

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Staphylococcal scalded skin syndrome (SSSS) is a skin disease characterized by blistering and desquamation caused by exfoliative toxins (ETs) of Staphylococcus aureus.
1 It mainly affects neonates and children younger than five years of age. SSSS shows clinical improvement with appropriate antimicrobial treatment and fluid management.2 However, cases of sepsis, renal failure, and electrolyte imbalance may lead to significant morbidity and mortality.
The recommended empirical therapies for SSSS include penicillinase-resistant penicillins, first-generation cephalosporins, and clindamycin.3 Previous epidemiologic studies showed predominant isolates in SSSS among children to be methicillin-susceptible S. aureus (MSSA).456 However, recent reports have shown cases due to methicillin-resistant S. aureus (MRSA).78 Thus, some experts recommend the use of vancomycin for empirical treatment of SSSS in countries in which MRSA is prevalent.1 Although the role for systemic antibiotics is not fully defined, decisions on empirical antibiotic treatment should be based on the local epidemiology of antimicrobial susceptibility of S. aureus responsible for SSSS.
Although epidemiologic studies for SSSS are limited in Korea, MRSA has recently been reported to be predominant in children with SSSS.910 The aim of this study was to investigate the microbiological characteristics of S. aureus isolated from children diagnosed with SSSS. Furthermore, we studied the clinical characteristics of SSSS patients according to S. aureus clones and ETs.
METHODS
Study design
This study was conducted in three different university hospitals located in two cities (Seoul, Seongnam) and one island (Jeju) in Korea. We included subjects under 15 years of age from January 2010 to December 2017 who were clinically diagnosed with SSSS and those in which S. aureus was isolated. In all three hospitals, S. aureus isolates from clinical specimens were stored at -70 °C through a hospital-wide surveillance system. The isolation sites of S. aureus included the nasal mucosa, axilla, and inguinal area.
Demographic information and clinical findings of patients such as age, sex, fever, underlying diseases, laboratory results, treatments, and outcomes were investigated based on medical records. The clinical characteristics of SSSS, including the involved area of the skin, the presence of Nikolsky's sign, and the status of desquamation were collected. SSSS cases were classified into three types.11 The generalized type was defined as a large area of skin lesions (over 30% of the whole body) with tender erythroderma, large bullae, and a positive Nikolsky's sign. The intermediate type was defined as skin lesions with tender erythroderma, vesicles, or pustules in a regionally limited area (< 30%) and a positive Nikolsky's sign. The abortive type was defined as a case of a diffuse scarlatiniform rash with tender erythema without Nikolsky's sign.
Analysis of S. aureus isolates
Microbial identification and antimicrobial susceptibility tests were performed using automated microbiology systems, including Vitek II ID-GPC (bioMérieux, Durhan, NC, USA) and Microscan Walk-Away (Siemens Healthcare Diagnosis, Deerfield, USA). Genomic DNA from S. aureus isolates was extracted using a Wizard® Genomic DNA Purification kit (Promega, Madison, WI, USA). Sequencing reactions were performed in the DNA Engine Tetrad 2 Peltier Thermal Cycler (Bio-Rad, Hercules, CA, USA) using the ABI BigDye® Terminator v3.1 Cycle Sequencing kit (Applied Biosystems, Waltham, MA, USA) in Macrogen Corporation (Seoul, Korea). Seven housekeeping genes (arc, aroE, glpF, gmk, pta, tpi, and yqi) of S. aureus were amplified by PCR, and the amplification products were sequenced using the MLST database (https://pubmlst.org/saureus/). All S. aureus isolates were tested for the presence of ET genes (eta, etb) by PCR using primers that were described previously.12
Statistical analysis
An independent two-sample t-test was used to analyze parametric continuous variables, while differences between categorical variables were tested using the χ2 test. All data were analyzed using R software version 3.4.3 (R Foundation for Statistical Computing, Vienna, Austria), and the results were considered statistically significant when the P value was less than 0.05.
RESULTS
Demographic and clinical characteristics of children with SSSS
A total of 26 children were included in this study from January 2010 to December 2017 at Seoul National University Hospital Children's Hospital (n = 2), Seoul National University Bundang Hospital (n = 12), and Jeju National University Hospital (n = 12). All episodes occurred before the hospital visit, and had no epidemiologic relationship with each other. The mean age was 2.3 years (range, 0–4.8 years). Nine children (34.6%) were under one year of age, and two (7.7%) were under one month. The sex ratio of cases was 1:1. Five children (19.2%) had underlying diseases, including two preterm infants, one with atopic dermatitis, one with paroxysmal supraventricular tachycardia, and one with vesicourethral reflux.
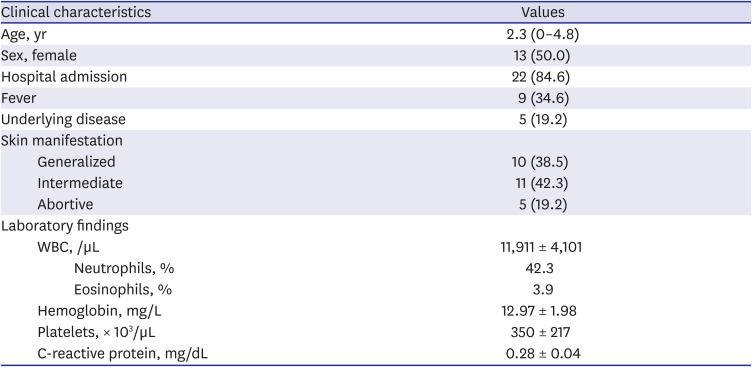
Among all patients, 22 (84.6%) were hospitalized and four (15.4%) were diagnosed and treated at outpatient clinics. Fever (defined as body temperature above 38°C) was detected in nine (34.6%) patients. According to skin manifestations, the intermediate type was found in 42.3% (n = 11), followed by generalized type (38.5%, n = 10) and abortive type (19.2%, n = 5). Laboratory findings of all SSSS patients are shown in Table 1.
Table 1
Clinical characteristics of children with staphylococcal scalded skin syndrome
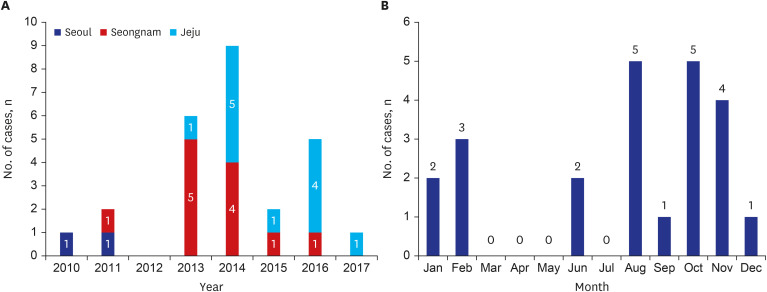
Yearly and monthly distribution of SSSS patients are shown in Fig. 1. More than half of the SSSS patients (n = 15, 57.7%) were diagnosed during 2013 and 2014. According to monthly distribution, the highest number of patients (n = 5, 19.2%) were identified in August and October, respectively.
Antimicrobial susceptibility and treatment
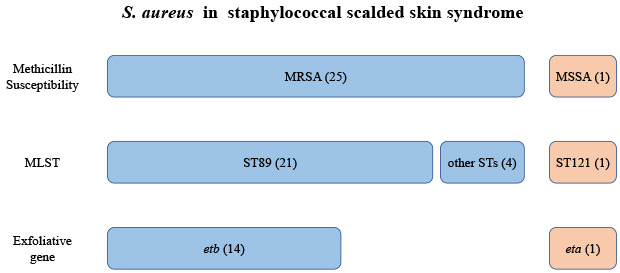
The majority of S. aureus isolates (25/26, 96.2%) was resistant to methicillin. Erythromycin resistance was found in 24 (92.3%) and clindamycin resistance in 22 (84.6%) of the isolates. Among the 22 clindamycin-resistant isolates, all isolates were resistant to erythromycin. All isolates were susceptible to vancomycin, rifampin, ciprofloxacin, and trimethoprim/sulfamethoxazole.
In this study, all patients were treated with systemic antibiotics. The mean duration of antimicrobial treatment was 8.3 days regardless of the administration route. Nafcillin or first-generation cephalosporin was most commonly prescribed (n = 20, 76.9%) for the treatment of SSSS. Vancomycin was administered to four patients (15.4%) and clindamycin to nine patients (34.6%) (Table 2). Among children with SSSS in which MRSA was isolated, five children (20.0%) were treated with susceptible antibiotics (vancomycin or clindamycin), and the mean duration of the susceptible antimicrobial treatment was 9.75 days. Interestingly, among children treated with non-susceptible agents, the mean antimicrobial treatment duration was 8.07 days. However, the difference was not statistically significant (P > 0.05). No cases had secondary skin infections, but acute renal failure occurred in a preterm infant six days after exfoliation of the skin and peritoneal dialysis was performed for one week. After treatment, the patient recovered without permanent renal sequelae. This was the only case in which MSSA was isolated.

Multilocus sequence test and ET
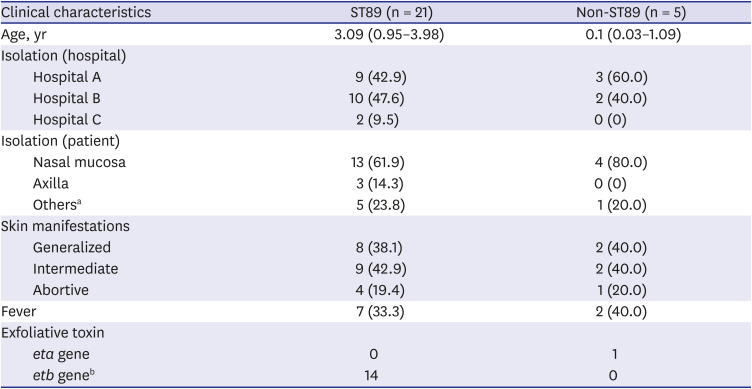
Among the 26 S. aureus isolates, six different sequence types (STs) were found. The most common clone was ST89 (n = 21, 80.8%) with single clones of ST1, ST5, ST72, ST121, and ST1507. All ST89 isolates were resistant to methicillin and erythromycin. Among the ST89 clones, 14 (66.7%) had the etb gene. The eta gene was detected in one isolate (3.8%), which was the only methicillin-susceptible isolate and was ST121. The etb gene was detected in 14 isolates (53.8%), which were all ST89. The detection rate of ET gene according to clinical status were as follows; 60.0% (3/5) in abortive type, 60.0% (6/10) in generalized type, and 63.6% (7/11) in intermediate type. We observed no differences in the clinical characteristics depending on STs. However, etb gene detection was significantly related to ST89 (P < 0.05) (Table 3). The presence of the etb gene was not related to skin manifestations or fever.
Table 3
Comparison of clinical characteristics and exfoliative toxins according to sequence type
DISCUSSION
This study aimed to investigate the clinical features of SSSS in children and the molecular characteristics of S. aureus in SSSS in children in Korea. Among the 26 cases in this study which were recorded over the course of eight years, the majority of the isolates were found to be methicillin-resistant. The most prevalent ST was ST89. In addition, the etb gene was detected in 14 isolates (53.8%), all of which were ST89.
In this study, MRSA was isolated in 96.2% of patients with SSSS. This differs greatly from reports in other countries. Most epidemiological studies on SSSS showed that MSSA isolates accounted for 98.3%–100% in the USA, France, and Ireland.51314 Reports in China and Japan, which are countries adjacent to Korea, also reported the majority of their isolates to be MSSA at 95%–100%.61516 Meanwhile, an outbreak of SSSS was reported in Taiwan, with 70% (7/10) of cases due to MRSA.17 In general, methicillin resistance has not been found to be largely prevalent in SSSS, although there were a few reports.
In Korea, among MRSA infections, community-associated MRSA (CA-MRSA) is responsible for 5.9%–18.2%.1819 Among CA-MRSA, ST72 was the predominant clone, while ST89 accounted for 0.5%–2.0% of clinical isolates in Korea.20212223 In a study of S. aureus isolates acquired from skin, soft tissue, and bone and joint infections among children in Korea during 2010–2016, there were no ST89 isolates found.22 Furthermore, ST89 is not a common clone among CA-MRSA worldwide.23 A report from Japan found that although ST89 was found in bullous impetigo due to MRSA, most isolates were MSSA.2425 In contrast with the rare distribution of ST89 in other clinical infections or other countries, our study and previous studies in Korea showed a predominance of ST89 among children with SSSS.910
The annual incidence of SSSS in all ages is estimated to be 0.39–0.56 cases/million in Europe and the USA.513 Several epidemiologic studies have shown that its incidence is highest in children less than one year of age (7.5–20.9 cases/million), which accounts for approximately 28.8%–33.6% of SSSS cases.1326 In our study, 38.5% (n = 10) of the children were less than one year of age, which was similar to previous studies. Seasonal differences for SSSS were similar to those seen in other epidemiologic studies. However, the present study showed more cases in summer and fewer cases in spring.526
There are three ETs (ETA, ETB, and ETD) in human-infecting S. aureus. ETD-producing strains are mainly isolated from cutaneous abscesses.27 Two ETs are encoded on different genetic sites: the eta gene is localized on the chromosome, while the etb gene is localized on a plasmid.28 The prevalence of S. aureus strains carrying the eta and etb genes in clinical specimens is low, with an approximate range of 0.5% to 2%.2930 However, the prevalence of eta and/or etb genes ranges from 60% to 95% in S. aureus causing skin and soft tissue infections including SSSS.63132 Worldwide trends in ET related genes are divergent regionally and temporally. The present study showed a high prevalence (53.8%) of MRSA ST89 clones which harbor the etb gene in children with SSSS. These results coincide with those of previous studies performed in other provinces in Korea.910
SSSS is a skin disease caused by toxins produced by bacteria. Skin lesions can improve by production of antitoxin antibodies as stimulated by ET. In our study, nafcillin or cefazolin was used as the empirical and final treatment in most children. Among children in which MRSA was isolated, five (20.0%) were treated with antibiotics to which the isolates were susceptible, while 20 (80.0%) were treated with antibiotics to which were not susceptible. Interestingly, all patients showed that the clinical response and the time to recovery was comparable regardless of antibiotic susceptibility. The reason for the large proportion of patients treated with antibiotics which S. aureus was not susceptible to was largely due to the fact that culture results were reported later in the course, as well as initial treatment being maintained because of improvement in clinical status. Interestingly, all children were recovered without complications from SSSS regardless of the type of antibiotics, which may suggest the recovery in SSSS may depend more on the host immune response for development of anti-toxin antibodies rather than the use of systemic antibiotics. There was a limited number of patients included in this study, and majority of cases were due to a single strain (ST89). To further address this issue, it would be desirable to measure levels of anti-toxin antibodies in the host. In addition, larger studies examining the clinical responses of patients from different age groups as well as cases related to different molecular strains are necessary.
This study has some limitations. It was conducted in three university hospitals. Therefore, the data do not represent national SSSS epidemiology. Due to the retrospective nature of the study, risk factors for acquisition of MRSA such as the history of hospitalization, usage of antibiotics, and other conditions of colonization of S. aureus were not be investigated. In addition, it was difficult to determine whether S. aureus isolated from the skin of patients with SSSS was the actual pathogen causing SSSS. However, the observed MRSA ST89 clonal predominance in the present study was in accordance with previous studies among Korean children with SSSS. This, when taken together with the fact that ST89 is not commonly found in other clinical conditions such as skin and soft tissue infections or colonization in Korea, support the possibility that ST89 is an important strain for SSSS in Korean children.
In conclusion, our data showed that the majority of S. aureus causing SSSS in this study were methicillin-resistant ST89 clones and a large proportion hold the etb gene. The predominance of MRSA suggests that antibiotics effective against MRSA should be considered when treating children with SSSS in Korea. However, clinical responses were also observed in the cases treated with non-susceptible antibiotics. Thus, the role and effectiveness of antibiotics in the treatment of patients with SSSS need to be further studied.
 XML Download
XML Download