

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acromegaly is a chronic disease resulting from secretion of excess growth hormone (GH) and insulin-like growth factor (IGF-1) by a GH-producing pituitary adenoma, leading to bone and soft tissue overgrowth.1 As postoperative GH level is inversely associated with mortality,2 the purpose of treatment in these patients is to normalize GH and IGF-1 levels for symptom relief and to reduce mortality.34 Surgery through the trans-sphenoidal approach is generally the treatment of choice, and a first-generation long-acting somatostatin receptor ligand (SRl) may be used as the primary medical treatment for inoperable or incompletely removed cases. In case of primary treatment failure, second-generation SRIs such as pasireotide or GH receptor antagonists such as pegvisomant may be indicated as second-line therapy. Sterotactic radiosurgery may also be considered when the clinical response is insufficient.5
Acromegaly is rare, with a reported prevalence of 2.8–13.7 cases per 100,000 people and an annual incidence rate of 0.2–1.1 cases/100,000 people.6 Epidemiological studies of acromegaly have previously been conducted in Korea. In 1965 the Survey Committee for Endocrine Disorders in the Korean Endocrine Society first conducted a nationwide survey.7 Total 279 cases were confirmed from 26 university hospitals, and the annual incidence rate was estimated to be 1.4 cases per million per year. The Rare Disease Study Group in the Science and Research Committee of the Korean Endocrine Society also surveyed in a similar way from 2003 to 2007, with 1,350 patients diagnosed with acromegaly in 74 hospitals with annual incidence rate of 3.9 cases per million per year.8 Park et al.9 reported using Health Insurance Review and Assessment (HIRA) data surveyed from 2010 to 2014 that the annual incidence was 3.57 cases per million per year. It is known that the survival rates of patients with well-controlled GH or IGF-1 after treatment are similar to those of the general population.1011 According to a recent study, standardized mortality ratio in acromgaly patients is on the decline and malignancy is becoming a more major cause of death, unlike cardiovascular disease (CVD) was the main cause of death before.12 On the other hand, Holday et al.10 showed the coexistence of hypertension aggravates cardiomyopathy in patients with acromegaly. A significantly higher mortality rate was also observed when accompanied with diabetes.13
Since 1989, the nationwide health insurance system has been implemented in Korea, and a variety of medical information necessary to process the insurance claims is being securely stored and managed by the HIRA database. The data are open to researchers with the aim of contributing to the development of healthcare and medical knowledge under the supervision or consignment of the National Health Insurance Act and other statutes.14 This database has enabled many researchers to perform large-scaled clinical or epidemiological data analyses in Korea. Hence, our study was designed to utilize the HIRA claims dataset to determine the incidence and prevalence of acromegaly in Korea and to assess the comorbidities and survival benefits of the treatment modalities.
METHODS
Data collection
This was a nationwide population-based cohort study based on the HIRA claims dataset. Subscription in the National Health Insurance is mandatory for all Koreans who receive salaries or are self-employed and are required to report their income to the National Tax Service. According to the insurance system in Korea, the claims data with the appropriate diagnostic codes are submitted by service providers to the HIRA for reimbursement afterward. As mentioned previsouly, this claims data are released to investigators after deidentification for large-scaled analysis in Korea. It is of note that those diagnostic codes often fail to reflect the actual clinical conditions of patients due to diagnostic discrepancies or disease input errors.15 Because the HIRA database is de-identified, and does not allow investigators to retrieve a patients' individual laboratory test results, it is necessary to screen and obtain the group of patients satisfying the researcher's purpose of analysis within the dataset by applying multiple variables such as diagnostic codes, laboratory test and procedure codes, drug prescriptions and so on. This combination of variables in the data is called the “operational definition.”16 The reliability of data used is determined by how appropriately the operational definition identifies the actual target patient and extracts the proper data.
To apply more accurate operational definitions in our study, we crossmatched the benefit extension policy (BEP) application codes with the HIRA codes. The BEP in Korea was established to support medical expenses of patients with rare and incurable diseases such as cancers and rare genetic disorders accompanying high economic burden.17 The BEP code is assigned to diseases satisfying criteria of rarity and necessity to support the cost during diagnosis and treatment, and is mandatory to exempt certain portion of medical expenses needed to manage these diseases. Double comparison with the HIRA dataset and the BEP codes can assure the reliability of data extracted in our study.
Prevalence and annual incidence rate
Acromegaly was defined as a case in a patient who had a history of outpatient care or hospitalization based on both the International Classification of Diseases (ICD), the 10th Revision code (E22.0), and the BEP code (V112). We analyzed the prevalence and annual incidence of acromegaly during 2013–2017 with a washout period between 2009 and 2012 to calculate the incidence rate, which showed 1,093 patients with newly diagnosed cases of acromegaly.
Treatment effect
An effective treatment has been reported to normalize GH secretion and prevent metabolic complications in patients with acromegaly.3 Because the HIRA database includes information necessary to process the insurance claims and does not provide detailed data regarding clinical parameters such as individual laboratory test results or radiologic examinations, it is difficult to directly evaluate the treatment effects. To solve this limitation, we investigated the incidence of metabolic complications such as diabetes and hypertension after diagnosis with acromegaly between those with diagnosed but untreated acromegaly (defined as no treatment record after diagnosis) and those with treated acromegaly, which would enable us to indirectly observe the treatment effects in patients with acromegaly.
Among those newly diagnosed with acromegaly during 2011–2012 (n = 377), data of those with either hypertension (I10) or diabetes mellitus (E10–14) newly diagnosed during the follow-up period (2013–2017) were additionally extracted (hypertension, n = 147; diabetes mellitus, n = 109). We compared their incidence rates between those diagnosed and treated for acromegaly (treatment group) and those diagnosed but not treated for acromegaly (non-treatment group). In addition, after sub-dividing the treatment group into 1) medical, 2) surgical, and 3) medical and surgical treatment, each sub-group was compared with the non-treatment group for the incidence of hypertension and diabetes. Medical treatment was defined as those treated with somatostatin analogues (SA) or dopamine agonists. Those with surgical treatment were defined as patients treated by trans-sphenoidal approaches or radiologic therapy. This grouping was based on whether appropriate codes for either medical or surgical treatment was found during the follow-up period. This comparison was based on the notion that those with diagnosed and properly treated acromegaly would be less likely to experience metabolic complications when compared with non-treated patients (Supplementary Fig. 1).
Mortality
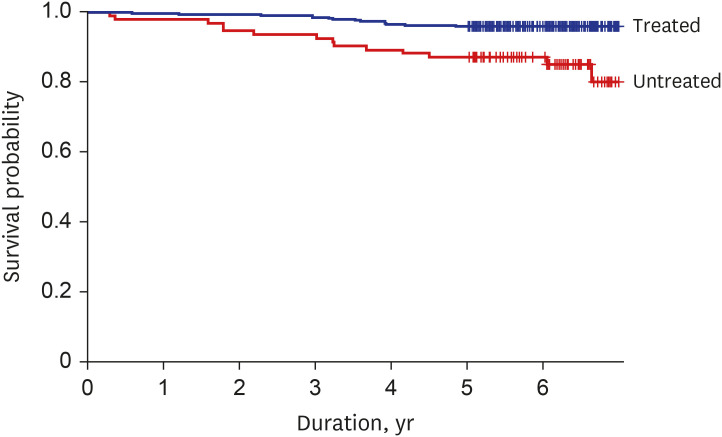
The mortality between those with diagnosed but untreated acromegaly and treated acromegaly was compared by using the identical dataset used for analyzing the incidence of hypertension and diabetes. For 377 patients with newly diagnosed acromegaly during 2011–2012, their mortality rates during 2013–2017 were compared between the treatment and non-treatment groups (Supplementary Fig. 2).
Statistical analysis
The hazard ratio (HR) and 95% confidence interval (CI) for hypertension and diabetes incidence and for mortality were estimated using the log-rank test and Cox's proportional hazard regression analysis. The multivariate model analysis was performed after adjusting for sex, age, and income level. The survival period was set between the date when acromegaly was first treated as the start date of observation, to either the date of a new clinical event, or on December 31, 2017, as the end date of observation. Patients who had been treated before the initial diagnosis of acromegaly were excluded from the analysis. The result was considered statistically significant if P < 0.05. Statistical analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
Epidemiologic data
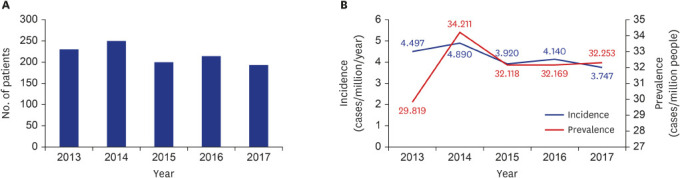
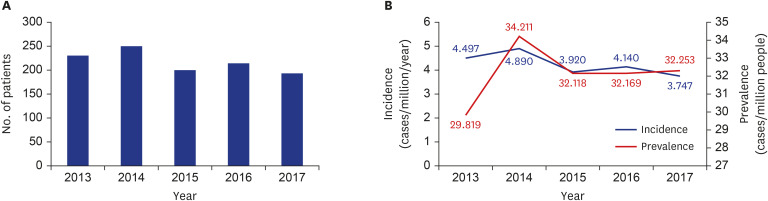
A total of 1,093 patients (M:F = 594:497) were newly diagnosed with acromegaly between January 2013 and December 2017 (Table 1). More than 200 people were diagnosed each year, and 195 were newly diagnosed in 2017 (Fig. 1A). The average annual incidence rate was 4.2 cases per million, and the prevalence rate increased in 2014 before reaching 32 cases per million (Fig. 1B).
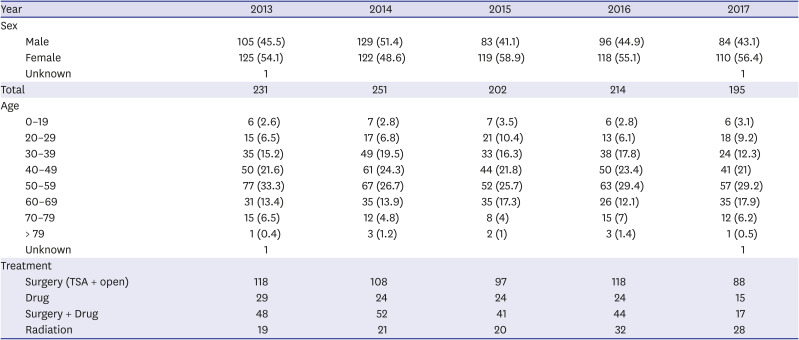
Table 1
Incidence of acromegaly in Korea between 2013–2017
Development of medical comorbidity according to treatment modality
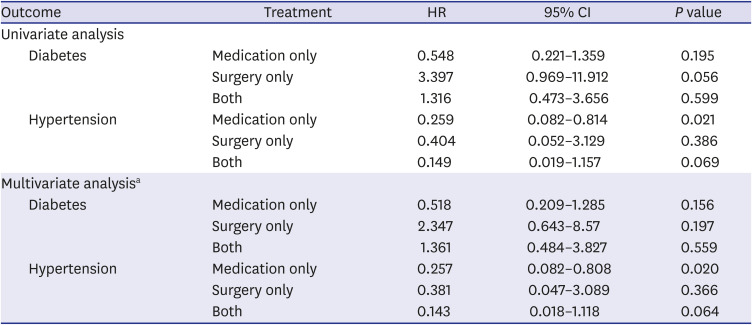
It was found that the risk of diabetes (P = 0.038) and hypertension (P = 0.025) was significantly lower in the treatment group than in the non-treatment group. Further analyses after subdividing the treatment group according to the treatment modality demonstrated that the incidence of diabetes in each group showed no significant difference when compared to the non-treatment group. However, the risk of hypertension in the medically treated group was significantly lower than that in the non-treatment group (HR, 0.259; 95% CI, 0.082–0.814; P = 0.021) (Table 2) and remained significantly lower after adjustment for confounders (HR, 0.257; 95% CI, 0.082–0.808; P = 0.020) (Table 2).
Table 2
Prevalence of diabetes mellitus and hypertension in patients with acromegaly
Survival analysis of acromegaly patients
According to the survival analysis conducted on patients newly diagnosed with acromegaly during 2011–2012, patients in the non-treatment group showed a significantly lower probability of survival (curve difference at P < 0.001 by log-rank) than those in the non-treatment group (Fig. 2), which remained significant after adjustment for confounders (HR, 3.668; 95% CI, 1.644–8.183; P = 0.002).
DISCUSSION
This study was designed to investigate the annual incidence and prevalence of acromegaly, which further compared the occurrence of complications by treatment modality in Koreans from January 2013 to December 2017. Survival rate analysis was also conducted between treatment and non-treatment groups. From 2013 to 2017, the annual incidence of acromegaly in Korea was 4.2 cases per million people per year. In previous epidemiological studies in Korea, Yang et al.7 reported the acromgaly annual incidence of 1.4 cases per million per year. Kwon et al.8 also reported 3.9 cases per million per year and Park et al.9 reported 3.57 cases per million per year. This was also similar to the annual occurrence rate of 2–11 cases per million people per year from a systematical review.6 Yang et al.7 and Kwon et al.8 studies were conducted using the Nationwide Survey method, whereas the Park et al.9 study used health insurance HIRA data as shown in this study, having different study designs with heterogenous study periods in each study. In addition, our operational definition was different from previous studies, which may have caused relatively different results. There were no significant differences in the development of diabetes accrding to treatment modalities. However, hypertension showed significantly lower incidence in the medical treatment group. Over a period of 6 years since diagnosis, patients treated for acromegaly had a significantly higher survival rate than the untreated patients.
Malignancy has recently been reported to be the leading cause of death in patients with acromegaly.12 However, cardiovascular disease also has still remained as one of the main causes of death for acromegaly.18 In particular, it is reported that the mortality rate from CVD is still high in patients with acromegaly and hypertension.19 It is known that the prevalence of diabetes and hypertension is higher than that in the general population.2021 Patients with acromegaly are known to be more likely to have concurrent hypertension; 1.9 times higher than that in the general population. This could be due to the direct anti-natriuretic effects of exess GH.22 Several animal studies have suggested that increased GH causes overactivation of the renin-angiotensin-aldosterone-system.23 Hyperinsulinemia also causes hyperactivity of the renin-angiotensin-aldosterone system, which promotes renal sodium reabsorption and thus increases plasma volume.24 It is also known that elevated insulin and GH levels contribute to hypertension by activation of the sympathetic nervous system.25 To indirectly estimate the therapeutic effects of acromegaly, we divided the acromegaly-treated patients into three groups: 1) medical, 2) surgical, and 3) medical plus surgical treatment group. The incidence of diabetes in the treatment group showed no significant difference when compared to the non-therapeutic group. We also investigated the incidence rate of hypertension after newly diagnosed acromegaly. This was similar to a previous study that showed significantly reduced development of hypertension after five years of medical treatment.26
As for diabetes, there was no significant difference between the treated and non-treated groups. This was unexpected and inconsistent with previous studies showing the improvement of glucose metabolism regardless of the outcome of surgical treatment.27 The study conducted by Kinoshita et al.28 on patients with acromegaly in Japan demonstrated that glucose metabolism did not normalize even after acromegaly treatment due to impaired beta cell function. In addition, Shekhawat et al.29 showed no significant difference between pre- and post-operative beta cell function in acromegaly patients with diabetes, and this was due to increased glucose-dependent insulinotropic polypeptide resistance and reduced beta cell function due to hyperglucagonemia. Similar to Japanese, Koreans are known to have reduced insulin secretion and compensatory insulin responses before the onset of diabetes,30 thus, decreased beta-cell function may fail to recover and lead to diabetes development even after treatment of acromegaly. This study was conducted before the second genration SA (pasireotide) was introduced in Korea which affects pancreatic beta cells and is believed to possibly raise the blood glucose level,31 and thus all of the subjects included in our study were treated with only the first-generation SAs. The first generation SA is known to bind to the somatostatin receptor type 2 (SSTR2) at the pituitary tumor cells, and SSTR2 is also expressed in the alpha cells in the pancrease possibly leading to the suppression of glucagon suppresion and hardly causing hyperglycemia.3233 Therefore, it is believed that the possibility of drug-induced diabetes or elevated blood glucose is not to be less likely to occur.
In our study, the treatment group had significant survival benefits compared to the non-treatment group. A previously reported survival analysis on acromegaly patients in New Zealand showed that the life expectancy was the same as that of the general population when the GH level was less than 1 g/L after treatment.10 A Finnish study, instead, showed that the life expectancies were the same as that of the general population if the GH levels remained below 2.5 g/L after treatment.11 Along with these results, our analysis confirmes and emphazises the importance of effective treatment to normalize GH secretion and prevent metabolic complications in patients with acromegaly, which could further assure the survival benefit. The previous study by Park et al.9 also compared the mortality, but compared between patient and general population, while our study compared between treatment and non-treatment group. This confirms the importance of treatment in patients with acromegaly.9 To our best knowledge, this is the first study to report the results of survival analysis in Korean patients with acromegaly according to whether treated or not.
In this study, patients with acromegaly were defined according to the operational definition based on both the claims data codes and the BEP codes in the HIRA database. This operational definition was considered to be appropriate because the incidence and prevalence of acromegaly were observed to be similar to those of previous studies. However, due to the inevitable nature of health insurance claims data, some of patients with acromegaly might have been omitted, which could have led to an underestimation of data. Because the HIRA database did not include individual test results such as IGF-1 or GH levels, the degree of severity could not be ascertained. To compare the complications among treatment modalities, the incidence of hypertension and diabetes was analyzed for five years in patients newly diagnosed with acromegaly during 2011–2012; however, this might not have been a sufficient period for the development of complications. The treated group would visit the hospital and have more opportunities to receive the management of their comorbidities, causing a bias that can be thought to be beneficial in their survival. However, this was also made possible by treating acromegaly, providing an additional basis for the importance of treatment. For those in the untreated group, it is not known why he/she was diagnosed but not treated. Considering the benefit of the BEP in Korea by which patients with rare and incurable disease can receive substantial financial support for their treatment, it is hardly possible to be treated without registering to the BEP. Thus, it can be guaranteed that those in the untreated group were not treated in Korea.
The annual incidence of acromegaly in Korea was similar to previously reported data. The incidence of diabetes did not significantly differ across treatment modalities, but that of hypertension was significantly lower after medical treatment. The treatment group showed significant survival benefits compared to the non-treatment group. Based on this study, we plan to expand our analysis to compare the cardiovascular outcomes between patients with acromegaly and the general population.
 XML Download
XML Download