

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Smoking is a risk factor for many diseases including cancer, cardio-cerebrovascular and respiratory tract diseases.1 In February 2005, the World Health Organization declared the Framework Convention on Tobacco Control (FCTC) for promotion of public health against tobacco epidemic.2 Overall, 181 countries signed the FCTC and are implementing the stipulated tobacco control policies in the treaty. One of the main policies in the FCTC is the recommendation of no smoking in public areas and indoors because second-hand smoke (SHS) is strongly associated with disease and death.3
Globally, 40% of children, 33% of non-smoking men, and 35% of non-smoking women are exposed to SHS.4 Fortunately, in Korea, SHS exposure has continuously declined since 2012 when smoking was banned in all public areas. However, while the overall smoking and SHS rates have continuously declined among adults, the smoking rates in adolescents have started to increase again since 2016 in Korea.5 Such increase can lead to an increase in the risk of SHS among adolescents, particularly through school-level factors and peer groups.6
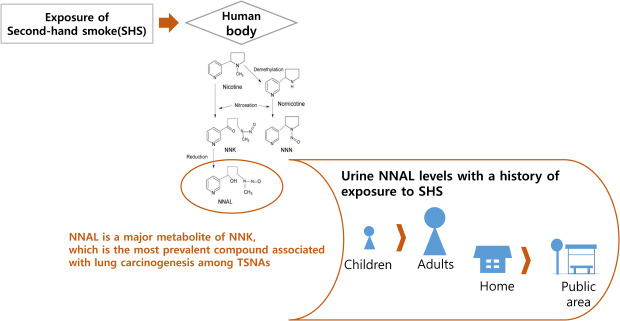
Tobacco-specific nitrosamines (TSNAs) are one of many carcinogens related with smoking. Among TSNAs, 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK) is the compound most associated with lung cancer and other smoking-related cancers. Accordingly, it was classified as a group 1 carcinogen by the International Agency for Research on Cancer (IARC) in 2007. The 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) is a biomarker for assessing the extent of exposure to NNK.7 Previous studies showed that NNAL is detected in both smokers and non-smokers exposed to SHS.89 In a US study, NNAL was detected in 55% of the total participants, 41% of whom were non-smokers.10 Particularly, NNAL levels among non-smoker children were significantly higher than those of adults aged over 20 years.10 Considering that NNAL is a biomarker of the NNK classified as carcinogen, these findings indicate the potential of NNAL as a predictor of SHS-related disease. More than 39% of adolescents were reported to be exposed to SHS in Korea based on their parents' questionnaires.11
As such, we aimed to investigate the association between SHS exposure and urine NNAL levels in Korean adolescents, using the data from the Korea National Health and Nutrition Examination Survey (KNHANES) VII.
METHODS
Study design and population
We used data from the KNHANES VII in 2016 to 2017. The KNHANES is comprised of three parts: health survey, health check-up including laboratory tests, and nutrition surveys. The data from the KNHANES include information such as socioeconomic status, education, alcohol, smoking, and anthropometric measurements. In total, 16,277 participants were included in the 2016-2017 survey. Of them, we initially selected 3,377 participants aged 18 years or younger. Then, 2,729 participants were excluded according to the following criteria: 1) age 6 years or younger because their SHS exposure was not investigated (n = 1,012); 2) no laboratory data on NNAL (n = 765); 3) participants aged 12 years or younger who did not respond to the assessment of tobacco smoking status (n = 863); and 4) currently smoking or had previously smoked tobacco (n = 89). Finally, 648 never-smoking adolescents aged 12 to 18 years were evaluated (Supplementary Fig. 1).
They were divided into two groups according to SHS exposure. No exposure was defined as never exposed to smoking both at home and in public areas, while exposure was defined as exposure to smoking at home or in public areas.
Variables
We assumed age, body mass index (BMI), white blood cell (WBC) count, high sensitivity c-reactive protein (hs-CRP), hemoglobin, monthly household income, and physical activity as relevant confounding variables in determining the association between SHS and urine NNAL level. BMI (kg/m2) was calculated by dividing the weight (kg) by the square of the height (m). The WBC count and hemoglobin were measured via flow cytometry using semiconductor laser and SLS hemoglobin detection method, respectively, by XN-9000 (Sysmex, Kobe, Japan). The other laboratory test, hs-CRP, was measured by immunoturbidimetry using cobas® (Roche, Hamburg, Germany). Monthly household income was estimated based on a family member's response to the survey. Physical activity was defined according to the practice of the recommended physical activity of children and adolescents.12 Adequate physical activity was defined as performing aerobic exercises above moderate intensity more than 1 hour daily and more than three times weekly (≥ 180 minutes per week) or muscle-strengthening activities more than three times weekly. Urine NNAL (ng/mL) levels were measured by high-performance liquid chromatography/mass spectrometry using Agilent 1200 Series with Triple Quadrupole 5500 (AB Sciex, Framingham, MA, USA). Separated weight was given because sampling examinations have been conducted on some of the participants aged over 6 years. The cut-off points of elevated urine NNAL level, which was determined to have the highest Youden index among values that satisfy more than 50% of both sensitivity and specificity, was 1.78 (sensitivity, 58.2%; specificity, 66.3%) and 2.01 ng/mL (sensitivity, 50.6%; specificity, 86.6%) in men and women, respectively. Normal urine NNAL levels were set as < 1.78 and < 2.01 ng/mL in men and women, whereas elevated urine NNAL levels were set as ≥ 1.78 and ≥ 2.01 ng/mL, respectively.
Statistical analysis
Considering the sample design of the KNHANES, we conducted a complex sample analysis that weighted and designated variables of cluster and stratification. Intergroup-differences between the unexposed and exposed SHS groups were evaluated using the independent t-test for continuous variables and the χ2 test for categorical variables. The cut-off points of elevated urine NNAL level were calculated using receiver operating characteristic (ROC) curve and Youden index. The risk for elevated urine NNAL levels was expressed as odds ratios (ORs) and their 95% confidential intervals (CIs), calculated using logistic regression models after applying sampling weight. The models were adjusted for confounding factors as follows: model 1, not adjusted; model 2, adjusted for age and BMI; and model 3, adjusted for age, BMI, WBC, hs-CRP, hemoglobin, monthly household income, and physical activity. All statistical analyses were performed using SPSS® statistics version 20 (IBM®, Armonk, NY, USA). P values < 0.05 were considered statistically significant.
RESULTS
In total, 425 boys and 223 girls (mean age, 15.0 years for both sexes) were included. Of them, 223 (34.4%; 134 boys, 31.5%; 89 girls, 39.9%) have history of SHS exposure. Table 1 shows the characteristics of the study participants by sex. With respect to exposure by location, 74 participants experienced exposure at home, whereas 193 participants experienced exposure in public areas.
Table 1
Participant characteristics according to sex

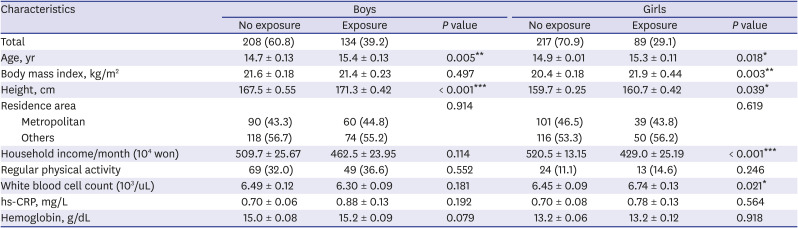
Table 2 presents the participants’ characteristics according to SHS exposure by sex. The male and female participants in the exposure groups were older and taller than their counterparts in the no exposure groups. Among girls, the exposure group had higher BMI and lower monthly household income than did the no exposure group (P < 0.05). The WBC levels were also higher in the female exposure group than in the female no exposure group.
Table 2
Participant characteristics according to exposure to SHS by sex
The mean urine NNAL levels in the no exposure and exposure group by sex are presented by geometric mean in Fig. 1. In boys, the mean urine NNAL levels of the no exposure and exposure group were 1.39 and 2.26 ng/mL, respectively, whereas they were 1.01 and 2.45 ng/mL, respectively, in girls (P < 0.001).
Fig. 1
NNAL levels according to exposure to second-hand smoke by sex.
NNAL = 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol.
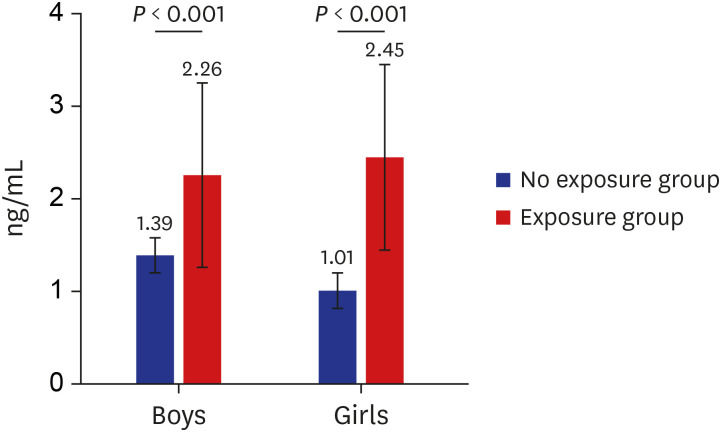
Fig. 2 shows the mean urine NNAL levels according to exposure area by sex. Among the participants exposed to SHS in homes, there were significant differences in the mean urine NNAL levels between the no exposure and exposure group in both boys (1.51 vs. 5.63 ng/mL, P < 0.001) and girls (1.68 vs. 4.67 ng/mL, P < 0.001). In contrast, both boys and girls showed no significant difference in the mean urine NNAL levels between the no exposure and exposure group among those exposed to SHS in public places (boys: 2.24 ng/mL vs. 1.96 ng/mL, P = 0.375; girls: 1.85 ng/mL vs. 2.23 ng/mL, P = 0.429).
Fig. 2
NNAL levels according to exposure area by sex.
NNAL = 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol.
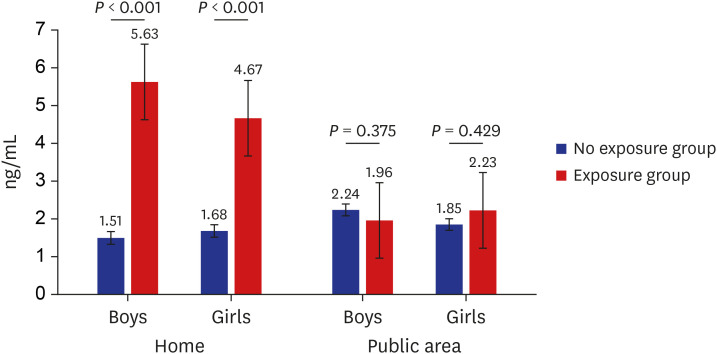
Table 3 shows the ORs (95% CIs) for elevated urine NNAL level by weighted logistic regression analysis. Unadjusted ORs (95% CIs) for elevated urine NNAL level by overall exposure and areas of exposure as home and public area were 2.44 (1.47–4.05), 19.93 (6.23–63.80), and 1.73 (1.06–2.83) in boys; and 5.73 (2.96–11.08), 10.45 (4.09–26.70), and 4.17 (2.14–8.11) in girls, respectively (model 1). The ORs (95% CIs) for elevated NNAL level by overall exposure and by areas of exposure as home, and public area were 2.68 (1.58–4.53), 31.02 (9.46–101.74), and 1.89 (1.12–3.17) in boys; and 6.50 (3.22–13.11), 20.09 (7.08–57.04), and 3.94 (1.98–7.77) in girls, respectively after adjusting for age, BMI, WBC, hs-CRP, hemoglobin, monthly household income, and physical activity (model 3).
Table 3
OR for elevated urine NNAL level according to sex and SHS exposure area

Data presented as OR (95% confidence interval), and ORs are calculated using weighted logistic regression analysis.
Cut-off points for elevated urine NNAL are 1.78 and 2.01 ng/mL in boys and girls, respectively. Elevated urine NNAL level was defined as values greater than the cut-off point.
Model 1: not adjusted; Model 2: adjusted for age and body mass index; Model 3: adjusted for age, body mass index, white blood cell counts, high sensitivity C-reactive protein, hemoglobin, monthly household income, and physical activity.
NNAL = 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol, SHS = second-hand smoke, OR = odds ratio.
DISCUSSION
NNAL levels of children with a history of exposure to SHS are higher than those of adults, and a high number of adolescents are exposed to SHS in Korea. The results of this study showed that exposure to SHS is significantly associated with elevated urine NNAL levels in Korean adolescents. With respect to exposure by location, exposure was greater in public areas than that in homes; however, NNAL levels were higher among participants with home exposure.
Several studies have attempted to indirectly present scientific evidence using biomarker that SHS exposure in children and adolescents increases the risk of smoking-related diseases. Kalkbrenner et al.13 conducted the study using serum and hair cotinine, known as major nicotine metabolites, as biomarkers for SHS exposure evaluated. In their study of elementary school aged asthmatic children living with smokers, the longer the parents smoke at home or the higher the number of cigarettes smoked at home, the higher the level of serum and hair cotinine. Ino et al.14 screened SHS exposure in elementary school children of Kumagaya City, Japan, using urinary cotinine as a biomarker for SHS exposure. Tobacco smoking of parents, particularly of mothers, was positively correlated with the urinary cotinine level.14 Similarly, Vardavas et al.15 used serum nicotine and cotinine as biomarkers for SHS exposure in Greek adolescents, and they found that most adolescents were exposed to SHS even when their parents were non-smokers.
Cotinine was mostly used as a biomarker for SHS. Cotinine is quantitatively the most important metabolite of nicotine, and about 70% to 80% of nicotine is converted to cotinine by the liver enzyme cytochrome P450 2A6.1617 Nicotine has a half-life of two hours, whereas cotinine has a half-life of 16 hours and is eliminated within three to four days from the last exposure. Thus, cotinine is relatively stable.18 For these reasons, cotinine has been widely used as a biomarker for studies on SHS exposure in children and adolescents, as in the studies above.
Among the many diseases related with SHS exposure, cancer is the most serious. The IARC has identified more than 60 carcinogens related to tobacco smoking, 15 of which are classified as group 1 (i.e., carcinogenic to humans).19 The association between SHS exposure and cancer risk in children has been identified in several studies. Using data from National Cancer Institute-Maryland Lung Cancer study and Mayo Clinic study, Olivo-Marston et al.20 showed that childhood SHS exposure increases the risk of adult lung cancer, including in never smokers. Further, those with childhood SHS exposure were younger at the time of diagnosis. Bjerregaard et al.21 also reported that SHS exposure during childhood increases the risk of bladder cancer, while no association was identified for SHS exposure during adulthood.
Tobacco smoking has many related carcinogens, and SHS exposure in children increases the risk of cancer and several respiratory diseases. However, nicotine and cotinine, the biomarkers widely used to identify the risk of SHS exposure, are not considered smoking-related carcinogens but a simple metabolite of nicotine.22 Another tobacco-specific biomarker with adequate sensitivity and specificity in assessing SHS exposure and has proven carcinogenicity in humans is NNAL.8 NNAL is a major metabolite of NNK, which is the most prevalent compound associated with lung carcinogenesis among TSNAs.23 NNK is formed by nitrosation of nicotine or related minor alkaloid during tobacco curing and burning process.24 NNK absorbed into the body is rapidly converted to NNAL by carbonyl reductases and 11β-hydroxysteroid dehydrogenase type 1.25 During α-hydroxylation of NNAL by cytochrome P450, diazonium ions are produced.26 Then, when diazonium ions bind with aldehyde, it produces DNA adducts. DNA adducts play an important role in carcinogenesis associated with smoking.23 If the DNA adducts are not repaired and replication continues, it causes miscoding and results in permanent mutation of the DNA sequence. If mutations occur in certain areas of important genes, such as RAS, MYC, TP53, and if these mutated cells are not removed by apoptosis, it leads to tumor development.26
Also, NNAL has a relatively long elimination half-life of 10–18 days, longer than the 16-hour half-life of cotinine.27 Moreover, the concentration of nicotine decreases rapidly due to its absorption in the surrounding environment, whereas the level of NNK increases with the longer duration of SHS exposure.28 As such, NNAL, as a metabolite of NNK, may be more useful than cotinine, as a metabolite of nicotine, to determine the health impact of long-term smoke exposure. However, there are relatively fewer studies on NNAL as a biomarker of SHS exposure in children and adolescents than studies on cotinine. Chao et al.29 reported that NNAL is advantageous for assessing smoke exposure. They showed that although the urinary cotinine levels were similar in adults and children exposed to SHS, urinary NNAL levels were significantly higher in children than those in adults.
Few studies on SHS exposure and biomarkers in Korean children and adolescents have been conducted to date. Lee et al.30 evaluated the degree and characteristics of SHS exposure using urinary cotinine levels for non-smoking Korean adolescents. They reported that low positive rates of urine cotinine in Korean adolescents and that SHS-related characteristics do not affect the positive rate of urine cotinine.
To our best knowledge, there has been no previous study that used NNAL as a biomarker of SHS exposure in children and adolescents in Korea, thus making this the first one on NNAL. Further, the findings of this study were based on data from the KNHANES, a population-based survey, and applied a complex sample design to evaluate individuals representative of the Korean population.
Despite these strengths, there are several limitations in this study. First, a larger-scale study could not be carried out because the urine NNAL test was performed only in select survey participants. Another limitation associated with this result is the wide confidence interval due to the small number of samples.31 Particularly, this limitation was most remarkable in the home exposure group ORs. Second, not all non-smoking adolescents may have been identified because smoking status was self-reported. Third, there was no detailed breakdown of the exposure site, and thus a detailed analysis of the exposure outside the home was not conducted. Fourth, this study did not include quantitative data to show the association of urine NNAL level with the amount of exposure. Fifth, in the home exposure group, further analysis related to the family members of the participants could not be made. Unfortunately, we could not obtain direct information on whether parents smoked or not, and which family members smoked at home.
In conclusion, SHS exposure is significantly associated with elevated urine NNAL level in Korean adolescents, particularly in female adolescents and in those with home exposure. Considering carcinogenicity of NNAL, this study is meaningful in that it reminds community members, including parents who smoke at home, about personal behavior change and the necessity of tobacco legislation for protecting adolescents from SHS exposure.
 XML Download
XML Download