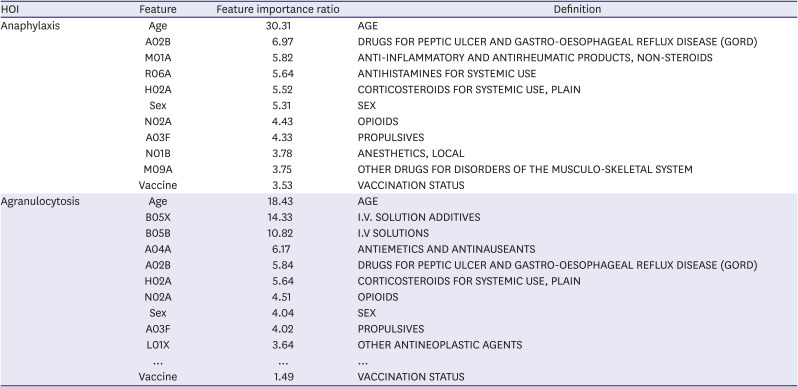
The importance of the features of the model for predicting HOIs and their feature importance ratios are presented in Table 3. Whole features with an importance ratio over 2 are listed in the Supplementary Materials. Twenty-seven features were found to be important because their feature importance ratio was over 2. Age had the highest feature importance ratio, and sex was the 6th most important feature. The status of flu vaccination was also significant (importance ratio: 3.53) and ranked 11th. Among drug-related features, drugs for peptic ulcer and for gastro-esophageal reflux disease (GORD), nonsteroidal anti-inflammatory drugs (NSAIDs), antihistamines, and corticosteroids ranked high. In the results of agranulocytosis, 25 features had a feature importance ratio of over 2. The most important feature was age, with a feature importance ratio of 18.4, and the status of vaccination was ranked 38th with a feature importance ratio less than 2 (1.49). Blood substitutes, solutions, antihistamines, drugs for GORD, and corticosteroids ranked high as drugs (in that order).
Table 3
Feature importance ratios for the top-10 features and vaccine
Validation of the important features
Literature evidence
In anaphylaxis, among the 27 features that had an importance ratio of over 2, 19 features (70%) were mentioned as having an association with anaphylaxis in the literature such as scientific journals (see Supplementary Table 1 for details). For example, beta-lactam antibiotics, NSAIDs, opioids, and neuromuscular blocking agents are considered the most common anaphylaxis-inducing drugs,25 and they were included in our study results. Montañez et al.26 noted that the presence of concomitant diseases (asthma, mastocytosis, and cardiovascular diseases) could increase the risk of anaphylaxis, and the drugs used for cardiovascular diseases (blood glucose lowering drugs, lipid modifying agents, and angiotensin-II antagonists) or allergy (antihistamines and corticosteroids) were also included in the study results.
Among 25 features that have an importance ratio of over 2 in agranulocytosis, 19 features (76%) were already mentioned (or remarked on) in the literature such as scientific journals, public documents, or drug packages (see Supplementary Table 2 for details). For example, Schweizer et al.27 reported that 23.8% of patients who had a high risk of prostate cancer had febrile neutropenia after taking leuprolide (ATC code: L02AE02). A case report mentioned a patient who took tamsulosin (ATC code: G04CA02) at 0.4 mg/day with other drugs including octreotide and was diagnosed with neutropenia.28
Comparison with SIDER data
Among 48 drug-related features which had a feature importance ratio of over 1, 38 features including NSAIDs, anti-infectives, and antidepressants were also listed in SIDER as drugs that can induce anaphylaxis (PPV 79.17%). For the 24 drug-related features that had an importance of over 2, 17 of them were listed in SIDER (PPV 70.83%) (Fig. 3A).
Fig. 3
Comparison of SIDER-listed features and features with high importance ratios. (A) Anaphylaxis. (B) Agranulocytosis. The Venn diagrams show the number of features in each result, and the intersection includes those features that are not only already listed in the SIDER database but also have an importance ratio of over 1 (left) or 2 (right).
GORD = gastro-esophageal reflux disease, NSAID = nonsteroidal anti-inflammatory drug, SIDER = Side Effect Resource database.
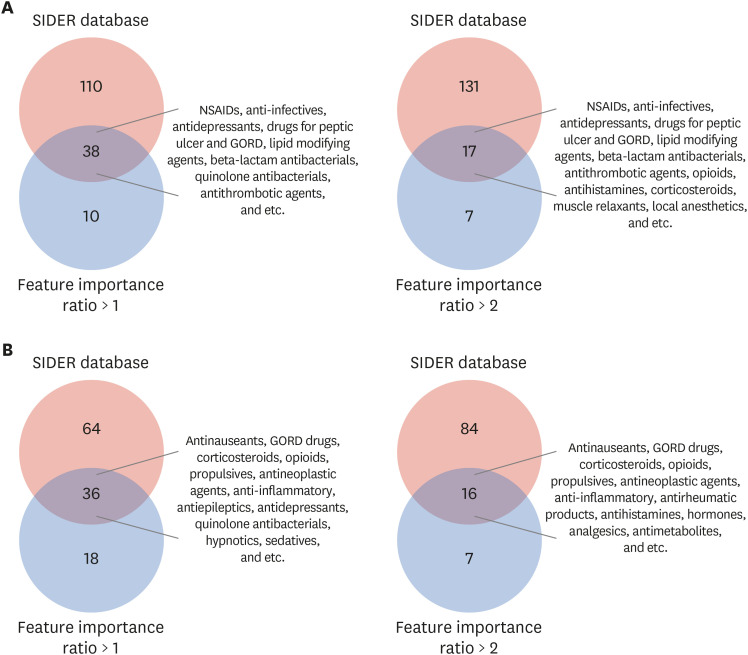
Among the 54 drug-related features that had an importance ratio of over 1, 36 features including antinauseants, antihistamines and antidepressants were also listed in SIDER as drugs that can induce agranulocytosis or neutropenia (PPV 66.67%). Of the 23 features that have an importance of over 2, excluding age and sex, 16 of them were listed in SIDER (PPV 69.57%) (Fig. 3B).
LIME analysis results
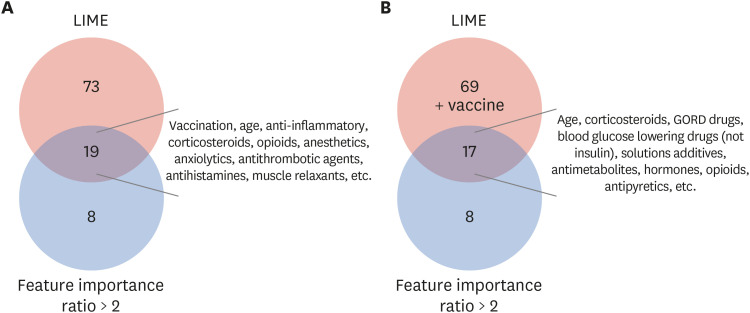
According to the LIME analysis, 19 of 27 features (70%) had positive relationships with anaphylaxis. Vaccination had a high feature importance ratio of 3.53 and a positive relationship with anaphylaxis (Fig. 4A). Moreover, 17 out of 25 features (68%) had positive relationships, which means each feature can help induce agranulocytosis. Vaccination status had a positive relationship with agranulocytosis, but the importance ratio was 1.49 (Fig. 4B).
Fig. 4
Comparison of LIME positive features and features with an importance ratio of over 2. The Venn diagrams show the number of features in each result and the intersection includes those features that are not only LIME positive but also have an importance ratio of over 2 (A) for anaphylaxis and (B) for agranulocytosis.
GORD = gastro-esophageal reflux disease, LIME = Local interpretable Model-agnostic Explanation.
DISCUSSION
Our study demonstrates that the machine learning-based vaccine adverse event monitoring system was able to detect which features affected agranulocytosis and anaphylaxis using the elderly flu vaccine cohort data provided by the NHIS and KCDA. The model was trained well, with a training data AUROC of over 99% and predicted HOI occurrences on the test data with AUROC values of around 70% for both outcomes. We proved that most features with an importance ratio of over 2 were related to the occurrences of each HOI by investigating whether each feature was mentioned in the scientific journals or with respect to drug packages. For features with an importance ratio over 2, the PPVs were 69.6% and 70.8% for agranulocytosis and anaphylaxis, respectively, when compared with data from the SIDER database. Vaccination status was considered to be an important feature in anaphylaxis surveillance results. This result is consistent with the fact that anaphylaxis is known to be an adverse reaction of the flu vaccine.29 Overall, this indicates that our prediction model, which is a machine learning-based surveillance method that is suitable for big data analysis, has the potential to detect important features that correspond with each HOI.
Our model can be used as a vaccine surveillance system because of its strengths related to surveillance. First, researchers can easily determine lists of suspected factors that can cause a HOI. Traditional statistical methods must calculate all the correlations between each factor and target, but our model can compare whole factors including all kinds of drugs, vaccination status, and demographic features simultaneously for the same HOI. The matching of adverse events and target drugs is often dependent on experts with domain knowledge or passive reporting systems. However, because the drug development process has accelerated and numerous drugs are now on the market, it is difficult for experts to identify HOI-drug pairs. Our research can be effectively used to proactively determine suspicious HOI-drug pairs. Moreover, the random forest model used in this study is known to have better performance and speed than the regression model as the amount of data and the number of features increases, which is more suitable for the analysis of big data.30
Our model also demonstrated the potential for determining suspected drug-HOI pairs considering drug–drug interactions. When calculating feature importance, it considers all drugs that were administered within the risk period. For example, ketorolac tromethamine, which is called Toradol, is an NSAID for treating severe pain.31 The ATC group of ketorolac is M01A, and that of tromethamine is B05B (as a blood substitute). There is no relationship between each drug and agranulocytosis, but the Food and Drug Administration (FDA) has said that the mixture of two drugs can cause agranulocytosis as a side effect.31 This indicates that our results can imply drug–drug interactions.
Our model can detect suspicious drugs that the SIDER database does not contain. Because the SIDER database contains drug-HOI pairs up to 2015, there may be adverse reactions that had not been discovered at that time. We searched for suspicious drugs, which are called false positives and had a high importance ratio in our model. Therefore, we tried to obtain the reliability of the results through a literature search on false positive analyses and the results. First, our model outputs that A03F (propulsive) had a high importance ratio for inducing anaphylaxis, but this is not listed in the SIDER database. However, we found that Dhakal et al.32 mentioned anaphylaxis as a very rare side effect of Domperidone. Second, our model said G04C (drugs used in benign prostatic hypertrophy) was important for inducing agranulocytosis, but this is also not listed in the SIDER database. We found there was a case in which tamsulosin induced neutropenia and thrombocytopenia.33 These false positive related evidences make our model more powerful.
Another strength of our model is that it can screen for all factors that can induce a targeted HOI. In other words, periodic screening is possible by determining a HOI with a high fatality rate and a high risk, and this model can be effectively used by drug-related government departments. We present a new surveillance process accordingly: After listing all suspected drugs or vaccines that could cause a HOI using our model, an expert can select a possible HOI-drug pair from among the candidate pairs output by the model and perform a precise statistical analysis. Finally, if a significant result is found in the statistical analysis, a clinical verification can be performed through an epidemiological investigation. By providing suspicious drug-HOI pairs, surveillance can be performed faster and more effectively than current approaches, which rely on expert knowledge or passive reporting.
There are some limitations of this study that should be declared. First, machine learning-based models are more effective when the number of data and features are large but the data used in this study were not large enough to confirm the advantages of machine learning. In addition, because the data of elderly people who had been vaccinated for flu vaccine was used, the age range of the cohort was limited. However, through this study, we confirmed that the machine learning-based active surveillance monitoring system for adverse events can be effective. Second, feature importance analysis does not guarantee a causal relationship between drugs and adverse events. For example, among the factors included in the feature importance for the results of agranulocytosis, there were cases in which adjuvants such as fluids were present. However, in the case of adjuvants, their purpose and usage are clear, so the researcher can easily filter them out. The purpose of this study is not to investigate the exact causal relationship between drugs and HOI, but to quickly monitor adverse event candidates. Moreover, for screening purposes, the method proposed in this study could be effectively used to determine drug prescription patterns that are related to HOI. Third, our method can provide PPVs for predicting HOI induced by drugs, but it cannot provide sensitivity because we cannot know the complete list of drug-induced adverse reactions. This is a fundamental limitation of surveillance studies that aim to detect unknown adverse events. However, by providing a false positive analysis, we obtain the reliability of the research.
To our knowledge, this is the first study to develop a machine learning-based surveillance system for detecting suspicious factors that can induce adverse events using a nation-wide insurance claim and vaccination database. The results of the study demonstrated that our model can list all the factors related to a HOI simultaneously. We expect that our model will help to make the adverse event surveillance process more efficient.
 XML Download
XML Download