

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Entecavir (ETV) and tenofovir disoproxil fumarate (TDF) are equally recommended first-line drugs for chronic hepatitis B.123 A recent large-scale retrospective cohort study of patients who had started treatment with ETV or TDF between 2012 and 2014 reported that TDF was superior to ETV in reducing the risk of hepatocellular carcinoma (HCC),4 in contrast to other studies that did not observe significant differences.56789 ETV and TDF were introduced in Korea in January 2007 and December 2012, respectively. Due to the differences in drug approval, the 2012–2014 cohort produced a disparity between the ETV and TDF groups regarding index dates and follow-up periods.4 Patients in the TDF group had started antiviral treatments after December 2012 at the earliest, whereas patients in the ETV group had already been enrolled in 2012. Therefore, the TDF and ETV groups of the 2012–2014 cohort differed regarding the start date of antiviral treatments and follow-up duration. We thus hypothesized that the differences in HCC risk and incidence were due to differences in index dates and follow-up periods between the two treatments. To test this, we conducted a cohort study with matched the index dates of the two treatments and extended the enrollment and follow-up periods among the treatment-naïve chronic hepatitis B patients. In addition, we used a cohort similar to that used in a previous study4 (patients who had started antiviral drugs in 2012–2014 and did not match the index date) for comparison with other cohorts.
METHODS
Data source and study cohort
Insurance claim data were obtained from the Korean Health Insurance Review and Assessment Service (HIRA) database. We used two cohorts of patients treated with ETV or TDF using data of treatment-naïve adults aged between 20 and 79 years who had started antiviral therapy with ETV (0.5 mg/day) or TDF (300 mg/day) between January 2013 and December 2017. We excluded patients who 1) received both ETV and TDF during 2007–2018, 2) received other anti-hepatitis B drugs (lamivudine, clevudine, telbivudine, adefovir, ETV (1.0 mg), tenofovir alafenamide fumarate, or besifovir) during 2007–2018, 3) were administered ETV or TDF for fewer than 180 days during 2013–2018; 4) were diagnosed with cancer before ETV or TDF treatment, 5) were diagnosed with human immunodeficiency virus infection during 2007–2018, or 6) died from or were diagnosed with cancer within 180 days after treatment initiation. The second cohort (2012–2014 cohort) was compiled using the same inclusion and exclusion criteria except for enrollment period (January 2012 to December 2014). We collected data on treatment-naïve adults aged between 20 and 79 years who had started antiviral therapy with ETV (0.5 mg/day) or TDF (300 mg/day) between January 2012 and December 2014. We excluded patients who: 1) received both ETV and TDF during 2007–2018, 2) received other anti-hepatitis B drugs (lamivudine, clevudine, telbivudine, adefovir, ETV (1.0 mg), tenofovir alafenamide fumarate, or besifovir) during 2007–2018, 3) were administered ETV or TDF for fewer than 180 days during 2013–2018; 4) were diagnosed with cancer before ETV or TDF treatment, 5) were diagnosed with human immunodeficiency virus infection during 2007–2018, or 6) died from or were diagnosed with cancer within 180 days after treatment initiation.
Matching
Main cohort (cohort 1): we matched the ETV and TDF groups at a 1:2 ratio based on age (five-year intervals), sex, comorbidities (cirrhosis, diabetes, hypertension, and chronic obstructive pulmonary disease) at baseline (defined as the first prescription of an antiviral agent), hospital type (clinic vs. hospital) at baseline, and year of index date. Comorbidities were defined according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes. ICD-10 codes or drug codes associated with the examined variables are listed in Supplementary Table 1.
2012–2014 cohort (cohort 2): each group was matched at a 1:1 ratio based on age, sex, comorbidities at baseline, and hospital type at baseline. However, the year of the index date was not matched in the 2012–2014 cohort (Supplementary Fig. 1).
Outcome and follow up
The development of HCC was considered the outcome. The index date was the date on which the patient was first prescribed ETV or TDF. Patients were followed up until December 31, 2018. As with the main cohort, the 2012–2014 cohort was followed up until December 31, 2018.
Subgroup analyses
Subgroup analyses were conducted based on sex (male and female), age (20–49 and 50–79 years), hospital type at baseline (clinic and hospital), and presence of cirrhosis.
Ethics statement
Claims data was provided by the HIRA, and the identities of patients remained concealed. This study was approved by the Institutional Review Board of the HIRA (approval number: B2019-025), which waived the need for informed patient consent. The study protocol was consistent with the ethical guidelines of the 1975 Declaration of Helsinki. Both authors had access to the study data and reviewed and approved the final manuscript.
Statistical analyses
Categorical and continuous variables were compared using χ2 and t-tests, respectively. Incidences rates are presented as events per 100 person-years (PY) of observation, and 95% confidence intervals (95% CIs) were estimated assuming a Poisson probability distribution. Cox proportional hazard models were used to calculate hazard ratios (HRs) with 95% CIs. All statistical analyses were performed using R software, version 3.5.0 (R Foundation Inc.; http://cran.r-project.org). Statistical significance is reported at P values < 0.05.
RESULTS
Study population
The study population included 76,285 treatment-naïve patients treated with ETV (n = 21,486) or TDF (n = 54,799) (Fig. 1). After matching, the ETV and the TDF groups comprised 18,491 and 36,982 patients, respectively. Baseline characteristics of the completed and the 1:2 matched cohorts are shown in Table 1.
Fig. 1
Flow diagram of the study population in matched set.
ETV = entecavir, TDF = tenofovir disoproxil fumarate, COPD = chronic obstructive pulmonary disease.
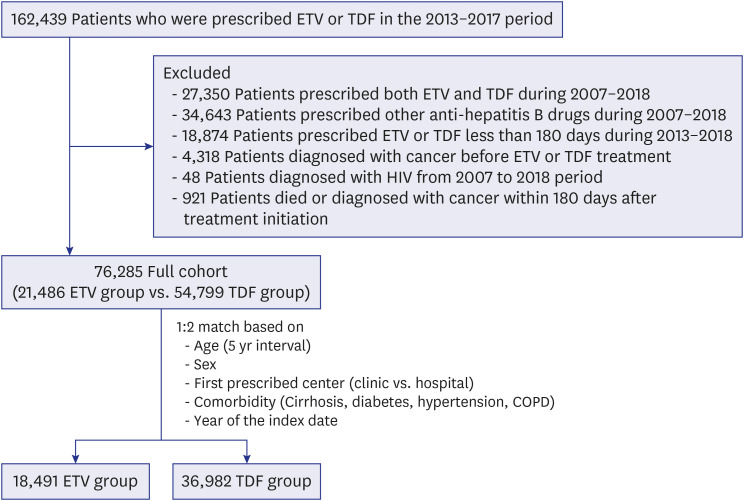
Table 1
Baseline characteristics of patients treated with tenofovir versus entecavir
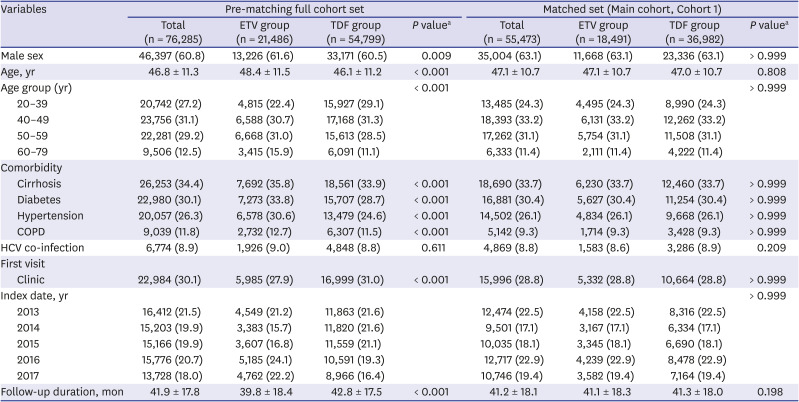
Data are presented as number (%) or mean ± standard deviation. The main cohort groups were matched for age (five-year intervals), sex, comorbidities, hospital type at baseline, and year of the index date.
ETV = entecavir, TDF = tenofovir disoproxil fumarate, COPD = chronic obstructive pulmonary disease, HCV = hepatitis C virus.
aP values were calculated using χ2 tests for categorical variables and t-tests for continuous variables.
Clinical outcome in the main cohort
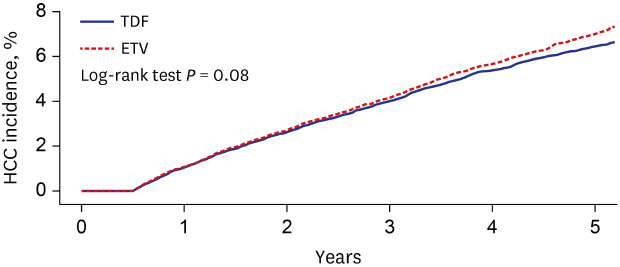
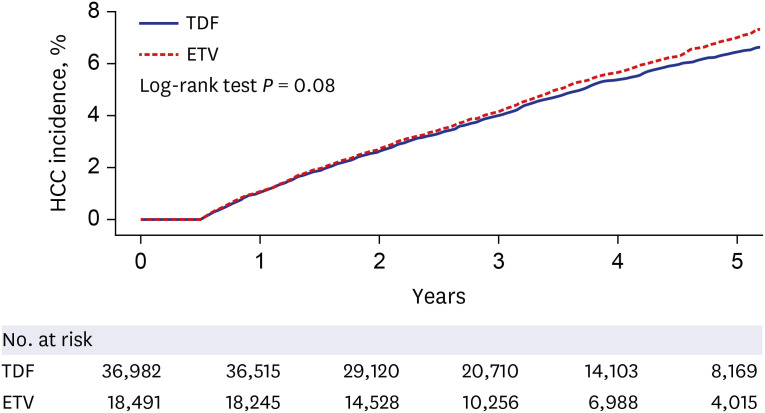
The patient data showed a mean follow-up time of 41.2 months (Table 1). During follow-up, a total of 912 patients in the ETV group (4.9%) and 1,708 in the TDF group (4.6%) developed HCC; however, a significant difference in HCC incidence between the treatment groups were not observed (1.46 per 100 PY vs. 1.36 per 100 PY; HR, 0.93; 95% CI, 0.86–1.01; P = 0.081) (Table 2, Fig. 2).
Table 2
Subgroup analysis of hepatocellular carcinoma stratified according to sex, age, hospital type, and presence of liver cirrhosis at baseline in cohort 1
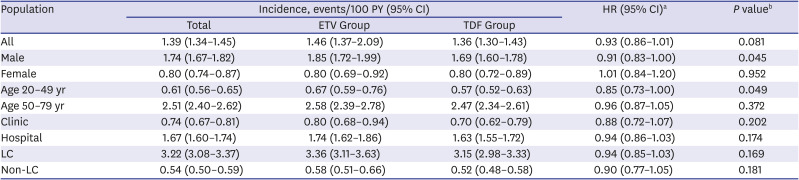
PY = patient-years, ETV = entecavir, TDF = tenofovir disoproxil fumarate, HR = hazard ratio, CI = confidence interval, LC = liver cirrhosis.
aHazard ratios are given for the excess risk of each outcome among patients treated with TDF, as compared to matched patients treated with ETV; b
P values were calculated using a Cox proportional hazard model.
Subgroup analyses
HCC incidence did not differ between subgroups based on hospital type and presence of cirrhosis (Table 2). However, differences seen in the male subgroup and the younger age group were statistically significant (HR, 0.91; 95% CI, 0.83–1.00, P = 0.045; HR, 0.85; 95% CI, 0.73–1.00; P = 0.049).
Clinical outcome in the 2012–2014 cohort (Cohort 2)
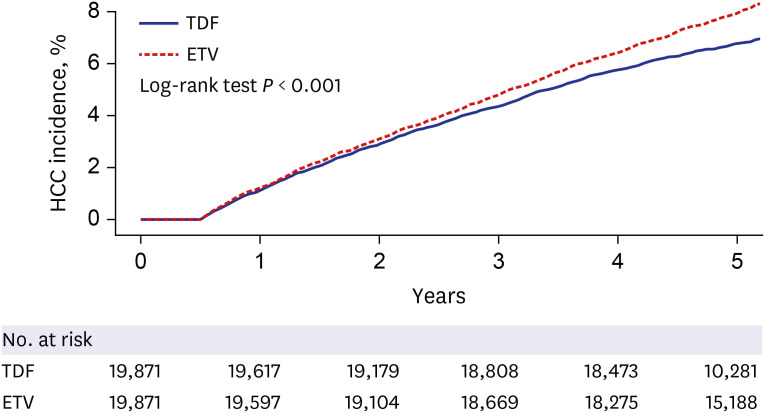
The 2012–2014 cohort included 19,871 matched pairs (Table 3, Supplementary Fig. 1). The proportions of index years per group differed. The follow-up duration was significantly longer for the ETV group than for the TDF group (68.5 ± 16.5 vs. 58.7 ± 12.1; P < 0.001). Unlike the results in the main cohort, the incidence of HCC was significantly lower in the TDF group than in the ETV group (1.42 per 100 PY vs. 1.66 per 100 PY; HR, 0.85; 95% CI, 0.79–0.91; P < 0.001; Fig. 3).
Table 3
Baseline characteristics and hazard ratios of the 2012–2014 cohort (Cohort 2)
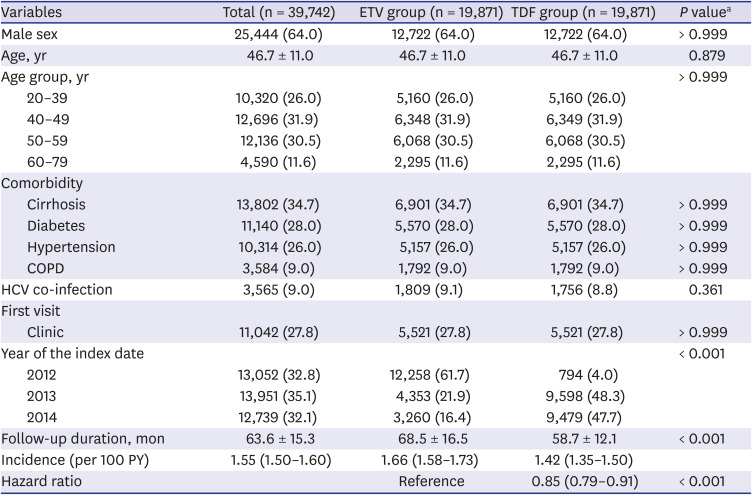
Data are presented as number (%) or mean ± standard deviation.
Groups were matched for age (five-year interval), sex, comorbidities, and hospital characteristics at baseline.
ETV = entecavir, TDF = tenofovir disoproxil fumarate, COPD = chronic obstructive pulmonary disease, HCV = hepatitis C virus, PY = person year.
aP values were calculated using a χ2 test for categorical variables and a t-test for continuous variables.
DISCUSSION
In a nationwide retrospective cohort study, we analyzed 55,488 cases treated with ETV or TDF. To our knowledge, this is the largest study comparing ETV and TDF treatment using long-term follow-up data. Moreover, we extracted all cases treated with ETV or TDF in Korea from 2013 through 2017 using national insurance claims with all Koreans as compulsory beneficiaries. Therefore, the findings of the present study show real-world evidence in the Korean population.
ETV and TDF have similar safety and efficacy for viral suppression,1011 and both are recommended first-line antiviral therapies.123 However, potential differences in HCC incidence between ETV and TDF are controversial.456789121314 Recently, two studies reported a lower risk of HCC development in TDF-treated patients than in ETV-treated patients in Korea4 and Hong Kong,12 whereas other studies founded no differences.567891314 Even meta-analyses on this issue came to contradictory conclusions.151617 Increased risk of HCC may be an important consideration when choosing an antiviral agent. Given the inherent limitations of observational data, these conflicting results of previous studies should be cautiously interpreted. A previous study in Korea4 reporting an increased risk of HCC incidence with ETV has been recognized for its robustness through a wide variety of analytic and validation methods with hospital-based cohort data. We assumed that uncontrolled variables related to the index dates or follow-up periods of the two drugs may affect HCC incidence results in a nationwide cohort study.4 As expected, our study showed a 15% reduction in the risk of HCC in the TDF group compared to that in the ETV group in the 2012–2014 cohort, similar to the cohort of the previous study of Choi et al.4 However, the incidence and risk of HCC did not differ significantly between the two groups in the main cohort analysis matched for the index year. These results are consistent with those of a recent meta-analysis showing that the differences in follow-up duration between the ETV and TDF groups can affect the results and are generally biased towards treatments with shorter follow-up duration.16 In the 2012–2014 cohort of this study, which was designed similarly to the study of Choi et al.,4 the numbers of at-risk patients sharply decreased only in the TDF group compared to the ETV group at the fifth year (Fig. 3). This is because many cases of TDF started late and the observation period was short. This supports our assumption that differences in follow-up duration contributed differences in HCC incidence.
The second reason for these differences may be due to differences in the population included in the study. A study by Choi et al.4 used the National Health Insurance Service (NHIS) claims data that includes periodic general health examination data of all insured individuals. Therefore, the data includes healthcare use, health screening, socio-demographic variables, and mortality of the entire Korean population.18 By contrast, HIRA data do not include records from laboratories, health-affecting behavior, such as smoking, drinking, and diet, and health examination records.19 The number of patients in this study was higher than that in a previous study using NHIS data by Choi et al.4 This is because the previous study dataset included only those who had a general medical examination, while our study further included all insured individuals who had never had a general medical examination. Moreover, the proportion of underlying diseases, such as hypertension (7.8% vs. 26.3%), diabetes (6.3% vs. 30.1%), and liver cirrhosis (26.8% vs. 34.4%), was higher in our study than that in the study using NHIS data. We propose that this reflects the differences between the population segment undergoing medical examinations and the general population. As expected, there is a trade-off between the types of data. NHIS claims data have the advantage that the data contains detailed laboratory results or socioeconomic variables; however, it excludes the population segment that has not undergone general health examination.
Among the male and younger subgroups, the TDF group showed lower HCC risk than the ETV group, although the CIs were close to 1.0. We did not find any other similar indications or reports of superior effects of TDF in the younger group and male subgroups. One possible cause may be the influence of several confounding variables that were not controlled in this study, such as alcohol, Child-Pugh score, or other comorbidities. Particularly, males have higher rates of alcohol intake and smoking than females, and these factors were not sufficiently controlled. Therefore, the superior effect of TDF in the male subgroup needs to be cautiously interpreted. Second, TDF may be preferred in young women of childbearing age for safety of pregnancy,20 which may have caused bias in subgroup analysis.
Even though we attempted to overcome the inherent limitations of observational studies by matching, clinical data associated with other comorbidities and data regarding disease severity were lacking. We thus could not assess clinical information, such as laboratory results, due to the limitations of insurance claims data. Laboratory information, such as viral load, HBeAg status, and hepatitis B virus genotype are important risk factors for HCC. The variables used in our study were not sufficiently controlled; we were not able to assess socioeconomic status, lifestyle factors such as smoking and alcohol consumption, and family history of HCC.
We presumed that the selection of antiviral agents was performed as recommended in the guidelines; however, we cannot exclude biases regarding drug selection according to a practitioner's preferences or due to unassessed comorbidities of individual patients such as renal disease.2122 While this confounding bias may have occurred in the present study, we expected it to be negligible. According to the WHO guidelines, avoidance of TDF and use of ETV instead, or dose reduction of TDF should be considered for patients with baseline estimated glomerular filtration rates < 50 mL/min or in those at risk factors for renal insufficiency.22 However, TDF is not contraindicated in patients with renal disease, and a recent meta-analysis reported negligible differences between TDF and ETV regarding renal dysfunction.23
In addition to the effects on HCC, there have been many studies comparing the effects of tenofovir and ETV.5810112324 A meta-analysis that compared the efficacy of tenofovir and ETV suggested that tenofovir is better at virus inhibition in the early stage; ETV is superior in protecting liver function in the early stage, but its therapeutic effect is similar in the long term.24 Conflicting reports on HCC incidence have been reported, but there are consistently no differences between the two drugs for other outcomes such as death or liver transplantation.5813 Among studies in the Korean population, the studies based on hospital data showed no difference between the two drugs on HCC incidence,5813 while a study based on claims data reported higher HCC incidence in the ETV group.4 Although the result is limited to the male and younger subgroups, the incidence of HCC in the TDF group was lower than the ETV group in this study. Therefore, the possibility that this difference may be due to the bias cause by limitations of claims data should also be considered.
Our study did not produce any evidence that ETV treatment was inferior to TDF treatment for the prevention of HCC. We suggest that the index date and follow-up period may be residual confounding factors when comparing ETV and TDF. Therefore, to compare the effect of ETV and TDF treatment on HCC incidence, the index date and follow-up period should be controlled. Additional studies with in-depth analyses of clinical, socioeconomic, and lifestyle data are needed to further confirm our results.
 XML Download
XML Download