

 PDF
PDF Citation
Citation Print
Print



In December 2020, the Republic of Korea (Korea) is experiencing a third wave of the coronavirus disease 2019 (COVID-19) pandemic.1 Although the cumulative proportion of COVID-19 among children and adolescents is lower in Korea (9.6% on December 20, 2020) than in the United States (12.2% on December 10, 2020), daily new cases among children are growing fast in both countries.12 Policies for COVID-19 in Korea require all cases to be admitted to isolation units of designated hospitals or residential treatment centers (RTCs), regardless of patient's age or symptoms. All children with COVID-19 are thus isolated in facilities, and cases arise where isolation with uninfected caregivers is required. However, mandatory admission to isolation units may not be necessary considering the mild degree of COVID-19 in children3 and the low transmissibility of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by children in households and schools.45 Limiting the spread of SARS-CoV-2 can also be achieved at home as recommended by many other countries.6 In this study, we evaluated the usefulness of facility isolation by estimating the time between symptom onset and entering isolation at a hospital or RTC as well as the clinical course during isolation. We also investigated the transmissibility of SARS-CoV-2 from infected children to uninfected caregivers in isolation units.
Children with COVID-19 were included from the Nowon RTC and Seoul Metropolitan Government-Seoul National University Boramae Medical Center (BMC) in Seoul from August 6 to November 14, 2020. All cases were confirmed by reverse transcription-polymerase chain reaction (RT-PCR) in a combined nasopharyngeal and oropharyngeal swab. Children were isolated with a caregiver in case of need. When the caregiver was uninfected with COVID-19, the infected child was encouraged to wear a facemask. The uninfected caregivers were recommended to use personal protective equipment (PPE) that includes an N95-equivalent mask (e.g., KF94), gowns, goggles, and gloves.7 Strict interventions on proper use of PPEs were not employed because most caregivers felt wearing PPEs is not feasible when caring for a child. There were no interventional incentives and disincentives directed to caregivers for adhering to the usage of PPEs. The patient's daily symptoms and vital signs were self-checked and/or monitored by the medical staff. Children's isolation was lifted on the 10th day after the diagnosis if asymptomatic, or on the 14th day from symptom onset if symptomatic.8 The uninfected caregivers' nasopharyngeal swabs were tested for SARS-CoV-2 before their child's end of isolation and two weeks after the isolation was lifted. Demographic, epidemiologic, and clinical data were collected retrospectively with an approval by the Institutional Review Board at Seoul National University Hospital and BMC and written consent was waived (IRB No. 2004-013-1115).
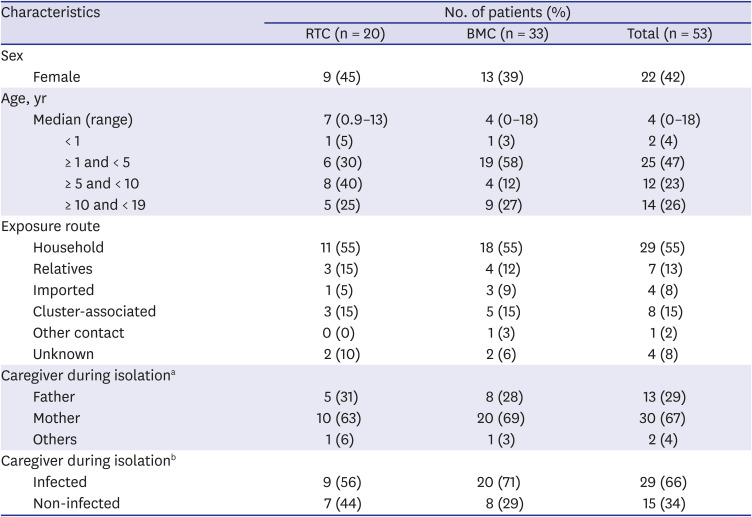
A total of 53 children were included in this study and their demographic and epidemiologic profiles are described in Table 1. The median age of the patients who stayed in BMC and RTC was 4 years (range, 0–18) and 7 years (range, 1–13), respectively. The most common source of infection was household contact (55%). Children were isolated for a median of 12 days (11 days and 12 days for asymptomatic and symptomatic patients, respectively). Fifty (94%) children were isolated with a caregiver; 38 children with a single caregiver, five pairs of siblings with one of their parents, one pair with both parents (infected father and uninfected mother).
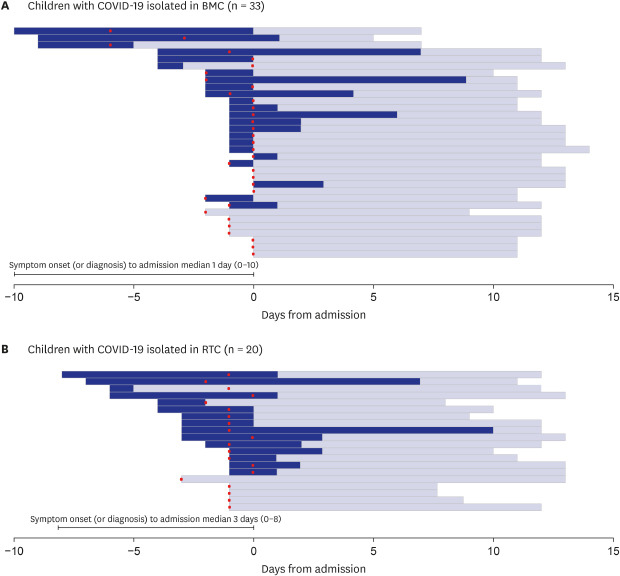
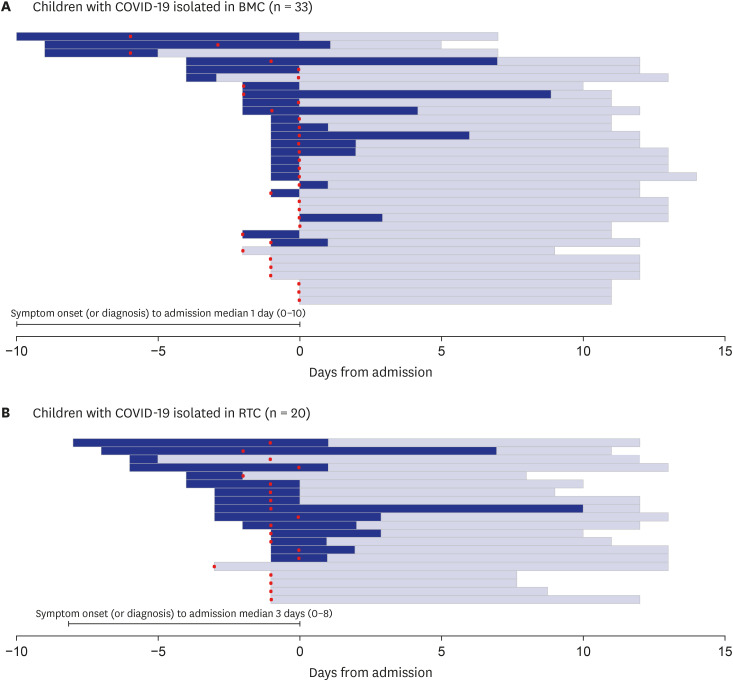
One fourth were asymptomatic until discharge and most symptomatic children presented with fever and/or upper respiratory symptoms. Detailed information about clinical manifestation was presented in Supplementary Table 1. All symptoms resolved without requiring specific treatment. The symptomatic children's total number of days with illness was calculated as 144 days. Of note, approximately 76% (109 days) were experienced before entering the isolation unit. Symptomatic children stayed in isolation symptomless for a median of 11 (0–18) days. The median time from symptom onset to facility isolation was 2 days (1 day at BMC and 3 days at RTC). Approximately 39% (n = 16) of the symptomatic children had spent some time with their family for longer than 2 days before entering the isolation unit (Fig. 1). In asymptomatic children, the median time from diagnosis to facility isolation was 1 day (1 day at both BMC and RTC) and 8% of the children stayed home with their family for longer than 2 days before entering the isolation unit (Fig. 1).
Meanwhile, 15 children in this study were isolated with a single uninfected caregiver. All of the 15 caregivers protected themselves by wearing facemasks and conducting hand hygiene, but did not wear gowns, gloves, or goggles. They had frequent close contact with their infected child while in isolation (Fig. 1). Furthermore, 10 (66.7%) of the children were younger than 5 years old who are unable to strictly follow the guidelines. In particular, three infants < 2 years of age were not required to wear a facemask. There was an uninfected mother who was co-located in the isolation room with two infected children (1 and 2 years old, respectively) and an infected husband (index patient of this cluster). The mother had become infected by the end of self-quarantine at home. She often could not comply with the recommendations of personal protection when she was surrounded by the three family members with COVID-19. Nevertheless, none of the uninfected caregivers became infected during the study.
Reports on pediatric cases of COVID-19 suggest that children generally have mild illnesses.23 In the US, less than 5% of all children diagnosed with COVID-19 are hospitalized,2 whereas all children with COVID-19 in Korea have been placed in isolation units at medical facilities as of December 2020.1 In the early case series of 91 children with COVID-19 in Korea, 88% were asymptomatic or had unrecognized symptoms for a median 3 (range, 1–28) days prior to diagnosis,9 which implies that many children with COVID-19 already stayed in the community during the period of high infectivity. Moreover, there was no need for mechanical ventilation and/or intensive care management, suggesting that most of the children would have recovered without hospitalization. Similarly, 53 children with COVID-19 in this study were either asymptomatic or mildly symptomatic. During the median observation period of 12 days, all children were released from isolation with no significant medical issues and requirement of medical treatment. Most of the children in isolation rooms were actively running around, studying, or simply watching video clips on smartphones. Occupation of hospital beds or rooms at RTC by these children with mild clinical course should be reconsidered especially when the magnitude of the pandemic is becoming a burden on the local healthcare system.
The imposition of strict isolation of all confirmed COVID-19 cases in facilities in Korea might have been a successful strategy in limiting virus spread and meeting timely management of patients at risk during the earlier stage of the pandemic. However, with a rapid surge of COVID-19 cases in Korea, enormous amounts of medical and human resources are unnecessarily used to isolate and care for infected children whose illness generally improve spontaneously. These resources could be more efficiently utilized for severely ill patients with genuine medical needs. The RTCs are designed to accommodate asymptomatic and mild COVID-19 cases with an expectation of limiting spread in the community as well as sparing beds in hospitals. However, constructing RTCs still cannot keep up with the rapid increase of COVID-19 cases. Moreover, as shown in our study, most patients with COVID-19 stay in the community during the early phase of the infection when the infectivity is highest, and enter RTCs at the time when the viral load of SARS-CoV-2 is expected to decrease.10 Thus, the benefit of isolating children in medical facilities for limiting transmission might not be as great as expected. In addition, the current study shows that children already have been cared safely at home during the acute phase of COVID-19.
The impact of isolating children in facilities on their physical and mental health should not be overlooked.11 Children isolated with only one caregiver or even alone in the unit are likely to be more restricted physically and stressed mentally than those accompanied by other family members at home. This is not only a problem in COVID-19 confirmed children but also non-infected children who remain at home without main caregivers. In one case of this study, a 4-year-old boy's anxiety worsened significantly when he remained at home without his main caregiver who had to care for an infected sibling in a RTC. For this case, staying home and following isolation guidelines would have been better for the entire family.
Meanwhile, the transmissibility of COVID-19 by children, although yet to be defined, has been reported to be low compared with other age groups. An early study on household transmission from children showed a secondary attack rate of 0.5%.5 Also, in a previous study with a similar setting to the current study, 12 uninfected caregivers isolated in hospitals with their child who had COVID-19 were not infected with the use of appropriate PPEs.12 In this study, even only with the use of facemask, none of the 15 caregivers were secondarily infected by their child in a situation of inevitable close contact for a prolonged period. These observations suggest that household transmission of COVID-19 by children to their guardians might be negligible with appropriate precautions including facemasks and hand hygiene.
In conclusion, in this descriptive observational study we found that most of the children with mild COVID-19 were already symptomatic for some time before entering isolation units. Moreover, their clinical course was uneventful during the isolation period and the risk of virus transmission to their uninfected caregivers was low. Amid the third wave of the pandemic in December 2020 when we are experiencing a shortage of hospital beds, the Korea Disease Control and Prevention Agency with the support of the Korean Society of Pediatric Infectious Diseases released the new guidelines for home care for children with COVID-19.13 In accordance with the guidelines, children with mild COVID-19 may be cared for safely in home settings. Children may benefit psychologically by staying at home, without increased risks for clinical deterioration or transmission of the virus to family members.
 XML Download
XML Download