

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The survival of adults with congenital heart disease (ACHD) is increasing by virtue of improvement in medical and surgical treatment.12 Health conditions related to congenital heart disease (CHD), such as congenital heart anomalies, past surgeries and procedures, residual cardiovascular abnormalities, and acquired hypertension or coronary artery disease make for a complex and continuous impact on the cardiovascular system in ACHD. For these reasons, long-term and systematic treatment management is required for ACHD.
A variety of issues require additional monitoring in ACHD compared to the general population, including ventricular function problems, arrhythmia, cyanosis, quality of life and psychological issues, infection, surgery, and pregnancy. Among these, arrhythmia, especially atrial fibrillation (AF), has become a serious public health concern and economic burden34 with the emergence of an aging society.5 The association between atrial septal defect (ASD), one form of CHD, and AF is well established. The main cause of morbidity in adults with ASDs is atrial arrhythmias. Approximately 10% of untreated patients with ASDs develop atrial arrhythmias, predominantly AF, by 40 years of age.67 The incidence continues to rise with age and AF is reported in more than 50% of patients after the age of 60.78 Therefore, the number of ACHD with AF is expected to increase.79 However, there are few studies regarding the incidence of AF in ACHD patients and its impact on survival. Therefore, our aim in this study was to assess the impact of AF on the survival of ACHD patients using Korean National Health Insurance Service (KNHIS) data.
METHODS
Study population
We collected the data from the KNHIS records from 2006 through 2015.10 The ACHD data in the National Health Insurance benefit records represent newly diagnosed patients in the corresponding year. AF patients in ACHD were identified, and the death data for Koreans from 2006 through 2016 were used for survival analysis.
KNHIS database
The universal coverage health insurance system in Korea for all citizens was initiated in 1963, based on the National Medical Insurance Act. And universal healthcare coverage was achieved in 1989.1112 The KNHIS database for Health insurance subscribers and Medicare recipients excluding foreigners consists of the following four databases: 1) qualification database including age, sex, type of subscription (e.g., insured employees, insured self-employed individuals or medical aid beneficiaries), income rank, and death; 2) medical check-up database includes the general health examination data for the insured employees by every year or every two years. In addition, it contains the data for the insured self-employed and insured employees who get their lifetime transition period medical check-ups at 40 years old and 66 years old; 3) medical institution database including clinic type, number of beds, number of medical doctors, and location of medical care institution; 4) treatment database including the type of disease, disease code using the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), and prescription. Treatment database has four categories of medicine, dentist, oriental medicine, and pharmacy. Among those four categories of treatment database, we only used the medicine. And we used variables from the qualifications database in conjunction with the treatment database.1314
Definition of variables
Age was categorized as 20–29 years, 30–39 years, 40–49 years, 50–59 years, 60–69 years, 70–79 years, and 80 years or older. A socioeconomic factor included the percentile group of income level using the national health insurance premium divided into 20 quartiles. Income level was categorized as below 25%, 25%–49%, 50%–74%, and 75% or over.
Diagnosis
The data consisted of the diagnoses of CHD according to the ICD-10.15 The diagnoses used were Q20, congenital malformations of cardiac chambers and connections; Q21, congenital malformations of cardiac septa; Q22, congenital malformations of pulmonary and tricuspid valves; Q23, congenital malformations of aortic and mitral valves; Q24, other congenital malformations of heart; Q25, congenital malformations of great arteries; and Q26, congenital malformations of great veins; and I27.8, Eisenmenger syndrome. The followings are the specific diagnoses of ACHD. 1) Congenital ventricular and/or ASDs, including atrioventricular septal defects (Q21.2), ventricular septal defects (VSD; Q21.0, Q21.00, Q21.01, Q21.08, Q21.09), ASDs (Q21.1, Q21.10, Q21.11, 21.18, Q21.19), and congenital malformation of the cardiac septum, unspecified (Q21.9); 2) patent ductus arteriosus (Q25.0); 3) pulmonary artery stenosis (Q22.1, Q25.6); 4) coarctation of aorta (Q25.1); 5) pulmonary venous connection (Q26.2, Q26.3, Q26.4); 6) congenital tricuspid valve disease (Q22.4, Q22.8, Q22.9); 7) congenital aortic valve disease (Q23.0, Q23.1); 8) congenital mitral valve disease (Q23.2, Q23.3); 9) malformation of coronary vessels (Q24.5, Q24.8, Q24.9); 10) stenosis or malformation of aorta (Q24.4, Q25.2, Q25.3, Q25.4, Q25.8, Q25.9); 11) Tetralogy of Fallot (Q21.3); 12) Ebstein anomaly (Q22.5); 13) transposition of great arteries (Q20.3); 14) corrected transposition of great arteries (Q20.5) 15) Eisenmenger syndrome (Q21.81, I21.81); 16) double outlet right ventricle (Q20.1); and 17) single ventricle (Q20.4). AF was diagnosed with ICD-10 code I48.
Because ICD-10 code Q21.0 (VSD or ASD) was subdivided in 2011, we ran additional analyses for the difference by AF, survival curve, and death risk of VSD (Q21.00, Q21.01, Q21.08, Q21.09) and ASD (Q21.11, Q21.10, Q21.18, Q21.19, Q21.2) from 2011 through 2015.
Comorbidities
We collected comorbidities from primary and secondary diagnoses; hypertension (I10, I11, I12, I13, I15); diabetes mellitus (DM; E10, E11 E12, E13, E14); myocardial infarction (I21, I22, I25.2); heart failure (I11.1, I50, I97.1); ischemic stroke (I63); hemorrhagic stroke (I60, I61, I62); and malignant neoplasm (C00–C97).
Statistical methods
The differences in characteristics were analyzed using the Student's t-test for the continuous variables and the χ2 test for the categorical variables. The χ2 test was used to compare the distribution between AF in ACHD and AF in the Korean general population (n = 679,416).10 The Cochran-Mantel-Haenszel test was used to compare the distribution among ACHD, AF in ACHD, and/or AF in the Korean general population. KNHIS records in 2015 included 41,701,269 individuals.10 We calculated the age-standardized incidence rates (incidence rate) of ACHD, AF in ACHD, and AF in the Korean general population with the direct method16 using the beneficiaries of health insurance from the Korean National Health Insurance Statistical Yearbook from 2006 through 2015 and the estimated Korean population in 2015 as the reference.17 In addition, the incidence rate of AF in ACHD with the direct method was calculated using age groups according to the direct method using a decade of ACHD data as a reference. The Kaplan-Meier method was used to compare survival among patients with ACHD according to AF, AF by age group, and AF by sex using the log-rank or Wilcoxon tests. Simple and multiple Cox proportional hazards analyses were carried out using the variables of age, sex, income level, AF, and comorbidities such as hypertension, DM, myocardial infarction, heart failure, ischemic stroke, hemorrhagic stroke, and malignant neoplasms. If not specified, the hazard ratio (HR) of death from AF in ACHD patients will be referred to as ‘HR for AF in ACHD.’
RESULTS
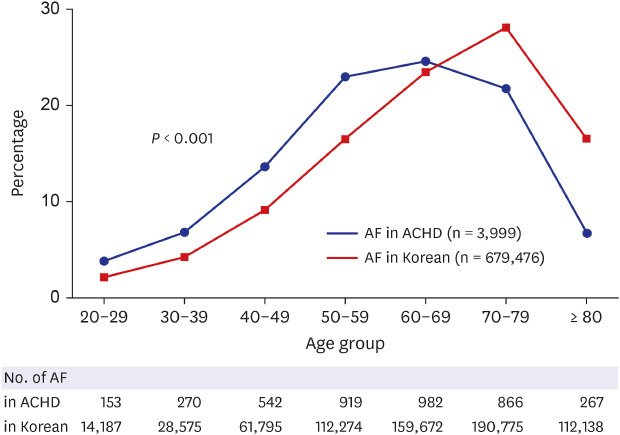
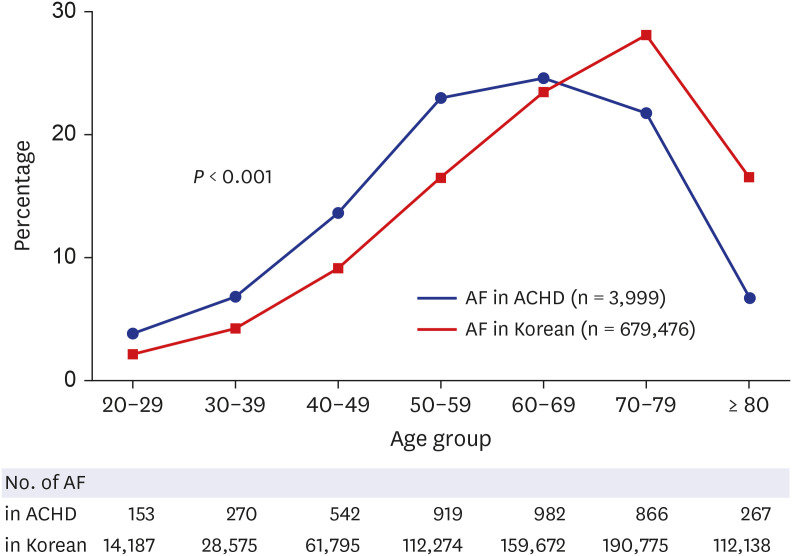
The distribution of the patients with diagnosed ACHD (n = 66,690) by AF in ACHD (n = 3,999) in Korea from 2006 through 2015 are presented in Table 1. The clinical characteristics of AF patients included older age, a higher proportion of male sex, and more comorbidities, e.g., hypertension, DM, heart failure, and ischemic stroke, compared to non-AF patients (P < 0.01). In AF patients, there was a higher proportion of ASD, congenital tricuspid valve disease, congenital aortic valve disease, congenital mitral valve disease, Ebstein anomaly, and corrected transposition of great arteries than in non-AF patients (P < 0.05). We showed the distribution of general characteristics with ACHD and AF in ACHD between 2006 and 2015 by year in Supplementary Table 1. The mean age of the ACHD patients increased from 45.1 (± 17.1) years in 2006 to 52.3 (± 16.1) years in 2015 (P < 0.001). The proportion of ACHD patients at age ≥ 70 years increased from 9.7% in 2006 to 15.9% in 2015 (P < 0.001). The male proportion increased from 40.0% in 2006 to 47.1% in 2015 (P < 0.001). The mean age of ACHD patients with AF increased from 54.0 (± 15.8) years in 2006 to 63.1 (± 13.3) years in 2015 (P < 0.001). The proportion of ACHD patients with AF at the age of ≥ 70 years increased from 18.2% in 2006 to 36.0% in 2015 (P < 0.001). The proportion of age groups with AF in between ACHD patients (n = 3,999) and the general population with non-valvular heart disease (n = 679,476) in Korea10 was different (P < 0.001) (Fig. 1). We showed the distribution of characteristic by AF in specific ACHD in Supplementary Table 2 and the distribution of AF and comorbidities by sex in ACHD in Supplementary Table 3. And the crude HR of death for AF in ACHD subjects was 2.61 (95% confidence interval [CI], 2.43–2.81). After adjustments for age, sex, comorbidities, and income level, adjusted HR for AF in ACHD was 1.39 (95% CI, 1.29–1.50). The HR for age, sex, and specific CHD are described in Supplementary Table 4.
Table 1
Distribution and death risk of characteristics by AF in ACHD from 2006 through 2015 (n = 66,690)
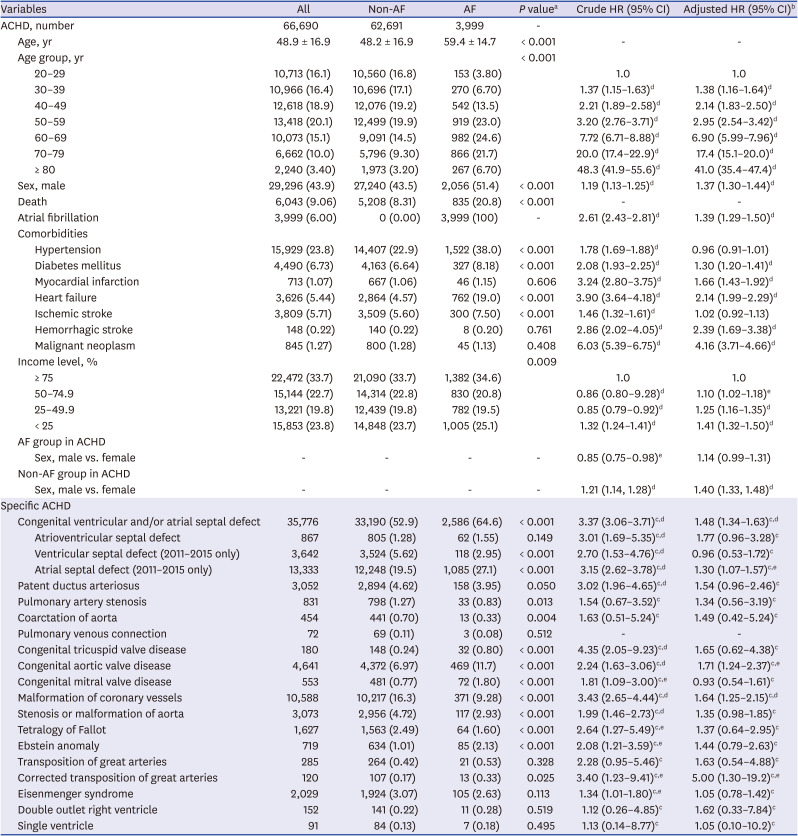
Values are presented as mean ± standard deviation or number (%).
AF = atrial fibrillation, ACHD = adults with congenital heart disease, HR = hazard ratio, CI = confidence interval.
aStudent's t-test or χ2 test; bHR after adjustment for age, sex, atrial fibrillation, comorbidities, and income levels; cHR for AF vs. non-AF in each specific ACHD; dP < 0.001; eP < 0.05.
Fig. 1
Distribution between newly diagnosed AF patients in ACHD (n = 3,999) and non-valvular AF in the Korean general population10 (n = 679,476).
AF = atrial fibrillation, ACHD = adults with congenital heart disease.
As shown in Table 2, the incidence rate of AF in the Korean general population from 2006 through 2015 was 1,842.0 persons per 100,000. The incidence rate of AF in ACHD was 5,996.4 persons per 100,000 ACHD. It was higher than that in the Korean general population (P < 0.001). The incidence rate of ACHD, AF in ACHD, and AF in the Korean general population increased with aging (P < 0.001). We showed the incidence rate of AF with ACHD from 2006 through 2015 by sex and by year in Supplementary Table 5. And we also showed the incidence rate of ACHD and specific ACHD from 2007 through 2015 by year to assess newly diagnosed ACHD and specific ACHD in Supplementary Table 6.
Table 2
Age-standardized incidencea,b and 95% CI of AF in ACHD, ACHD, and AF in the Korean general population10 over a decade (from 2006 through 2015) (unit: per 100,000)
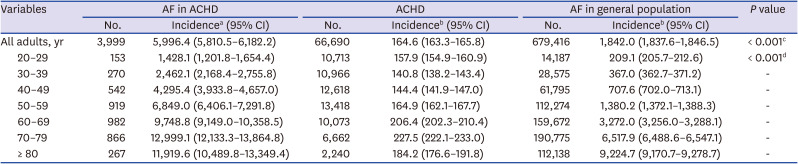
CI = confidence interval, AF = atrial fibrillation, ACHD = adults with congenital heart disease, ICD-10 = the 10th revision of the International Statistical Classification of Diseases and Related Health Problems.
aAge-standardized incidence rates of AF (ICD-10 codes: I48) with ACHD (ICD-10 codes: Q20.x, Q21.x, Q22.x, Q23.x, Q24.x, Q25.x, Q26.x, and I27.8) were calculated using age groups according to the direct method using a decade of ACHD data as a reference; bAge-standardized incidence rates of AF (ICD-10 codes:I48) with ACHD (ICD-10 codes: Q20.x, Q21.x, Q22.x, Q23.x, Q24.x, Q25.x, Q26.x, and I27.8), ACHD, and AF in the Korean general population were calculated using age groups according to the direct method using the estimated Korean population in 2015 as a reference; cComparing between AF in ACHD and AF in the Korean general population using the Cochran-Mantel-Haenszel test; dComparing among AF in ACHD, ACHD, and AF in the Korean general population using the Cochran-Mantel-Haenszel test.
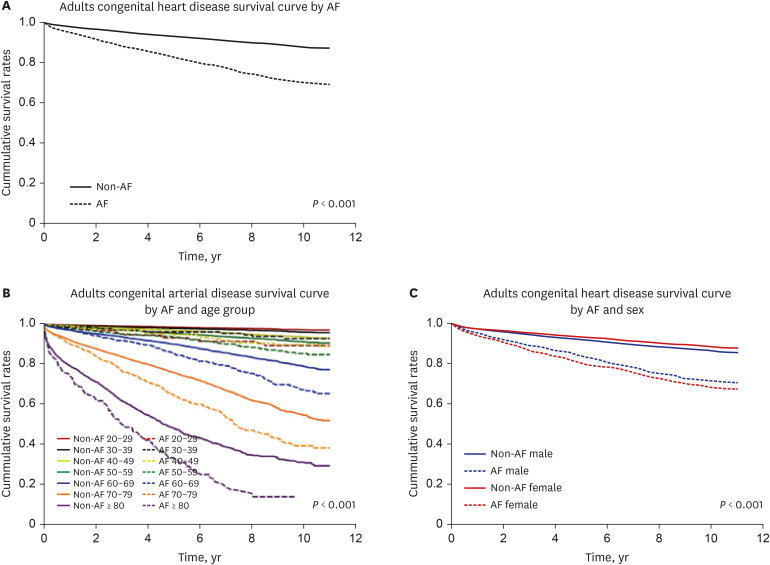
The overall 10-year survival rate (SR) for ACHD was 86.0% (Supplementary Fig. 1).15 The overall 10-year SR for ACHD was higher in non-AF patients (87.5%) than in AF patients (69.7%) (P < 0.001) (Fig. 2A). The 10-year SR for AF in ACHD decreased with aging (P < 0.001) (Fig. 2B). In terms of sex difference, the overall 10-year SR for ACHD was higher in females (86.9%) than in males (85.0%) (P < 0.001) (Supplementary Fig. 1). The 10-year SR for non-AF in ACHD was 88.2% in females and 86.4% in males and the 10-year SR for AF in ACHD was 68.1% in females and 71.2% in males (P < 0.001) (Fig. 2C). The 10-year SR for ACHD is shown in Supplementary Fig. 1 and the 10-year SR for all the specific CHD depending on the presence of AF is shown in Supplementary Fig. 2.
DISCUSSION
Although myocardial infarction, heart failure, hemorrhagic stroke, and malignant neoplasm have high HR in ACHD, AF also has high HR in ACHD. Therefore, we discuss HR for AF in ACHD. The HR for AF in ACHD after adjustment for age, sex, income level, and comorbidities was 1.39 in this study. Similarly, high HR for atrial arrhythmia in CHD death occurred in a population-based analysis from Quebec, Canada (HR, 1.47)18 and in the CONCOR study in the Netherlands (HR, 2.11 after adjusting for age, sex, repair status, and defect severity).19 On the other hand, the adjusted HR for AF was from 0.70 to 0.98 in the Korean non-valvular general population.10 The proportion of death in the AF group with ACHD was 2.5 folds higher than that in the non-AF group with ACHD, and the incidence rate of AF in ACHD (5,996.4 persons per 100,000) was higher than that in the general Korean population (1,842.0 persons per 100,000) over a decade. Therefore, AF may occur more frequently in ACHD and have a worse prognostic effect than in the general population with non-valvular AF.
The prevalence and mortality were increased with aging in a Korean CHD study.15 AF was more common in aging patients with CHD2021 and the incidence rate of AF in ACHD was higher for older age groups in Taiwan.22 In our study, the mean age of the AF group was higher than that of the non-AF, and the proportion of AF became greater with aging in ACHD (Table 2). The common age group of AF with ACHD was 50's to 70's (Supplementary Fig. 3). The overall 10-year SR for ACHD was 86.0% (Supplementary Fig. 1).15 The SR for AF was lower than that for non-AF subjects in the older age group with ACHD (Fig. 2B). The duration of atrial volume overload has been identified as a key factor promoting atrial fibrosis linked to atrial arrhythmias in patients with CHD.23 Atrial fibrosis increases with age and contributes to the structural remodeling that plays a key role in promoting and maintaining AF. In addition, as patients with CHD age, they risk acquiring comorbidities such as hypertension, diabetes, and obesity that further contribute to atrial dilation, fibrosis, and electrical remodeling, increasing vulnerability to AF.724 Consequently, the SR for AF with ACHD decreased due to incremental factors related to aging. In addition, research on other diseases based on KNHIS data, such as Takayasu's arteritis14 or thromboangiitis obliterans,25 showed a lower SR or higher HR with age, in agreement with ACHD showing a lower SR or higher HR with age in the present study. For these reasons, we could not exclude the natural history of aging in ACHD. Therefore, AF in ACHD could have important clinical and public health implications with aging. Furthermore, Korea is a country that is aging at the greatest rate in the world. The proportion of the population over the age of 65 years increased from approximately 7% in 2001 to greater than 14% in 2017, indicating that Korea is an aged society.
For males, the HR for ACHD was significantly higher than that for females. Interestingly, the 10-year SR was lower in females than in males in AF with ACHD. Because Korean males had a higher mortality rate and lower life expectancy than in Korean females,2627 we could not explain precisely the reason why 10-year SR in females with AF in ACHD was lower than that in males. However, we could speculate that male patients might be more likely to die before AF develops because overall survival in ACHD was lower and the prevalence of serious comorbidities was higher in male patients (Supplementary Table 3). The adjusted HR for males in ACHD with AF did not increase significantly (HR, 1.14; 95% CI, 0.99–1.31 in Table 1).
Malignant neoplasm showed the highest HR for ACHD among comorbidities, which was consistent with the report that the first cause of death in Korea is malignant neoplasm.26 Heart failure also had a higher HR in ACHD. One of the common causes of heart failure is CHD, and various congenital heart malformations cause heart failure due to pressure and/or volume overload. In Swedish Cause of Death register data from 1970 to 1993, CHD patients with AF developed heart failure.28 Myocardial infarction, hemorrhagic stroke, and DM had higher HRs for ACHD. The odds ratio for coronary artery disease in ACHD was associated with atherosclerotic risk factors in Canada,2930 and the relative risk for hemorrhagic stroke with CHD was 8 folds higher than that of matched controls from the general population in Sweden.31 There was a significantly higher death risk for ACHD depending on a relatively lower income level. Income inequality can actually affect cardiovascular disease.32
The overall proportion of AF with ACHD was 6.0% over a decade. This result is similar to a study that found 8.3% AF among 21,982 Swedish patients with CHD from 1970 to 1993.28 For specific CHD, the proportion of congenital ventricular and/or atrial septal defect, ASD, congenital aortic valve disease, malformation of coronary vessels, and Eisenmenger syndrome was 53.6%, 20.0%, 7.3%, 15.9%, and 3.0%, respectively (Supplementary Fig. 4). The proportion of AF in ASD was 27.1%, which is the highest value among specific ACHDs in this study. This finding is consistent with a previous study by Moe et al.21 who found 23% AF or atrial flutter in ASD patients. We also found higher HRs of AF for ASD, patent ductus arteriosus, congenital aortic valve disease, malformation of coronary vessels, and Eisenmenger syndrome. This result was similar to a previous study. ASD can develop dilatation of right atrium which may become substrates for AF development. Interestingly, HRs for AF in congenital tricuspid valve disease, congenital mitral valve disease, stenosis or malformation of aorta, Tetralogy of Fallot, Ebstein anomaly, and corrected transposition of great arteries in simple Cox proportional hazards analysis were significant. Meanwhile, adjusted HRs for AF did not show any significance in our study. Because CHD shows various types of cardiac structural abnormality, it has very different hemodynamic changes for each patient and cardiac anomaly type arrhythmias.333435
Our study has several limitations.15 First, the national health insurance benefit records might have missed ACHD of patients who did not use medical services or who paid for their own medical expenses.36 The section is relatively low in Korea because the national health insurance system covers almost all the Korean population. Second, we could not evaluate clinical data such as the size of atrial shunt (or defect), timing of the ASD repair, or the type of ASD, medication data such as anticoagulant drugs, the occurrence of AF related to cardiac surgery, or procedures because of data limitations. Third, we could not determine the cause of death because the Korean National Health Insurance benefit data do not include this information. Therefore, a long-term hospital-based AF and ACHD registry including echocardiography data in Korean patients would be useful for identifying anatomical and hemodynamic correlations from echocardiography data. Such long-term, large-scale analysis would contribute to preventive measures to reduce the incidence of AF in ACHD and associated mortality.
In conclusion, AF may occur earlier in ACHD patients and have a worse effect on ACHD than in the general population with non-valvular AF in Korea. AF may portend a worse prognosis in ACHD patients with a 10-year SR of about 70% across a decade. Specifically, the older age group and female group had lower SRs than their counterparts. Therefore, AF should be considered in future research designs and cardiovascular healthcare services policies for ACHD, with particular attention given to sex and age.
 XML Download
XML Download