

 PDF
PDF Citation
Citation Print
Print



The novel respiratory virus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) emerged at the end of 2019, leading to the coronavirus disease 2019 (COVID-19) pandemic worldwide. As of May 1, 2021, there had been a cumulative 150,989,419 confirmed cases, including 3,173,576 deaths globally.1 Currently, approximately 300 vaccines are under development on various platforms, with five already in the market and in phase 4. The majority of vaccines target the receptor binding domain (RBD) of the spike (S) protein of SARS-CoV-2,2345 because the virus is known to bind the receptor angiotensin-converting enzyme 2 of the host cell via the RBD of the S protein, and infects through it.67
The COVID-19 vaccine administration in Korea began on February 26, 2021 under the national vaccine project. Currently, there are two vaccines available in the country: the AstraZeneca COVID-19 vaccine inj. (adenovirus-vectored vaccine, AstraZeneca, Cambridge, UK), and the Comirnaty inj. (mRNA vaccine, Pfizer-BioNTech; Pfizer, New York, NY, USA and BioNTech, Mainz, Germany). Both vaccines require two doses; the second dose boosts the immune response.8 As of May 1, 2021, a total of 3,395,104 people received the first dose, and 236,188 people received the second dose.9
The Boramae Medical Center was designated as a COVID-19 treatment center, and vaccination of healthcare workers (HCWs) began in early March 2021. To date, 1,817 HCWs, have completed the second dose of Pfizer-BioNTech, and 350 others received the first dose of AstraZeneca. In this study, two separate blood samples from HCWs who received the second dose of the Pfizer-BioNTech vaccine were collected to evaluate the antibody production. Blood sampling was done 7 ± 2 days (1 week) and 14 ± 2 days (2 weeks) after the second dose. complete blood count (CBC; hemoglobin, white blood cells, and platelets), admission panel (blood urea nitrogen, creatinine, cholesterol, protein, albumin, bilirubin, alkaline phosphatase, aspartate transaminase, alanine aminotransferase), inflammation markers (C-reactive protein and procalcitonin), hepatitis B surface antigen/hepatitis B surface antibody, and SARS-CoV-2 antibody tests were performed. Antibody tests for SARS-CoV-2 were performed using both the automated electrochemiluminescence immunoassay (ECLIA) and the chromatographic lateral flow immunoassay (LFIA) in point-of-care testing (POCT), which are representative methods in general hospital laboratories.
A total of 289 people were enrolled in this study; however, six people did not participate in the second blood sampling, leaving only 283 blood samples in the second sampling. Demographic and basic hematologic characteristics are shown in Supplementary Table 1. Most values were within the reference ranges, with a few exceptions. Nevertheless, these out-of-range values were still not recorded critical or panic values. Therefore, all the subjects could be considered healthy adults.
The ECLIA tests were analyzed with two types of SARS-CoV-2 antibody kits using the Cobas 8000 e801 unit (Roche Diagnostics, Mannheim, Germany). The first kit was the quantitative Elecsys Anti-SARS-CoV-2 S assay (Elecsys Anti-S; Roche Diagnostics) and the second kit was the qualitative Elecsys Anti-SARS-CoV-2 assay (Elecsys Anti-N; Roche Diagnostics). The Elecsys Anti-S assay uses a recombinant protein representing the RBD of the S antigen, which favors quantitative determination of high-affinity antibodies against SARS-CoV-2.10 The Elecsys Anti-N assay uses a recombinant protein representing the nucleocapsid (N) antigen for the determination of antibodies against SARS-CoV-2.11 The clinical sensitivities (days post PCR COVID-19 confirmation ≥ 7) were 97.6% and 93.6% for anti-S and anti-N, respectively.1011 The clinical specificities were 100.0% and 99.8% for anti-S and anti-N, respectively.1011
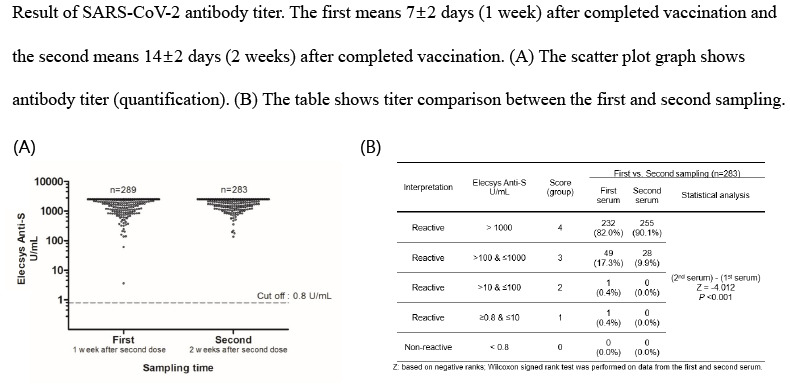
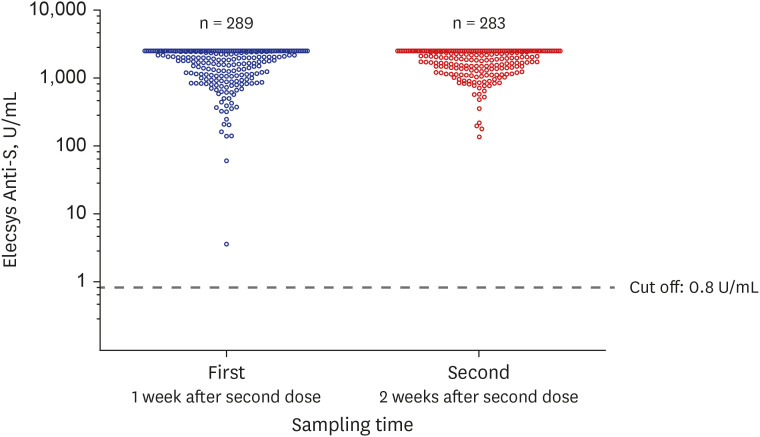
The Elecsys Anti-S results are shown in Fig. 1. The reactive (positive) value is ≥ 0.8 U/mL, and all subjects (100%; first, n = 289; second, n = 283) showed reactivity (Fig. 1); that is, antibodies to the RBD of the S protein were produced in all subjects' serum at 1 or 2 weeks after the second dose. Among them, 137 (137/289 = 47.4%) in the first sampling and 144 (144/283 = 50.9%) in the second sampling recorded excessive antibodies, exceeding the upper limits of the measurable range (2,500 U/mL). The values of Elecsys Anti-S could be divided into five groups (score 0–4) according to log10: score 0, non-reactive (< 0.8 U/mL); score 1, reactive (≥ 0.8 U/mL and ≤ 10 U/mL); score 2, reactive (> 10 U/mL and ≤100 U/mL); score 3, reactive (> 100 U/mL and ≤ 1,000 U/mL); and score 4, reactive (> 1,000 U/mL). When grouped as above and compared between the first and second serum sampling (Table 1), a significantly higher antibody titer was observed in the second sampling (P < 0.001). In the first sampling, two patients with relatively low titers (≤ 100 U/mL) did not have any specific laboratory findings. The antibodies to the RBD of the S protein were detected in all subjects; however, antibodies to the nucleocapsid (Elecsys Anti-N) were detected in only two HCWs with a history of SARS-CoV-2 infection (data not shown).
The LFIA method tests used the GeneFinder COVID-19 IgG/IgM Rapid Test (Osang Healthcare, Anyang, Korea) to detect antibodies targeting the RBD of the S protein and/or the N protein. We evaluated the clinical performance of the LFIA with 97.9% sensitivity (days from symptom onset ≥ 8) and 98.0% specificity. LFIA tests were performed with both whole blood and serum. All results were determined in the five groups by three specialized readers based on the intensity of the test line according to the reference color sheet. The results were reviewed until all the specialized readers reached agreement, and the result of the agreement was recorded as the final result (Supplementary Table 2). A total of 286 (286/289 = 99.0%) and 282 (282/283 = 99.6%) HCWs in the first and second sampling, respectively, showed positive antibody findings. There was no significant difference between whole blood and serum (P = 0.248); however, the second serum sampling showed significantly intensive signals compared to the first sampling (P < 0.001).
This study should be interpreted considering the following limitations.
First, the gold standard for quantifying soluble materials such as antibodies has been enzyme-linked immunosorbent assay (ELISA),1213 but it was not included in this study because it is difficult to implement in a general hospital laboratory setting. Nevertheless, this was not a major issue because the S protein antibodies were excessively produced in all subjects, hence leading to approximately 100% sensitivity for ECLIA and LFIA. Second, in this study, there was no significant difference between ECLIA and LFIA because of the excessive antibodies produced. ECLIA can provide a quantitative evaluation; moreover, it has higher screening power and is much more advantageous than LFIA when bulky samples are treated in a laboratory. However, because ECLIA needs an analytic equipment with a higher cost than LFIA, it is better to evaluate the advantages and disadvantages of both methods with respect to the laboratory environment.14151617 If LFIA is chosen as the main method, it is recommended that an additional, more sensitive ECLIA or ELISA method be performed when the LFIA results are negative or inconclusive (including grey zone). Third, antibody tests were not performed before vaccination and between the first and second dose. It is regrettable that if both tests were performed, it would have been possible to obtain more objective and scientific analysis by separating the first and second dose. Finally, this study evaluated the production of antibodies against the RBD of the S protein and/or the N protein of SARS-CoV-2; however, this does not fully represent the immunity of the vaccinated subjects. There is controversy as to whether these antibody titers have a positive correlation with overall adaptive humoral immunity (including neutralizing antibody titer) and adaptive cellular immunity (including T cell activity).1819202122 Therefore, complicated and expensive experiments, such as virus plaque reduction tests, cytokine quantification tests, and flow cytometry of T cell markers, are further needed to provide convincing evidence on the immunity from vaccination.
In summary, the healthy adults in our study reacted to the Pfizer-BioNTech vaccine; All participants produced SARS-CoV-2 S protein antibodies only 1 week after completion of vaccination, and the antibody titer became significantly higher a week after (i.e., 2 weeks after completion of vaccination). These results are similar to those of previous studies on the mRNA vaccine; approximately 1–2 weeks after completion of vaccination, the antibody titers were found to be high and the total vaccine efficacy exceeded 95%.2123242526 Moreover, because of the large amount of antibody formation within 2 weeks after completion of vaccination, the LFIA method also showed high sensitivity. Compared to the ECLIA test, the sensitivity reached 99.6% (based on the second sampling serum). Finally, there was no significant difference between whole blood and the serum in detecting SARS-CoV-2 antibodies after vaccination. Therefore, in a small laboratory without an ECLIA analyzer and centrifuge for serum separation, antibody formation (seroprevalence) test for vaccine efficacy could be performed using whole blood through LFIA in the POCT.
Currently, Korea is speeding up COVID-19 vaccination according to its priorities. In addition, the individual prevention and isolation guidelines for COVID-19 are being revised only for people who have completed vaccination. Despite the limitations, our findings intuitively demonstrate SARS-CoV-2 antibody formation in Korean healthy adults who have completed Pfizer-BioNTech vaccination, using the ECLIA and LFIA, which can easily be performed in a general laboratory. Therefore, it is considered useful for future policy decisions regarding vaccination.

 XML Download
XML Download