

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The introduction of biosimilar tumor necrosis factor inhibitors (TNFis) made an effective and lower-cost treatment option available for patients with inflammatory arthritis.12 Biosimilar TNFis were first approved for the treatment of rheumatoid arthritis (RA) by the European Medicines Agency in 2013 and the United States Food and Drug Administration in 2016. In Korea, an infliximab biosimilar was approved for RA treatment in 2012 ahead of both Europe and the US. Furthermore, biosimilars can be successfully extrapolated and used for any indication of their originator TNFis.
Recently updated European League Against Rheumatism guidelines for the management of RA recommend that biosimilars be considered as equivalent to their originators.3 The lower costs of biosimilars compared to their originators were expected to increase accessibility to biologic disease modifying anti-rheumatic drugs (bDMARDs) and to improve the health care outcomes of patients with RA.4 However, there is great diversity of thought regarding whether the introduction of biosimilars has actually resulted in economic savings in terms of drug prices or medical costs for patients with inflammatory arthritis, that would allow more patients to access bDMARDs.
In the European Economic Area, biosimilar competition has already reduced average list prices and increased accessibility to bDMARDs for patients.5 A previous study in six central eastern European countries predicted that the introduction of the infliximab biosimilar for Crohn's disease would bring substantial cost savings or would increase the number of patients with access to biologics therapy.6 Meanwhile, recent US studies have shown biosimilars to have low uptake78 owing to several reasons, including the absence of automatic substitution, not being included in formularies, and rebate traps, where manufacturers can withdraw substantial bio-originator drug discounts (up to 50%) if the payer uses biosimilars.9
The introduction of biosimilars in Korea may have affected the use of bDMARDs and drug prices differently compared to other countries. The Korean national regulation concerning biosimilars has distinctive points: the national insurance system is a single-payer system like that of Europe, and the national reimbursement guidelines for patients with rheumatic diseases consider biosimilars to be equivalent to their originators,10 as in the US. This system has led in clinical practice to the choice between biosimilar and originator being made by patients and physicians. A previous study using the Korean National Sample Cohort database showed that the infliximab biosimilar reduced direct medical costs for both patients and the payer during the early period of its introduction, between 2011 and 2014.11 However, another study suggested that the factors affecting the use of biosimilars rather than the originators differ in patients with RA versus those with ankylosing spondylitis.12 This difference of preference for biosimilars according to diseases can affect utilization of bDMARDs.
We aimed to examine the uptake of biosimilar TNFis in the treatment of patients RA and its economic implications for healthcare expenditure in Korea.
METHODS
Data source
All Koreans are eligible for coverage under the National Health Insurance Program. Health insurance is a single-payer system managed by the Health Insurance Review and Assessment (HIRA) and the National Health Insurance Service (NHIS).13 A total of 50 million individuals are included in the Korean HIRA or NHIS database.13 HIRA has developed a patient database using stratified random samples comprising 3% of the total population. Based on data from 2011, 1,375,842 patients were included in this HIRA-National Patient Sample (NPS) database.14 The database contains individual beneficiary information in addition to healthcare service information such as diagnoses, procedures, prescriptions, and tests. We used the HIRA-NPS between 2009 and 2018.
Study design
We extracted patients with RA with claims for bDMARDs between 2009 and 2018. We divided the bDMARDs into two groups: a TNFi group including etanercept, infliximab, adalimumab, and golimumab, and a non-TNFi group including tocilizumab and abatacept that had been approved for the treatment of RA in Korea.
Changes in the proportion of each agent among bDMARDs users were presented. Then we analyzed the market share of biosimilars on the utilization of bDMARDs. To evaluate the economic implications of the introduction of biosimilars on the medical cost of bDMARDs, overall medical costs for each patient were calculated by summing the cost of the physician examination, test, and medications in the claims for bDMARDs. Overall trends of medical costs per patient for each bDMARD were presented for 10 years.
Based on the data policy of the Korean NHIS, we hid the brand name of each drug. The dates of approval of each drug in Korea are given in Supplementary Table 1.
Statistical analysis
Descriptive statistics were used to describe the number of patients treated with bDMARDs half-yearly. We calculated the proportion of users of each bDMARD among total patients with bDMARDs between 2009 and 2018 and expressed their longitudinal changes in percentage. The medical costs per patient for each agent were expressed in Korean won and calculated by dividing the overall medical costs by the number of patients. All analyses were performed using SAS 9.2 (SAS Institute, Cary, NC, USA).
Ethics statement
This study was determined to be exempt from Institutional Review Board (IRB) review by Hanyang University Hospital IRB (IRB, file No. HYUH 2019-01-011) because we used existing, publicly available data, and the subjects could not be identified directly or through identifiers linked to them.
RESULTS
Changes in the patterns of bDMARDs use for RA between 2009 and 2018
From 2009 to 2018, between 1.4% and 1.7% (18,707 in 2009 to 24,811 in 2018) of patients with diagnostic codes of RA were extracted from the sample populations, which ranged in number from 1.38 million in 2009 to 1.48 million in 2018.
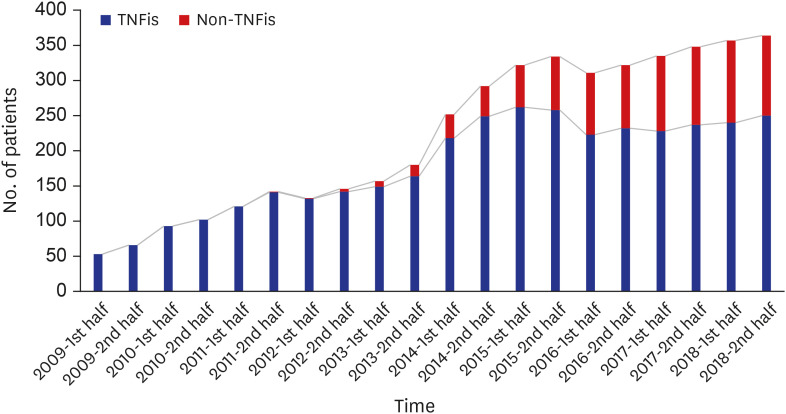
Compared to the first half of 2009 (n = 53), the number of bDMARD users increased almost seven-fold by the second half of 2018 (n = 354). The use of TNFi has been steadily increasing since 2009 and abruptly increased from 2014 to 2015. Since the approval of non-TNFis in 2011, their use rapidly increased until 2016 (Fig. 1). After 2016, the use of TNFis and non-TNFis tended to increase gradually to a similar degree.
Fig. 1
Utilization of TNFis and non-TNFis in rheumatoid arthritis patients between 2009 and 2018.
TNFi = tumor necrosis factor inhibitor.
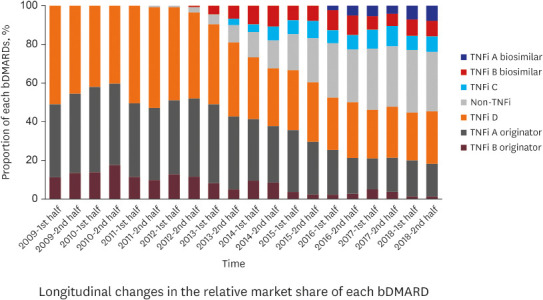
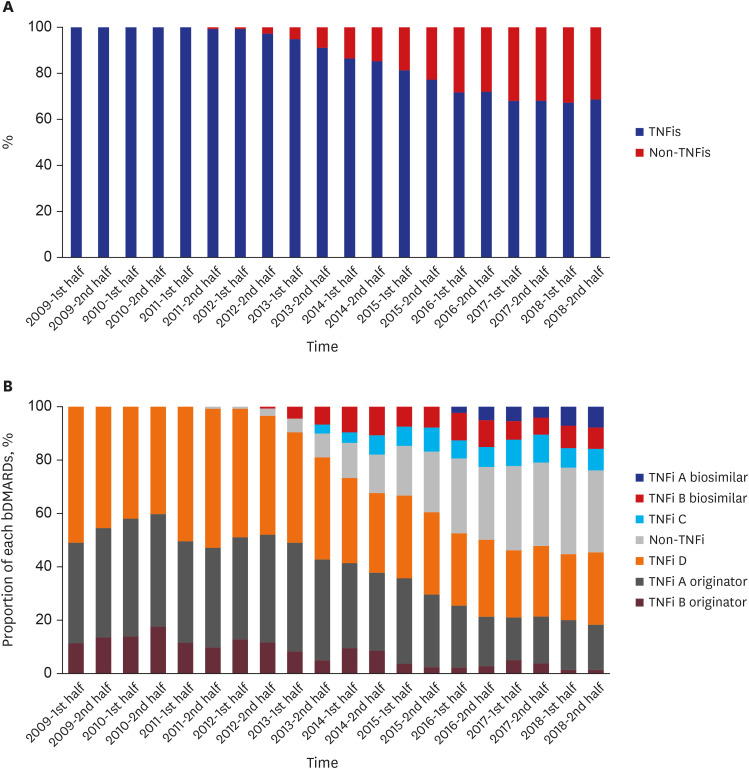
Since the introduction of biosimilar TNFis in 2012, the proportion of their use among all bDMARDs increased to 15.8% through 2018. When we expressed the use of non-TNFis as a percentage, it increased to 31.3% through 2018 (Fig. 2A). Along with the gradual increase in the use of biosimilar TNFis, that of the corresponding originator drugs has decreased, while the use of other TNFis appears to be maintained (Fig. 2B).
Uptake of biosimilar and originator TNFis for patients with RA
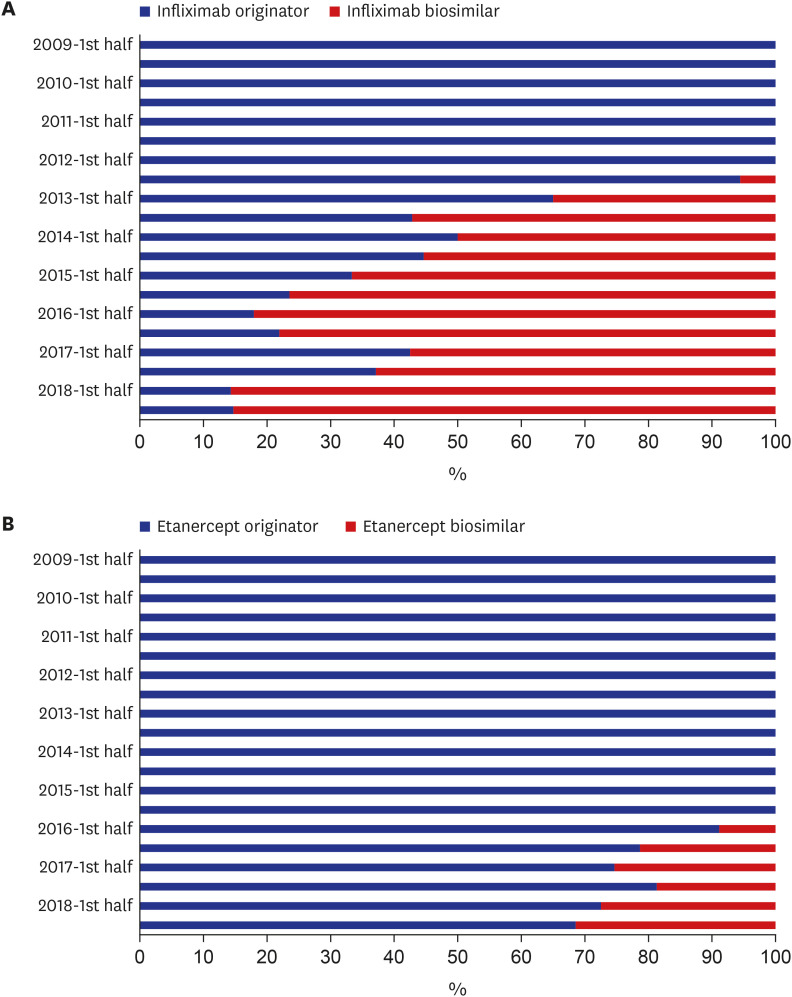
Infliximab biosimilar accounted for 35.0% of the market share in the first half of 2013 and rapidly increased to 85.3% in the second half of 2018. Etanercept biosimilar, however, which accounted for 8.9% in the first half of 2016, increased to 31.5% in the second half of 2018, showing a more modest increase in market share than did the infliximab biosimilar (Fig. 3).
Changes in annual medical costs per patient with RA using bDMARDs
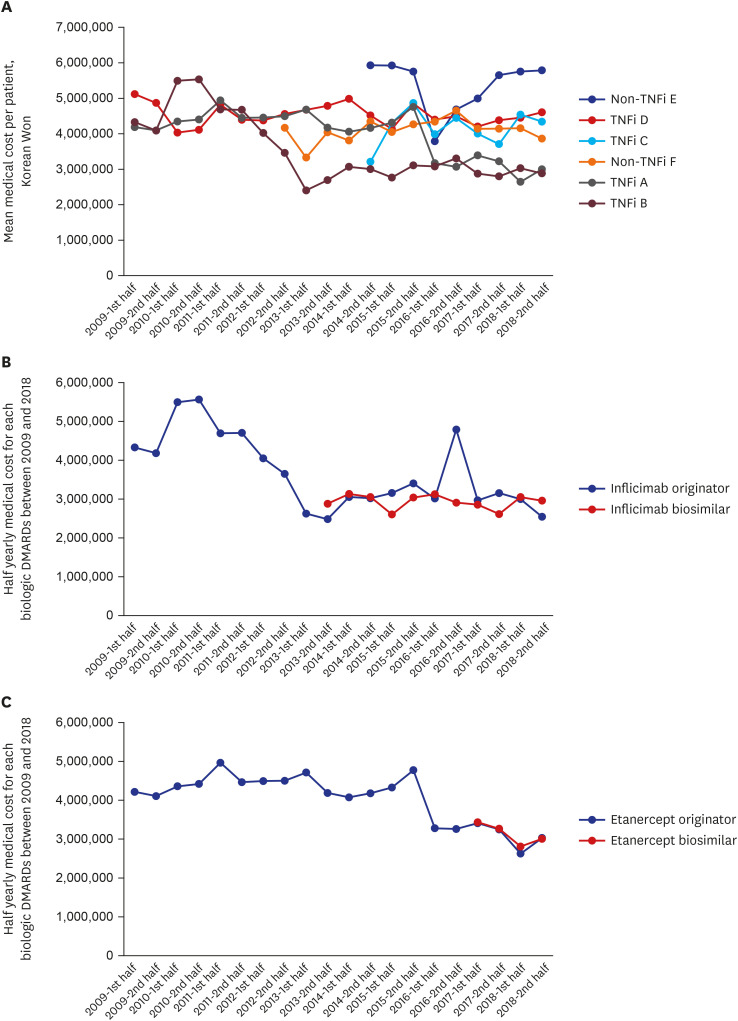
The mean half-year's medical expenses per bDMARD-treated patient gradually increased from 2009 to 2018 for two TNFis (TNFi C and TNFi D) and two non-TNFis (non-TNFi E and non-TNFi F), those for which the patents had not yet expired. However, two TNFis that have corresponding biosimilars (TNFi A and TNFi B) showed decreasing medical costs (Fig. 4A). Shortly before the introduction of biosimilars, the medical costs of the patients who used their originators were reduced. However, after the introduction of the biosimilars, the medical costs of RA patients tended to be maintained. The medical costs of biosimilar users were not different from those of the originator users (Fig. 4B and C).
Fig. 4
Longitudinal changes in the per patient medical costs for users of (A) bDMARDs, (B) infliximab, and (C) etanercept between 2009 and 2018.
TNFi = tumor necrosis factor inhibitor, bDMARD = biologic disease modifying anti-rheumatic drug.
Among the total medical costs, the proportion of drug costs was lower in the infliximab biosimilar group compared to the infliximab originator group. However, for etanercept, the proportion of drug costs among the total medical costs was comparable between the originator and biosimilar groups (Supplementary Table 2).
DISCUSSION
This study found that the prevalence of bDMARDs use in patients with RA has continuously increased over the past decade. We also observed that the use of biosimilar TNFis increased after their introduction. The uptake of biosimilars was 15.8% of the total bDMARDs used by the second half of 2018. In terms of medical cost per patient, users of infliximab or etanercept had lower costs than those of other bDMARDs. Medical costs for those patients decreased just before the introduction of biosimilars, but they have tended to maintain similar costs since then.
Utilization of bDMARDs in Korea appeared to be significantly affected by the drug approval status. The use of TNFis has been steadily increasing since 2009 but abruptly increased from 2014 to 2015. This might be related to the approvals of infliximab biosimilar in 2012 and etanercept biosimilar in 2015. Meanwhile, abatacept was first approved in 2011 as an option for patients with RA who responded inadequately to TNFis, and its indication was expanded for bDMARD-naïve patients in 2013, followed by tocilizumab. Accordingly, the use of non-TNFis, which first began in the second half of 2012, rapidly increased until 2016.
The uptake of biosimilars among bDMARDs in 2018 was 15.8% in Korea. Among all infliximab users, the proportion of biosimilar users was 85.3%, but among all etanercept users, the proportion of biosimilar users was 31.5%. This uptake of biosimilars is not so high compared to the trends in Europe, despite the fact that the approval year in Korea for biosimilars was earlier than that of Europe. In Denmark, the infliximab biosimilar constituted 90.6% of the total amount of infliximab four months following patent expiration of the bio-originator, and it led to a reduction in the medical costs by two-thirds.15 Similar results were seen for the etanercept and adalimumab biosimilars.1516 In Korea, there was no mandatory regulation for the transition to biosimilars as in Europe. Therefore, the utilization of biosimilars is decided by the preferences of the physicians or patients. The relatively low uptake of biosimilars may be related to the fact that there is little medical cost-saving of the biosimilar compared to the originator. The medical costs of originator users tend to be decreasing slightly only just before the introduction of the biosimilar. The cost savings in the originator after the introduction of TNFi biosimilar in response to the availability of less expensive biosimilar and competition between the biosimilars themselves was also shown in the UK.17 However, in Korea, the cost-saving was not much, and the medical costs of biosimilar users eventually grew to be similar to those of the originator users. Therefore, the motivation for physicians and patients to switch from originator to biosimilar could be limited, although there is evidence of similar effectiveness and safety in biosimilars compared to originators.
Another interesting point is that the introduction of biosimilars did not increase the market share of the drug as a whole. Along with the gradual increase in use of biosimilar TNFis, the use of the corresponding originator drugs has decreased, while the use of other non-TNFis or originator TNFis, whose patents have not yet expired, has increased. This indicated that the use of biosimilars is a result of switching from the corresponding originators or from starting with the biosimilar instead of its originator. This implies that biosimilars have not yet improved overall accessibility to bDMARDs for RA patients.
To maximize the benefits of biosimilars, the cooperation of multiple stakeholders is required.18 It is necessary for biosimilar drug manufacturers to demonstrate real-word evidence that the biosimilar has similar effectiveness and safety as its originator, in addition to the equivalence demonstrated in clinical trials. This may be more important for the extrapolated indications than for RA. Along with this evidence in the real world, we can carefully guess that the lower the price, the higher the preference of physicians and patients. In addition, patient understanding of biosimilars is crucial for treatment success and avoidance of nocebo effects.19 Full understanding of biosimilars by physicians and carefully considered communication strategies can help support patients when initiating or switching to biosimilars.18
This study has several strong points. First, we used the HIRA-NPS database between 2009 and 2018, which has a higher degree of external validity than single-center or multicenter cohort studies. Second, biosimilars were approved as early as 2012, and the reimbursement guidelines in Korea recommended biosimilars as equal to originators in patients with rheumatic diseases. Therefore, we were able to use long-term observational data in the real world to analyze drug utilization tendencies. Third, our data encompassed overall bDMARDs including non-TNFis. This allows us to evaluate the impact of TNFi biosimilars on non-TNFis as well as on TNFis.
However, there are also limitations associated with the HIRA-NPS data source. First, patient samples are available from 2009 to 2018, but it is not possible to follow an individual patient over the observational period, as each sample is cross-sectional, and none are linkable by individual. Second, some medical costs might be affected by the reimbursement guidelines. As shown in our study, the medical costs per patient can be high at the initial introduction of bDMARDs. This is because the Korean insurance guidelines recommend close monitoring every month during the initial 6 months, which can lead to frequent outpatient visits and performance of laboratory tests. Therefore, it is appropriate to grasp the overall trend rather than interpreting the results at one point in time, although we analyzed time according to the half-year to compensate for this potential issue. Third, we could not evaluate clinical effectiveness and safety, because our data did not include results regarding inflammatory marker or joints counts. By now, there have been several observational studies evaluating the effectiveness and persistence of infliximab biosimilars that have revealed outcomes comparable to their originators.2021 Further observational studies evaluating the effectiveness, safety, and economic benefit of biosimilar use in various patients are needed to improve our knowledge of biosimilars.22
In conclusion, the proportional use of biosimilar TNFis has increased since their introduction in Korea. The availability of less expensive biosimilar TNFis seems to bring about a decrease in medical costs for users of the originator TNFis.
 XML Download
XML Download