

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Allogeneic hematopoietic stem cell transplantation (HSCT) is a potentially curative option for various malignant and nonmalignant diseases. Among several donor options, umbilical cord blood has been emerged as an established alternative source of hematopoietic stem cells, especially for patients lacking a suitable human leukocyte antigen (HLA)-matched related or unrelated donor. Multiple studies have demonstrated similar survival in children and adults receiving cord blood transplantation (CBT) to a standard unrelated donor HSCT.123
Total body irradiation (TBI) has traditionally been included in the standard myeloablative conditioning (MAC) regimens, since it enables both irreversible elimination of malignant cells and strong immune-suppression.4 Especially in CBT, TBI has been reported to do an important role in successful neutrophil engraftment.5 However, its long-term complications have emerged as a major challenge, and no-TBI regimens were introduced and preferred by many centers.
Although conditioning regimens comprise a principal element of HSCT, studies analyzing the impact of different conditioning regimens on CBT outcomes are scarce, especially in pediatric population. Recently, a study by Eapen et al.6 demonstrated that total body irradiation 10 Gy, cyclophosphamide 120 mg/kg, and fludarabine 75 mg/m2 (TCF) regimen consisting of TBI 13.2 Gy, cyclophosphamide 120 mg/kg, and fludarabine 75 mg/m2 were associated with improved survival, compared to other regimens in CBT for children with acute leukemia. This type of TCF conditioning regimen excluded anti-thymocyte globulin (ATG).
In this study, we aimed to identify the impact of conditioning regimens on the outcome of CBT in children with acute leukemia, by comparing outcomes of the TCF with 10 Gy TBI versus non-TCF regimens.
METHODS
Study population
A retrospective chart review was performed on patients with acute leukemia who received CBT between 2002 and 2015, at Samsung Medical Center. The subjects were retrospectively identified through a survey of our institutional database. All patients were diagnosed with acute leukemia and were candidates for allogeneic HSCT. CBT was performed if no suitable HLA-matched related or unrelated donor was available. Patients who had received prior allogeneic transplantation were excluded. Before March 2005, the HLA disparity between the recipient and the graft was determined at the 6-loci antigen level only (i.e., HLA-A, HLA-B, and HLA-DR). After March 2005, the cord blood grafts were matched with at least 4–6 HLA-A and HLA-B at antigen level and HLA-DRB1 at the allele level to the recipient. When two cord blood units were transplanted, transplantation was performed in the same level of match between each unit. Double unit CBT was performed in patients who lack a single cord blood unit with adequate cell dose. All patients received MAC regimens, either TBI-based or intravenous busulfan-based.7 The type of conditioning regimens was selected based on the patient's diagnosis, disease status, and the availability of drugs and TBI. TBI to a total dose of 10 Gy in 3 daily fractions was given (3.33 Gy/day for 3 days). Busulfan was given intravenously at a dose of 3.2 mg/kg/day for 4 days. ATG (Thymoglobulin; Genzyme, Cambridge, MA, USA) was administered at a dose of 2.5 mg/kg for 3 consecutive days. Graft-versus-host disease (GVHD) prophylaxis consisted of cyclosporin A combined with mycophenolate mofetil or methylprednisolone. All patients received antimicrobial prophylaxis with acyclovir and micafungin.
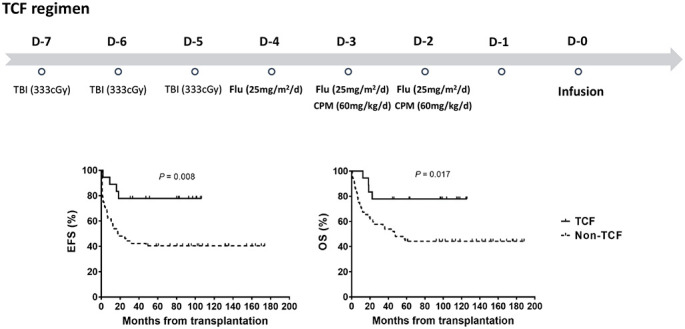
Patients were allocated into 2 groups; the TCF and the non-TCF group. The TCF group included patients conditioned with the TCF regimen, while the non-TCF group included those who received MAC regimens other than the TCF regimen. For TCF regimen, TBI 10 Gy was given as 3.33 Gy/day (without fractionation) for 3 days (d-7 to d-5), cyclophosphamide 60 mg/kg/day for 2 days (d-3, d-2), and fludarabine 25 mg/m2/day for 3 days (d-4 to d-2). The conditioning regimen was mainly TCF in AML after 2008, but other regimens which exclude TBI were selected in patients under 2 years of age. In the case of ALL, TCF has been used as the main conditioning regimen since 2013.
Definitions
Neutrophil engraftment was defined as the first of three consecutive days for absolute neutrophil count greater than 0.5 × 109/L. For post-transplant monitoring of donor engraftment, chimerism testing was routinely performed on peripheral blood and bone marrow samples, via polymerase chain reaction amplification of short tandem repeat loci. Mixed chimerism was defined as the presence of ≥ 1% recipient-derived cells. Diagnosis and grading for acute GVHD was based on the standard criteria. Cytomegalovirus (CMV) disease was defined as a positive CMV antigenemia assay and any of the following: the presence of relevant symptoms, signs, the presence of retinitis on ophthalmologic examination, or a tissue biopsy specimen that was CMV positive by either culture or immunohistochemical staining.89 Non-relapse mortality (NRM) was defined as death from any cause other than disease relapse or progression. Overall survival (OS) was calculated from the date of transplant to death from any cause or last contact if the patient remained alive. Event-free survival (EFS) was calculated from the date of transplant to the date of relapse or progression, graft failure, death, or last contact if the patient remained event-free.
Statistical analysis
Patient and transplant characteristics of the 2 groups were compared using the χ2 test or the Fisher's exact test for the categorical variables. Continuous variables were compared using the Student's t-test or Mann-Whitney U test. The 5-year probabilities of EFS and OS were estimated by the Kaplan-Meier method, and univariate comparisons between survival curves were performed using the log-rank test. All statistical analyses were performed by R version 3.6.1 and SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). A P value < 0.05 was considered statistically significant.
RESULTS
Patient and transplant characteristics
A total of 71 patients were included in this study. Tables 1 and 2 illustrates the characteristics of these 71 patients (46 males and 25 females). The TCF group included 18 patients and the non-TCF group included 53 patients. The median age and body weight of the total patients at the time of CBT were 7.3 years (range, 0.6–18.5) and 26.0 kg (range, 6.2–72.0), respectively. The median numbers of infused total nucleated cells (TNCs) and CD34+ cells were 4.4 × 107/kg (range, 1.2–13.2) and 1.6 × 105/kg (range 0.5-8.3), respectively. In terms of the median age (P = 0.810), body weight (P = 0.413), and numbers of infused TNCs (P = 0.084) and CD34+ cells (P = 0.078), no significant differences were noted between the 2 groups. The proportion of the types of leukemia was also not statistically different between the 2 groups (P = 0.088). Of the total 71 patients, 48 (67.6%) were in CR1 at transplant. There was no significant difference between the 2 groups in the disease status at transplant (P = 0.904).
Table 1
Patient and transplant characteristics
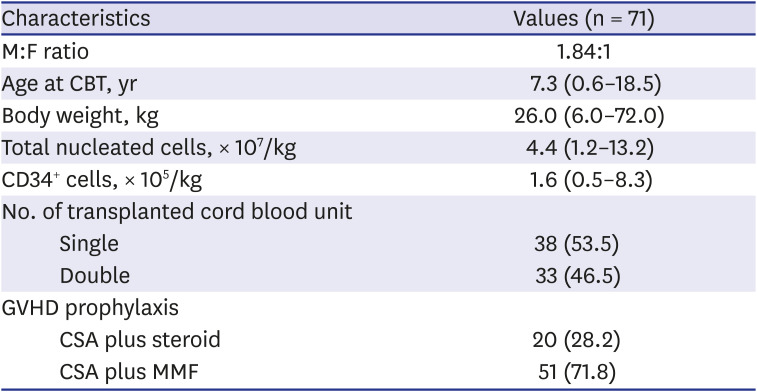
Table 2
Patient and transplantation characteristics according to treatment group
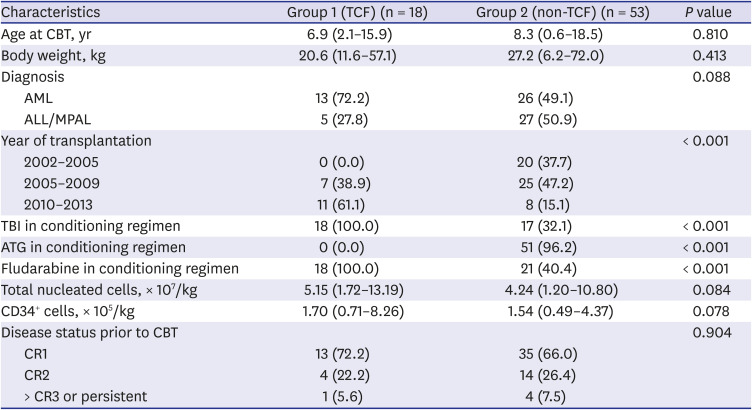
Values are presented as median (range) or number (%).
TCF = total body irradiation 10 Gy, cyclophosphamide 120 mg/kg, and fludarabine 75 mg/m2, CBT = cord blood transplantation, AML = acute myelogenous leukemia, ALL = acute lymphoblastic leukemia, MPAL = mixed-phenotype acute leukemia, TBI = total body irradiation, ATG = anti-thymocyte globulin, CR = complete remission.
Marked differences were noted in the composition of conditioning regimens. All patients in the TCF group used TBI, while 17 (32.1%) out of 53 patients in the non-TCF group included TBI in their conditioning regimen (P < 0.001). No patient (0%) in the TCF group used ATG, while 51 (96.2%) of 53 patients in the non-TCF group included ATG in their conditioning regimens (P < 0.001).
Patients' outcomes
Engraftment
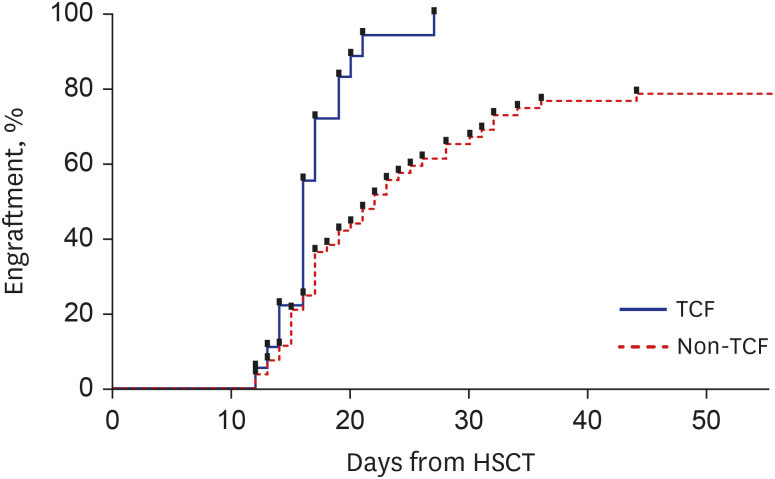
The median time to neutrophil engraftment was 17 days (range, 12–44) for the total patients, 16 days (range, 12–27) for the TCF group, and 18 days (range, 12–44) for the non-TCF group. Compared to the non-TCF group, the probability of neutrophil recovery was significantly higher in the TCF group (P = 0.014) (Fig. 1). Whereas all patients in TCF group achieved donor-origin hematopoiesis, 12 patients among 53 patients (22.6%) in non-TCF group failed, resulting in significant difference (P = 0.029). In the non-TCF group, causes of failure to achieve donor-origin hematopoiesis included early transplant-related mortality (n = 4), primary (n = 6) or secondary (n = 1) graft failure, and autologous recovery (n = 1).
GVHD
In the TCF group, grade II to IV and grade III to IV acute GVHD occurred in 15 (83.3%) and 3 (16.7%) patients, respectively. In the non-TCF group, grade II to IV and grade III to IV acute GVHD occurred in 25 (47.2%) and 6 (11.3%) patients, respectively. With regard to the incidences of grade II to IV acute GVHD, patients in the TCF group experienced a significantly higher incidence of grade II to IV acute GVHD (P = 0.003). However, when compared in terms of the incidence of grade III to IV acute GVHD, no significant difference was noted between the two groups (P = 0.236) (Table 3). Cumulative incidence of chronic GVHD was 83.3% (15 of 18 patients) in the TCF group and 43.6% (23 of 53 patients) in the non-TCF group (P < 0.001).

CMV antigenemia and CMV diseases
In terms of the incidence of CMV antigenemia, no statistical differences were noted between the TCF (61.1%) and non-TCF (60.4%) groups (P = 0.956). However, CMV diseases occurred in 1 patient (5.6%) in the TCF group and 16 patients (30.2%) in the non-TCF group, demonstrating a significantly lower incidence of CMV diseases in the TCF group (P = 0.029).
Early bloodstream bacterial infection
Early bloodstream bacterial infection in the first 30 days occurred in 6 among 18 patients (33.3%) in the TCF group and 19 of 53 patients (35.8%) in the non-TCF group, with no significant difference (P = 0.862).
Survival, NRM and relapse
The median follow-up period of the total survivors was 117 months (range, 45-188). The 5-year EFS and OS of the total 71 patients were 49.8% and 52.5%, respectively. Among the TCF group, 4 out of 18 patients died at the time of analysis; 3 died of relapse after CBT, and 1 died of transplant-related mortality (infection and grade IV acute GVHD). Among the non-TCF group, 30 out of 53 patients died; 15 died of relapse, and 15 died of non-relapse causes, most of which were transplant-related mortality. The 5-year EFS for patients in the TCF and non-TCF groups were 77.8% and 40.4%, respectively (**P = 0.008) (Fig. 2A). The 5-year OS in the TCF and non-TCF group were 77.8% and 44.2%, respectively (*P = 0.017) (Fig. 2B), demonstrating significantly higher survival rates in the TCF group.
Fig. 2
Comparison of 5-year survival rates of the 2 groups. (A) The 5-year EFS. (B) The 5-year OS.
EFS = event-free survival, TCF = total body irradiation 10 Gy, cyclophosphamide 120 mg/kg, and fludarabine 75 mg/m2, OS = overall survival.
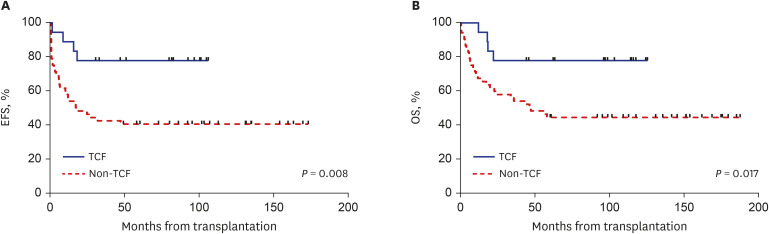
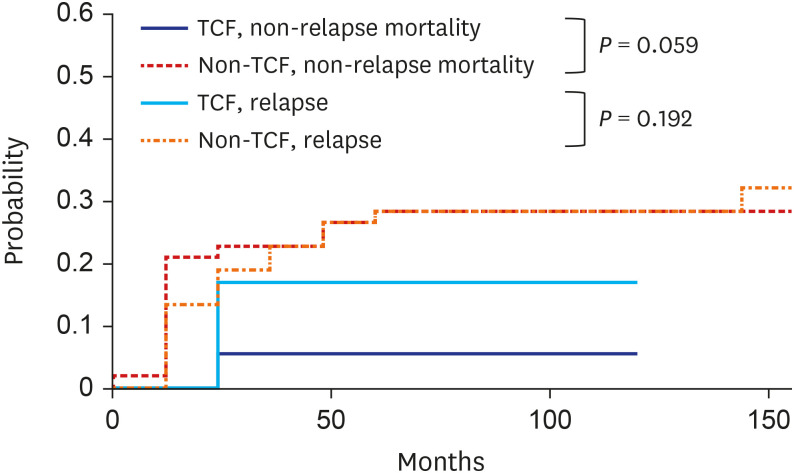
The cumulative incidences of relapse at 5 years were 16.7% (95% confidence interval [CI], 3.8% to 37.2%) for the TCF group and 28.3% (95% CI, 16.8% to 40.9%) for the non-TCF group, with no significant difference between the 2 groups (P = 0.192). Meanwhile, the cumulative incidences of 5-year NRM were 5.6% (95% CI, 3.8% to 37.2%) for the TCF group and 28.3% (95% CI, 16.9% to 40.9%) for the non-TCF group (P = 0.059) (Fig. 3).
Survival according to the use or non-use of TBI and ATG
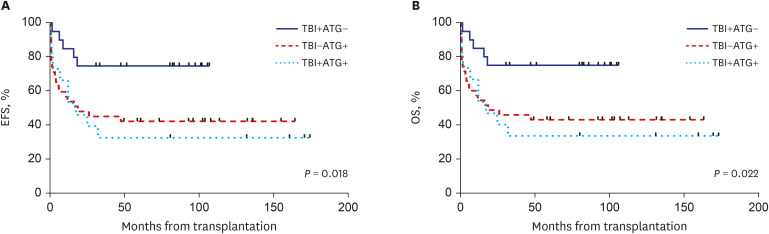
To determine the outcome of each treatment methods, 71 patients were additionally divided into 3 groups according to the use of TBI and ATG. Group 1 included patients who received TBI, but not ATG (TBI+ ATG−), group 2 included those who received ATG, but not TBI (TBI− ATG+), and group 3 included those who received both TBI and ATG (TBI+ ATG+).
The 5-year EFS for patients in group 1 (n = 20), 2 (n = 36) and 3 (n = 15) was 75.0%, 42.9% and 33.3%, respectively. In survival comparisons, the 5-year EFS in group 1 was significantly higher than in groups 2 and 3 (P = 0.018) (Fig. 4A). The 5-year OS in group 1 was also significantly higher than in groups 2 and 3: the 5-year OS for patients in group 1, 2 and 3 was 79.7%, 48.4% and 33.3% (P = 0.022) (Fig. 4B).
DISCUSSION
CBT offers a chance of cure for patients with serious hematological malignancies, especially for those who lack suitable donors. Since CBT is characterized by a relatively lower cell dose and less stringent HLA matching criteria,1011 graft failure and delayed immune recovery are of major concern.121314151617 Conditioning regimens can have a substantial impact on the overall outcomes, but in most centers, the choice of conditioning regimen has been mainly based on experts' opinion, rather than universal criteria. A desirable MAC regimen should exert potent antitumor activity and sufficient immunosuppression, while avoiding excessive toxicity. In this study, we introduce a modified type of TCF regimen consisting of myeloablative TBI (10 Gy), cyclophosphamide (120 mg/kg) and fludarabine (75 mg/m2).
In this study, better survival outcomes were observed in patients conditioned with the TCF regimen, compared to the non-TCF regimen, in line with previous study be Eapen and collegues.6 The TCF group showed a higher probability of neutrophil recovery, a higher rate of achieving donor-origin hematopoiesis, a lower rate of CMV diseases, and higher 5-year OS and EFS. Because of the limited number of patients, statistical significance in relapse rate and NRM was not observed. But borderline trend of lower TRM incidence in TCF group was observed (P = 0.059).
TBI has been the traditional backbone of MAC regimen. Especially in the setting of CBT, several studies highlight the role of TBI. According to a Japanese registry-based study, neutrophil engraftment was superior in the TBI group regardless of the conditioning regimen, even in the presence of HLA mismatch or anti-HLA antibodies.5 This finding may indicate the potent immunosuppressive role of TBI in the milieu of an active immune interaction between donor and recipient. In addition, a part of data by Eapen et al.6 suggested the role of TBI in reducing leukemia recurrence. A significant higher relapse risk was observed in patients with non-trial, chemotherapy-only conditioning regimens, suggesting potent antitumor activity of TBI.
Nevertheless, TBI is avoided by many centers nowadays, owing to its various toxicities and the need for special facilities. Especially in children, there is a great concern about the late effects of radiation therapy. Of note, the major distinction between our TCF regimen and that used in the study by Eapen et al.6 is the dose of TBI. While a total of 13.2 Gy TBI was uniformly used both in trial- (BMT CTN 0501) and non-trial-based setting in the study by Eapen et al.,6 our strategy was to reduce the dose of TBI by 10 Gy.
Range of TBI practices are applied with a common target dose of 12 to 13.2 Gy in 6 to 8 fractions.18 However, due to the lack of resources, it was difficult to fractionate radiation therapy in our center. Because it was difficult to reduce the dose per fraction, limiting the total cumulative radiation dose to 10 Gy was necessary to prevent excessive toxicity. Despite discrepancies in patient numbers, our study demonstrated a comparable outcome to that reported from BMT CTN 0501; the 5-year OS of patients enrolled in the BMT CTN 0501 trial was 70%,6 while the 5-year OS of our TCF group patients was 77.8%. Considering the need for a less-toxic MAC regimen in CBT, reducing the dose of TBI may help reducing regimen-related toxicities in pediatric patients, while maintaining antitumor activity and myeloablative property. Given the outcome was satisfactory with TCF regimen containing 10 Gy TBI, our study suggests that TCF regimens with 10 Gy TBI could serve as a realistic alternative in areas with limited resources. In the future, late effects of patients who underwent CBT with 10 Gy of TBI should also be investigated.
Another major difference between the TCF and non-TCF group in this study was the use of ATG. The TCF group uniformly omitted ATG and showed better 5-year EFS and OS compared to the non-TCF group. In the 3-group analysis, group 1 (TBI+ ATG−) showed the highest 5-year EFS and OS as well. ATG has been shown to reduce the risk of graft failure and GVHD in allogeneic HSCT,19 but the use of ATG prior to CBT is an ongoing debate nowadays. While delayed immune recovery is an inherent property of CBT, ATG tends to aggravate this phenomenon, as demonstrated by several other reports.202122 The non-TCF group showed slower neutrophil recovery, a lower rate of donor-origin hematopoiesis, and a higher incidence of CMV diseases. Our study showed that group 3 (TBI+ ATG+) resulted in the lowest survival rate with high relapse rate. ATG has an immunomodulation effect on T lymphocytes, B lymphocytes, as well as dendritic cells.23 The level of antigen exposure is increased after TBI, which may enforce the immunomodulation effect of ATG. As a result, the graft-versus-leukemia effect may decrease and disease relapse may increase. The results of this study suggest that ATG should not be administered when using TBI as conditioning regimen.
Notably, the TCF group in this study showed a significantly lower incidence of CMV diseases, and this may be closely associated with the omission of ATG. Due to a high CMV seropositivity (94.1%) among Koreans in all population,24 most donors and recipients are seropositive (D+/R+) in Korea. Indeed, the incidence of CMV antigenemia was even higher in this study exceeding 60% in both TCF and non-TCF groups. Herein lies the clinical significance of the lower incidence of CMV diseases, especially in regions with high CMV seroprevalence, such as Korea.
In this study, a higher incidence of grade II to IV acute GHVD was observed in patients conditioned with the TCF regimen, and this can also be ascribed to the omission of ATG. However, no significant difference was observed in terms of grade III to IV acute GVHD, and even better survival outcomes were observed in the TCF group. Lindemans et al.22 also showed that without ATG, the incidence of NRM was not high even though the acute GVHD incidence was high. Altogether, these findings may suggest that the benefit of a rapid engraftment and immune recovery outweighs the harm associated with acute GVHD.
This study has several limitations, including its retrospective nature. In our institution, as in many CBT-performing centers, the choice of conditioning regimens was largely based on clinical factors and experts' experience. Moreover, since many patients in the TCF group were transplanted in more recent years, better supportive care in these patients may have affected the outcomes. The difference in treatment era and number of patients between both groups could have affected the difference in treatment outcomes. Nonetheless, this study is valuable in that it compared conditioning regimens in a relatively large number of pediatric patients undergoing CBT.
Overall, our findings demonstrated that children conditioned with myeloablative TBI (10 Gy), cyclophosphamide (120 mg/kg), fludarabine (75 mg/m2) and omitting ATG achieved better engraftment and survival rates, while less suffering from CMV diseases. We suggest that our modified type of TCF regimen can be a preferred option for pediatric patients with acute leukemia undergoing CBT.
 XML Download
XML Download