

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Despite global efforts to develop and improve treatments, cardiac arrest is a major global health problem and remains a leading cause of mortality.12 The estimated number of annual out-of-hospital cardiac arrest (OHCA) occurrences is 95 per 100,000 population in the United States,3 67 to 170 per 100,000 population in Europe,4 and 60 per 100,000 population in South Korea.5 The annual incidence of in-hospital cardiac arrest (IHCA) has been reported as 6–7 cases per 1,000 hospital admissions in the United states,6 and as 1.5–2.8 per 1,000 hospital admissions in Europe.4 The annual incidence of IHCA in South Korea, however, has not been widely studied. The survival to hospital discharge rates for OHCA are 8.5% and 8% in the United states and Europe, respectively,34 and the survival rate of OHCA is < 8.7% in South Korea.5
The incidence and mortality of cardiac arrests vary according to patient characteristics such as age, sex, and urbanization of the residential area.789 Moreover, several studies have indicated an association between mortality and hospital level or volume.101112 High-level hospitals or academic medical centers produced better survival rates due to their ability to facilitate specialized post-cardiac arrest care such as early coronary intervention and targeted temperature management (TTM).101112 However, Cudnik et al.13 found no independent association between hospital volume and survival after adjusting for patient characteristics, initial rhythm, the witnessed arrest, presence of bystander cardiopulmonary resuscitation (CPR). They also emphasized that resources and personnel, not hospital volume, were key indicators of resuscitation care to improve arrest outcome and to deliver high quality post-cardiac arrest care.
Although standardized resuscitation guidelines are updated and implemented internationally, there remain variations in survival and post-cardiac arrest care by hospital, region, and country.23 Specialized centers such as cardiac arrest centers have sufficient resources for post-cardiac arrest care such as early coronary intervention, and therefore may be effective for improving patient outcomes.14
In this study, we aimed to analyze the characteristics and mortality of patients who suffered cardiac arrest, by hospital level, using the National Health Insurance Services (NHIS) database, which covers the entire Korean population and medical institutes. We also sought to reveal differences in post cardiac arrest care and hospital costs by hospital level, and compare treatments before and after the changes in the resuscitation guidelines.
METHODS
Data source
Data were obtained from the Korean NHIS claim database, and were collected from January 2006 to December 2015. The NHIS represents a unique single insurer under a national healthcare system, which covers 96% of the Korean population and a medical aid program that covers 3–4% of the population. The database contains de-identified information on all insurance claims, including basic demographics, type of health insurance, diagnosis as coded by the International Classification of Diseases, 10th edition (ICD-10), and information on the type of medical institution admission, treatments, mortality rates, and hospital costs.15
Study population
We identified patients with suffered cardiac arrest during their index hospitalization using the claim codes for a CPR procedure (M5871, M5873-7) between 2006 and 2015. Index hospitalization was defined as the first instance of hospitalization in which a claim was made for a CPR procedure code. When there was another admission, including an emergency room (ER) visit or a hospitalization episode in a different hospital within 2 days, we defined them as one index hospitalization event and patients were included in the latter hospital. We used CPR procedure codes instead of diagnosis codes as Cho et al.16 previously reported that the use of ICD-10 diagnosis codes alone was an insensitive method for identifying cardiac arrest patients, and that the use of procedure codes showed better sensitivity and positive predictive value for identifying patients who have suffered cardiac arrest in South Korea.
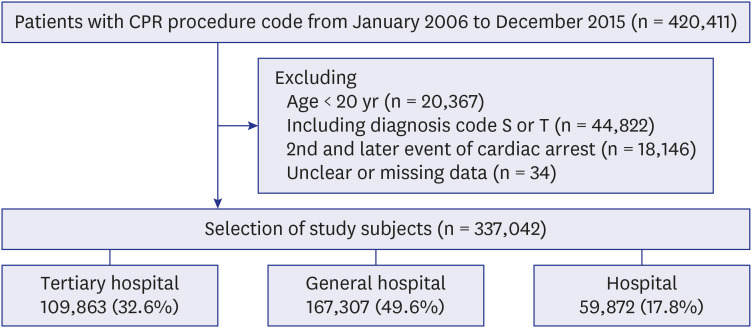
Patients were included in the study if they had undergone cardiac arrest, were ≥ 20 years old, had a claim code for a CPR procedure between 2006 and 2015, and had 1-year follow up data until 2016. Patients were excluded if they were < 20 years old, had a trauma-related diagnosis code (S or T) or a code from an oriental medical institute, drug store, or dentist, had a second or later event of cardiac arrest, or had missing data (Fig. 1).
Definition of variables
From the NHIS database, we collected information on patient's age, sex, urbanization level of the residential area, level of hospital at index hospitalization; comorbidities, which were differentiated by diagnostic codes at the medical institute before index hospitalization, and Charlson Comorbidity Index (CCI) by referring to diagnostic codes and hospital information.17 A disease was defined as “Comorbidity” when the relevant diagnostic code was recorded at least twice within 1 year during visits to clinics, or when a patient had one or more hospitalizations within 2 years before index hospitalization (Supplementary Table 1). The urbanization level of the residential area was classified based on the geographical region of the administrative divisions, while considering the population.
Patients were categorized into tertiary hospital, general hospital and hospital groups according to where they were admitted. The level of hospital is classified by the Ministry of Health and Welfare, according to designation criteria that take the level of medical service, function of medical care and training, human resources, and facilities into account. Tertiary hospitals have more than 20 professional departments with a resident training function, general hospitals have a minimum of 100 beds with 7–9 professional departments, and hospitals are defined as health care institutions with a minimum of 30 beds. We extracted details about specific treatments including defibrillation, extracorporeal membrane oxygenation (ECMO), percutaneous coronary intervention (PCI), coronary angiography (CAG), coronary artery bypass graft (CABG), continuous renal replacement therapy (CRRT), hemodialysis, electroencephalography (EEG), TTM, and several medications from information on reimbursements for each medical service (Supplementary Table 2). The estimated total hospital costs, length of hospital stay (hospitalization days), and length of intensive care unit stay (ICU days) were also extracted.
Study outcomes
The primary end point was the mortality rate within 30 days and 1 year of the index date. The secondary endpoints were hospitalization days, ICU days, short term hospital costs (within 30 days of the index date), and long-term hospital costs (from 31 days to 1 year from the index date). The exchange rate was assumed to be 1,155 Korean won per 1 United States dollars (USD).
Statistical analysis
Demographic data are described using proportions for categorical variables and means with standard deviations (SDs) for the continuous variables, at 30 days and 1 year follow-ups. Chi-square tests were used for categorical variables, while t-tests and analysis of variance were used to compare averages for continuous variables. Adjusted odds ratios (aORs) with 95% confidence intervals were calculated using multiple logistic regression analysis. Age, sex, insurance type, urbanization level, admission route, comorbidities, resuscitation medication (epinephrine and atropine), defibrillation, angiography, and guideline changes were adjusted to determine the association between hospital-level and 30 days and 1 year mortality rates. All P values were two-tailed with a significance threshold of P < 0.05. All statistical analyses were performed using SAS ver. 9.4 (SAS Institute, Cary, NC, USA).
Ethics statement
The study was approved by the Institutional Review Board (IRB) of the Korea University Medical Center (IRB No. 2017AN0083). The requirement for informed consent was waived due to the retrospective nature of the study and because it was based on a de-identified administrative database.
RESULTS
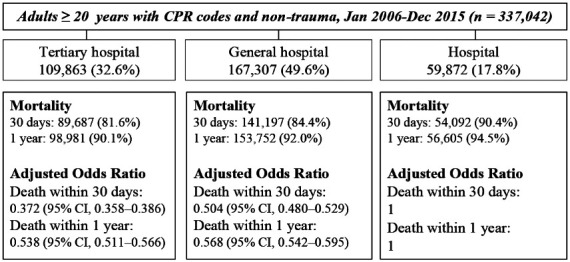
Data from a total of 337,042 patients were obtained from the NHIS database from January 2006 to December 2015. Patients were categorized into three groups according to the level of the hospital where they were admitted. The tertiary hospital, general hospital, and hospital groups accounted for 32.6%, 49.6%, and 17.8% respectively (Fig. 1).
The tertiary hospital group had the youngest mean age (tertiary hospital vs. general hospital vs. hospital, mean ± SD, years: 64.9 ± 14.8 vs. 67.1 ± 14.7 vs. 72.1 ± 14.0, P < 0.001). The proportion of elderly patients > 75 years (tertiary hospital vs. general hospital vs. hospital, %: 29.0 vs. 36.3 vs. 51.5, P < 0.001) and medical coverage (tertiary hospital vs. general hospital vs. hospital, %: 10.5 vs. 15.4 vs. 21.3, P < 0.001) were lowest in the tertiary hospital group. The tertiary and general hospital groups had the highest proportion of admissions through the ER (tertiary hospital vs. general hospital vs. hospital, %: 76.0 vs. 79.1 vs. 32.6, P < 0.001) (Table 1).
Table 1
Characteristics of patients according to hospital levels
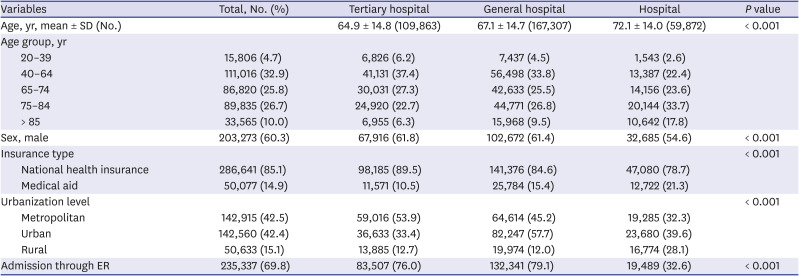
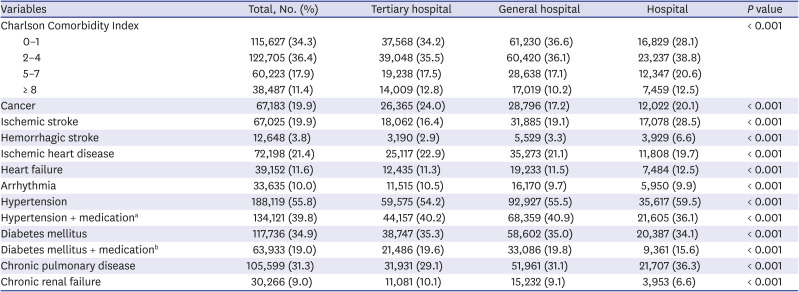
The severity of illness, reflecting comorbidities and indexed by CCI score, was lower in the tertiary and general hospital groups than in the hospital group. A sub-group analysis was conducted for comorbidities, which showed higher proportions of cancer (24.0%), ischemic heart disease (22.9%), arrhythmia (10.5%), and chronic renal failure (10.1%) in the tertiary hospital group. The proportion of patients with hypertension or diabetes mellitus taking antihypertensive or antihyperglycemic agents was higher in the tertiary hospital group than in the hospital group (Table 2).
Table 2
Comorbidities of patients according to hospital levels
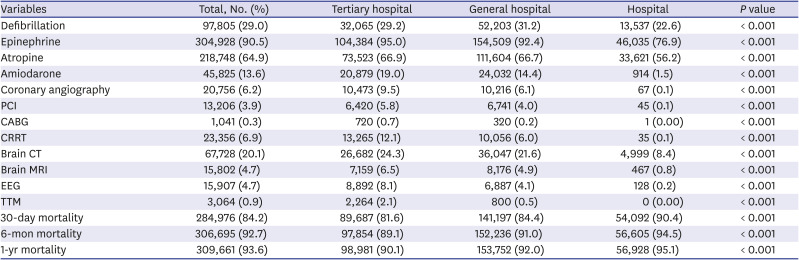
There were notable treatment differences among the three groups. Defibrillation (tertiary hospital vs. general hospital vs. hospital, %: 29.2 vs. 31.2 vs. 22.6, P < 0.001) was used more frequently in the tertiary and general hospital groups. Post-cardiac arrest care, including CAG, PCI, ECMO, CRRT, and TTM, was more frequently performed in the tertiary and general hospital groups than in the hospital group. The mortality at 30 days (tertiary hospital vs. general hospital vs. hospital, %, 81.6 vs. 84.4 vs. 90.4, P < 0.001) and 1-year (tertiary hospital vs. general hospital vs. hospital, %, 90.4 vs. 94.5 vs. 95.1, P < 0.001) were lowest in the tertiary hospital group (Table 3).
Table 3
Medications, procedures, outcomes of patients according to hospital levels
To examine the potential association between hospital level and mortality, we adjusted for age, sex, insurance type, urbanization level, admission route, CCI, comorbidities, defibrillation, resuscitation medication, angiography, and guideline changes through multiple logistic regression. The aOR for 30 days (tertiary hospital vs. general hospital vs. hospital, 0.372 vs. 0.419 vs. 1, P < 0.001) and the aOR for 1-year (tertiary hospital vs. general hospital vs. hospital, 0.538 vs. 0.604 vs. 1, P < 0.001) are presented in Table 4.
Table 4
Multiple logistic analysis for short-, mid-, and long-term mortality by hospital levels

aOR = adjusted odds ratio, CI = confidence interval.
aAdjusted for age, sex, insurance type, urbanization level, admission route, comorbidities, defibrillation, medication (epinephrine and atropine), angiography, and guideline change through logistic regression analysis of the relationship between level of hospital on death within 30 days, 6 months, and 1 year.
We compared hospitalization days, ICU days, short- and long-term hospital costs per patient among the three groups. The tertiary and general hospital groups had longer hospitalization and ICU days than the hospital group, and both groups had higher hospital costs especially within 30 days (tertiary hospital vs. general hospital vs. hospital, USD 5,486 vs. 3,167 vs. 1,086, P < 0.001) (Table 5). Moreover, the short-term hospital costs were 5 times higher in the tertiary hospital group than the hospital group. We also performed subgroup analysis of the hospitalization days and costs in survivors at 1-year (Supplementary Table 3).
Table 5
Hospitalization days and hospital costs according to hospital levels

Following the guideline change in 2010, the administration of atropine decreased from 91.5% to 45.6% in the tertiary hospital group, from 86.1% to 50.5% in the general hospital group, and remained similar in the hospital group, from 56.4% to 55.8%. The measurement of end tidal carbon dioxide (CO2) increased in the tertiary and general hospital groups. Post-cardiac arrest care, including CAG, PCI, ECMO, and TTM, was more commonly provided in the tertiary and general hospital groups after the guideline change (Table 6). The patient demographics before and after the guideline change are shown in Supplementary Table 4.
Table 6
Medications and procedures before and after guideline changes, by hospital levels
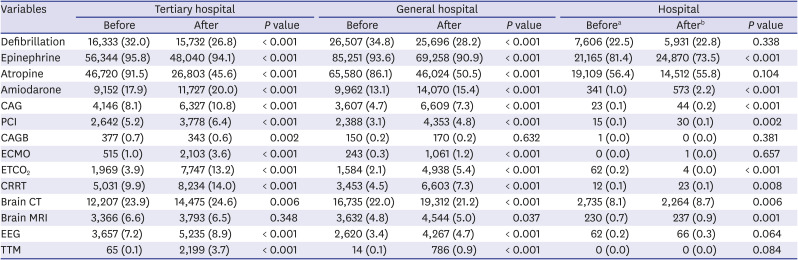
aBefore: January 2006 to December 2010, bAfter: January 2011 to December 2015.
CAG = coronary angiography, PCI = percutaneous coronary intervention, CABG = coronary artery bypass graft, ECMO = extracorporeal membrane oxygenation, ETCO2 = end tidal carbon dioxide, CRRT = continuous renal replacement therapy, CT = computed tomography, MRI = magnetic resonance imaging, EEG = electroencephalogram, TTM = targeted temperature management.
DISCUSSION
In this study, we found variations in the characteristics and mortality of patients who suffered cardiac arrest, by the level of hospital. The high-level hospital groups (tertiary and general hospital groups) had lower mortality after adjusting for patient and hospital factors. These variations in mortality may be affected by patients’ characteristics, post-cardiac arrest care, and adherence to changes in guidelines.
Regarding patients' characteristics, the patients in the tertiary and general hospital groups were younger, had a lower proportion of medical aid coverage, and fewer comorbidities. On account of the fact that elderly patients are more likely to have multiple comorbidities and to be denied aggressive treatments during both intra- and post-cardiac arrest,7 older age is known to be associated with poor outcome after OHCA as well as IHCA.718 The proportion of a CCI < 2 was higher in the tertiary and general hospital groups than that in the hospital group. The CCI is an indicator of the severity and complexity of comorbidities, and an increasing CCI was associated with increased risk of mortality in cardiac arrest patients.19 The lower proportion of medical aid coverage in the tertiary and general hospital groups could also influence the mortality rate, as several studies reported that lack of adequate insurance coverage could impact outcomes after both IHCA and OHCA due to disparities in access to health care or differential delivery of medical treatments after admission.2021
This study showed that post-cardiac arrest care was more commonly provided in the tertiary and general hospital groups, especially in short-term period. Growing evidence supports a role for post-cardiac arrest care that can reverse the underlying cause of arrest and limit ischemia-reperfusion injury that often occurs in cardiac arrest.22 CAG and PCI are necessary to correct cardiac etiologies of myocardial infractions.23 ECMO is an invasive and resource-intensive bridge treatment for maintaining organ perfusion and correcting the cause of cardiac arrest during both intra- and post-cardiac arrest.24 TTM is recommended in comatose survivors of cardiac arrest to prevent worsening of neurological ischemia-reperfusion injury.25 Such specialized post-cardiac arrest care recommended by the international guideline is required immediately after return of spontaneous circulation (ROSC) and demands costly medical facilities and multidisciplinary teams. These resources are available for 24 hours in most tertiary hospitals and several general hospitals. Notably, the difference between the hospital costs in the tertiary hospital group and the hospital group showed a bigger difference in the short-term period, which suggested that post-cardiac arrest care was mainly provided during the acute period. Also, longer hospitalization days in the tertiary and general hospital groups can contribute to higher hospital costs in both groups, even though the medical cost is reimbursed at a rate determined by the level of hospital.
In this study, the tertiary and general hospital groups showed better adherence than the hospital group to the resuscitation guideline change. In the 2010, AHA recommended some major changes in the adult advanced cardiovascular life support algorithms; Atropine was no longer recommended in the management of pulseless electrical activity or asystole; Measurement of the end-tidal CO2 level was recommended for monitoring CPR quality and detecting ROSC, as well as to confirm endotracheal tube placement; Post-cardiac arrest care such as PCI and TTM was emphasized and should be provided if clinically indicated.26 Among the three groups, the use of atropine markedly decreased, and the measurement of end-tidal CO2 increased in the tertiary and general hospital groups after the guideline change. PCI, TTM, and ECMO were more frequently provided in the tertiary and general hospital groups. These results suggested that high-level hospitals showed better guideline adherence, and thus they provided more post-cardiac arrest care which could meaningfully improve survival. Nas et al.27 reported that recognition of comprehensive post-cardiac arrest care and emphasis on PCI were important changes that contributed to improved survival and neurologic outcome after the 2010 guideline update.
After adjusting for patient characteristics, comorbidities, admission route, comorbidities, treatments, and guideline changes, the tertiary and general hospital groups had lower short- and long-term mortality rates. Similar to our findings, Kurz et al.10 suggested that higher-volume hospitals, which were capable of facilitating specialized post-cardiac arrest care, had higher survival rates of patients with cardiac arrest. Several studies also reported that teaching hospitals and hospitals with high volumes of CPR cases were associated with improved outcomes in patients with cardiac arrest, and found that high-level hospitals tended to have sufficient resources for post-cardiac arrest care with a multidisciplinary team that are available for 24 hours.282930 Although other studies showed that hospital factors, such as hospital volume, or the number of OHCA patients, were not independently associated with survival after adjusting for patient factors133132; these studies also agreed that an improvement in cardiac arrest outcome could be achieved by the availability of specialized post-cardiac arrest care.
High-level hospitals are designated by the government only when they are equipped with necessary resources, facilities and specialists as well as according to the hospital volume, and most of them are academic teaching hospitals in South Korea. As post-cardiac arrest care and training functions were mainly performed by these hospitals, lower mortality rates and better guideline adherence could be shown in the high-level hospital groups.
The presented results should be interpreted carefully in light of the following limitations. First, the insurance claim database does not include prehospital and in-hospital resuscitation information, including the presence of witnessed, initial rhythm, bystander CPR, and duration and quality of CPR; thus, we could not clearly divide the population into IHCA and OHCA groups. To compensate for this limitation, we analyzed the admission route as a surrogate for OHCA and IHCA, and considered that the patients who were admitted through ER were likely OHCA cases. Although the admission route was adjusted for analyzing the association between hospital level and mortality, our results could be affected by different characteristics and outcome of the IHCA and OHCA patients.33 Furthermore, the NHIS database does not include information on neurologic outcome, such as the Cerebral performance category, and therefore it cannot be used to investigate neurologic outcomes.
Second, the insurance claim database does not include the clinical information such as the etiology of cardiac arrest, medications and procedures, and laboratory data. These data did not embrace the purposes or time of treatments. Therefore, we could not ascertain whether the medications and procedures were provided for the treatment of cardiac arrest or not.
Third, there can be a referral selection bias due to the referral of patients from hospitals to general or tertiary hospitals for specialized post-cardiac arrest care, which could affect mortality rates.34 It was also reported that referral patients were healthier than average because they had survived the initial manifestations of their illness during the time necessary for referral and travel to the tertiary hospital.35
Lastly, despite the advantages of using nation-wide insurance claim data on all patients with cardiac arrest, insurance data are subject to errors related to coding and omission of costs, which was not covered by the NHIS. Moreover, the data did not include information on other types of chronic supportive care for outpatient rehabilitation, nursing homes, and prehospital managements including emergency medical service systems.
In conclusion, the tertiary and general hospital groups had lower mortality rates within 30 days and 1 year than the hospital group after adjusting for patient characteristics and hospital-related factors. The high-level hospital groups were younger, had a lower proportion of medical aid coverage, and fewer comorbidities. Post-cardiac arrest care was provided more commonly in the high-level hospital groups, which required higher hospital costs than the hospital group. The high-level hospital groups also showed better adherence to the resuscitation guideline change. Further investigations using clinical data will be required due to the limitations of the administrative insurance database.
 XML Download
XML Download