

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Panic disorder (PD) is a severe and persistent mental disorder, associated with high levels of subjective suffering, occupational and social disabilities.12 PD is characterized by a sudden and recurring surge in anxiety known as panic attacks as well as anxiety over panic attacks and avoidance of potential future panic attacks. In the United States, the prevalence of PD in the general population has been estimated to be 3%–5%,3 and the recent rise in cases over the past few years has increased the number of individuals negatively impacted by this condition. According to Korea's National Health Insurance Service, the number of patients with PD is increasing every year. Among them, the number of patients in their 20s more than doubled from 7,848 in 2014 to 18,851 in 2018—an average increase of 24.5 percent per year. The increasing number of patients diagnosed with PD and the growing awareness of the disease suggest that more active therapeutic intervention is becoming increasingly important.
Many studies have identified a higher incidence of comorbid mental disorders in patients with PD, especially anxiety, mood and substance use disorder.456 Several studies also examined the role of panic attacks as a key psychopathologic phenomenon in many mental disorders.789 In patients with PD, co-existence of other mental disorders is of considerable importance because of its high prevalence and its association with the severity and chronicity of PD; these factors greatly impact a patients' quality of life. Importantly, depression is one of the most common comorbid mental illnesses in patients with PD, an observation that holds high clinical importance since depression is highly associated with suicide. Therefore, to improve the prognosis of patients with PD, it seems very important to better understand the factors impacting the occurrence and deterioration of depression in these patients.
Many factors contribute to the occurrence and deterioration of depression in patients with PD. For instance, insomnia has been shown to be highly associated with the severity of symptoms in patients with PD,10 and it is said to sustain panic symptoms for a long time. Importantly, sleep disorders as a whole can worsen depression and suicidal behavior.11 At some level, PD, insomnia, and depression interact with each other and lead to continued disease progression.12 Given the potential effect that breaking this vicious cycle may have on improved prognosis, this study aimed to identify the mediating effect of insomnia on the occurrence and deterioration of depression in patients with PD.
METHODS
Participants
A retrospective review of available electronic medical records from consecutive patients with diagnosed PD was conducted. The patients who visited an outpatient clinic between October 2018 and December 2019, and were diagnosed as having a PD were included in this study. The diagnosis of PD was made by the clinician based on The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). The patients who were under 18 years old were excluded. Individuals with comorbid anxiety disorders or depression and personality disorders were included, but only if PD was judged to be the primary diagnosis. Patients with other major psychiatric disorder or neurological disorders were not included. A total of 110 participants met the inclusion criteria and were included in the statistical analyses. All data were deidentified and analyzed anonymously.
Measures
The PD Severity Scale (PDSS)
The PDSS measures all PD dimensions, including panic attack, anticipatory anxiety, panic-related phobias, wellness, severity of all symptoms, and impairment.1314 The PDSS is a 7-item self-report scale of PD symptoms (e.g., “During the past week, how much have you worried or felt anxious about when your next panic attack would occur or about fears related to attacks?”).15 Items are rated using a 5-point Likert scale ranging from 0 (none) to 4 (extreme). The Korean PDSS demonstrated good reliability and was satisfactory in a previous study.16
The Beck Depression Inventory-II (BDI-II)
The BDI is a 21-item questionnaire designed to assess the degree of depressive symptoms that appeared in the prior two weeks from time of administration. Each item is rated on a 4-point Likert scale ranging from 0 to 3; its total score ranges from 0 to 63, with higher scores indicating more severe depressive symptom. The BDI was originally developed by Beck et al.17 in 1961 and revised to BDI-II in 1996 in response to changes in the DSM-5 criteria for the diagnosis of depressive symptom. The psychometric properties of the BDI-II among the Korean adolescents showed good internal consistency (Cronbach's alpha = 0.89) and strong concurrent validity with the Patient Health Questionnaire-9 (r = 0.75).18
The Insomnia Severity Index (ISI)
The ISI is a brief self-report questionnaire that measures the patient’s perception of insomnia severity.19 The Korean version of the ISI was used to assess for sleep disturbance in the Korean population and shown to be a reliable and valid assessment tool.20 It consists of 7 questions described as follows: 1) Difficulty in falling asleep; 2) Difficulty in staying asleep; 3) Problems on waking up too early; 4) How satisfied are you with your current sleep pattern?; 5) How noticeable to others do you think your sleep problem is in terms of impairing the quality of your life?; 6) How worried are you about your current sleep problem?; 7) To what extent do you consider your sleep problem to interfere with your daily functioning currently? Each question is rated using a 5-point Likert scale scored from 0 to 4 (e.g., 0 = no problem; 4 = very severe problem). The sum of the answers to these 7 questions yields a total score ranging from 0 to 28.
Statistical analyses
Descriptive statistics were used to examine the tendency of the variables followed by mediation analyses. To test the mediational hypotheses, Baron and Kenny's21 3-step regression analysis was performed. The following criteria should be met: 1) The causal variable should have a substantial direct effect on outcome; 2) the causal variable should affect the mediating variable; and 3) the effect of the causal variable should disappear (complete mediation) or be substantially reduced (partial mediation) when controlling for the mediating variable. The causal variable's indirect effect through the mediating variable was estimated and tested for statistical significance. Since the sampling distribution shape is unknown in small samples, a bootstrapping procedure was also employed, using Hayes' PROCESS macro version 3.4.222324 All data analyses were performed using the Statistical Package for the Social Sciences, version 17 (SPSS Inc., Chicago, IL, USA) with significance established at P < 0.05.
RESULTS
Descriptive and correlation analyses
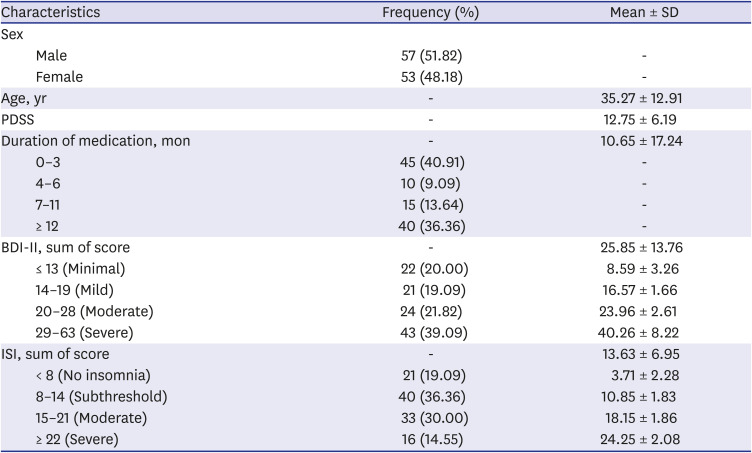
Table 1 summarizes the baseline characteristics per observed variable. The sample comprised approximately equal numbers of male and female participants (male:female = 57:53), with a mean age of 35 years (mean ± standard deviation = 35.27 ± 12.91). Almost 41% of the participants had duration of 0–3 months for drug treatment, and 10% had 4–6 months. Fourteen percent of patients continued medication for 7 to 11 months, while 36% continued treatment for more than a year. Eighty percent of participants demonstrated BDI-II scores ≥ 14, and almost 40% demonstrated BDI-II score ≥ 29 which implies severe depression. In terms of insomnia, more than 80% reported ISI scores ≥ 8 which suggests having insomnia symptoms; nearly 45% had clinical insomnia. The results of the correlational analysis are presented in Table 2. All correlations were reported when statistically significant.
Table 1
Sample characteristics of 110 participants with PD

Mediation analysis
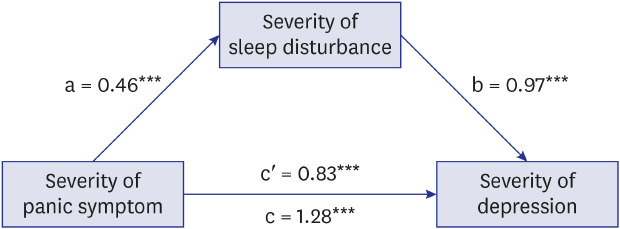
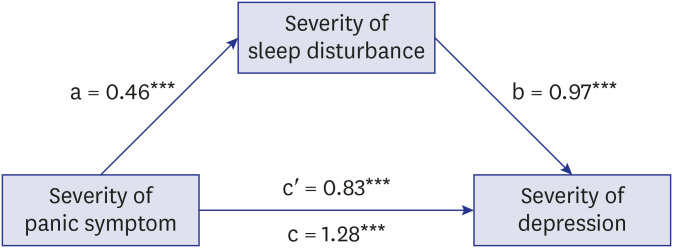
To quantify the mediating effect of insomnia on panic symptoms and depression, a mediation analysis using multiple regressions was performed (Table 3). The first regression analysis, with depression as the dependent variable and panic symptoms as the predictor, yielded a significant relation with participants perceiving more severe depression with more serious PD (β = 0.57, P < 0.001). A second regression analysis, with the mediator (insomnia) as the dependent variable and the panic symptoms as the predictor, demonstrated that severe panic symptoms increased sleep disturbance significantly (β = 0.41, P < 0.001). Another regression analysis was performed with both the panic symptom severity and sleep disturbance as predictors and depression as the criterion. This analysis revealed that the previously identified relationship between panic symptom severity (β = 0.37, P < 0.001) and insomnia retained its significance (β = 0.49, P < 0.001). Further support for this mediating effect of sleep disturbance was demonstrated using the Process Macro Model 4. In Fig. 1, the mediation model with insomnia (which mediates the relationship between severity of panic symptoms and depression) is presented. The total effect of panic symptom severity on depression was significant (t = 7.23, P < 0.001; c path). Also, there was a significant effect of panic symptoms on insomnia (t = 4.62, P < 0.001; a path) and of insomnia on depression (t = 6.69, P < 0.001; b path), based on unstandardized regression coefficients. Since the bootstrapped 95% confidence interval did not contain zero (0.23, 0.68), the indirect effect was significant. Furthermore, the main effect of panic symptom severity on depression was also significant, after controlling for the effect of insomnia, suggesting partial mediation (t = 5.11, P < 0.001; c′ path).
Table 3
Testing for insomnia as a mediator using multiple regression
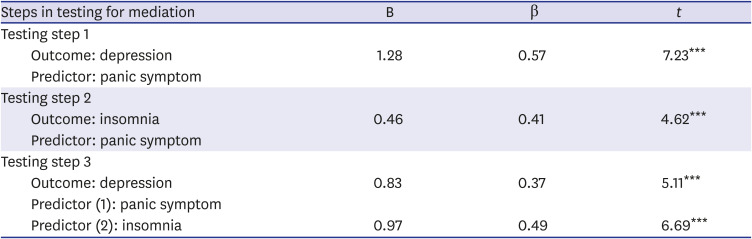
Fig. 1
A mediation model of insomnia in the relationship between panic symptom and depression. Regression coefficients are unstandardized; a, effect of panic symptoms on insomnia; b, effect of insomnia on depression; c, total effect of panic symptom severity on depression; c′, main effect of panic symptom severity on depression after controlling for the effect of insomnia.
***P < 0.001.
DISCUSSION
This study evaluated the mediating effect of insomnia (as assessed by the ISI) on the relationship between panic symptom and depression in patients with PD. Our main findings are as follows: 1) Depression symptoms are common in patients with PD; 2) Insomnia is common in patients with PD; 3) In patients with PD, depressive symptoms are partially mediated by insomnia. Several studies have shown that PD and depression occur together frequently, and that this may have important clinical implications (e.g., increased suicide risk, greater social dysfunction, poorer functional outcomes). Previous meta-analyses demonstrated that insomnia was significantly associated with depression,2526 however, to our knowledge, this is the first study considering insomnia as a mediating factor for developing depression in patients with PD.
In this study, depressive symptoms were frequently observed in patients with PD. A significant association between the severity of PD and depression was observed (β = 0.57, P < 0.001) (Table 3). In a mediation analysis, the total effect of panic symptom severity on depression was significant (t= 7.23, P < 0.001; c path). PD is found to be strongly associated with a wide range of other mental disorders, including depressive disorders (most common) and anxiety disorders (second most common). The findings presented here were consistent with those from previous studies. Comorbidity between PD and depression is one of the strongest psychiatric comorbidities in both treatment samples27 and general population studies,28 and many studies indicate that there is a higher incidence of depression in patients with PD.45629303132 The occurrence of secondary depression was related to the duration of illness, the number of panic attacks per year, and the degree of phobic avoidance in patients with PD.33 In addition, these two disorders have been known to share some risk factors. The tripartite model34 proposes that shared symptoms, such as negative affect or general distress factor represent their shared risk factors. Data from large-scale genetic studies have shown that factors affecting genetic variations between PD and major depressive disorders mostly reflect the same factors affecting those in neuroticism.3536 Also, both physical and/or sexual childhood abuse is known as a shared risk factor between PD and depression.37 The temporal priority of the timing of onset between two disorders has been a difficult topic to elucidate. In the NCS study,38 among the 302 respondents who reported at least one lifetime panic attack and one lifetime episode of depression, 31.1% indicated that their first episode of depression occurred before the first panic attack, 25.5% stated that both occurred in the same year, and 43.4% stated their first panic attack occurred prior to depression. These results are in line with previous studies demonstrating that anxiety precedes depression in individuals with lifetime comorbidity.39 A long-term follow-up study was conducted to investigate if sleep disturbances may affect treatment outcomes of patients with PD. According to the study, sleep disorders experienced throughout their lives appear to be a chain of mood spectrum disorders and PD.
As with depression, insomnia was also often seen in our sample. Approximately 81% of participants reported insomnia (ISI ≥ 8). In a regression analysis, severe panic symptoms were found to significantly increase sleep disturbances (β = 0.41, P < 0.001). Not only did insomnia correlate with symptoms of PD, but also showed a positive association with depression. As in many anxiety disorders, sleep may be affected in PD. In a recent study, there was a considerably higher prevalence of insomnia in patients with moderate to severe PD.10 Also, researchers have suggested that sleep disturbances and panic symptoms interact and reinforce each other in a vicious cycle.12 Studies of individuals from the general population revealed that one night of sleep deprivation increases general anxiety and physiological activation.40 When an individual experiences nightly panic attacks, they may have anxiety about sleeping.41 Anxiety can cause sleep deprivation, increase general activation and potentially trigger panic by delaying bedtime.12 Furthermore, some patients with PD tend to experience distress and even panic attacks with relaxed or reduced vigilance.42 There is a hypothesis that this reaction may occur shortly before bedtime in some patients and may interfere with the onset of sleep. In addition, there is evidence that certain cognitive (e.g., anxiety) and physiological (e.g., physiological arousal) signs of anxiety contribute to insomnia.43 For some individuals with anxiety disorders and insomnia, insomnia can be caused primarily by anxiety symptoms such as worry and physiological arousal.
Here, it has been shown for the first time that insomnia partially mediates the relationship between PD and depression in patients with PD. In fact, insomnia can play an important role in the development of depression. Several experimental studies have demonstrated that sleep disorders can lead to cognitive and emotional changes that pose a risk of depression.44 Alternatively, sleep disturbance may impair emotional control and stability,45 and may lead to changes in the neural processes connected to depression symptomatology.46 Secondly, continuous and chronic activation of the hypothalamic–pituitary–adrenal axis, the main neuroendocrine mediator of stress response, was proposed to play a key role in the development of depression in patients with insomnia with objective short sleep periods.4748
This study has several limitations. First, it is a cross-sectional study where data are collected at a single point in time to examine the relationship between disease and other variables of interest. Therefore, it is difficult to determine whether the outcome followed exposure in time or exposure resulted from the outcome. Secondly, this study leveraged data from a relatively small number of individuals. A small sample size affects the reliability of the results because of increased variability and bias. Thirdly, this study used self-report questionnaires. In collecting information through a self-report, people are often biased when reporting their experiences. For example, many individuals are either consciously or unconsciously affected by “social desirability.” That is, they are more likely to report experiences considered socially acceptable or preferred. Furthermore, since self-report questionnaires were used, patients were diagnosed without using structured interviews and comorbid disorders were only assessed at the symptom level. Finally, as insomnia is common with depression and also a possible symptom of depression. In this regard, it may not seem surprising that insomnia symptoms mediate depression. However, depression is known to be related various sleep disturbance from insomnia to hypersomnia, and the causal relationship between depression and insomnia has not been established yet. Therefore, our findings may help clarify such relationship.
It can be inferred that a specific insomnia treatment may be useful in preventing the occurrence of depression in patients with PD, a clinically significant outcome. The co-existence of PD with depression implies a serious and potentially ominous prophecy; the high suicide rate observed in patients with PD is further exacerbated by the coexistence of depression. Therefore, preventing depression in individuals with PD is very important because it may help reduce the risk of suicide as a result, a connection that has been made in many previous studies (i.e., the concurrence of depressive disorder and PD is related to the likelihood of suicide attempts).49505152
 XML Download
XML Download