

 PDF
PDF Citation
Citation Print
Print



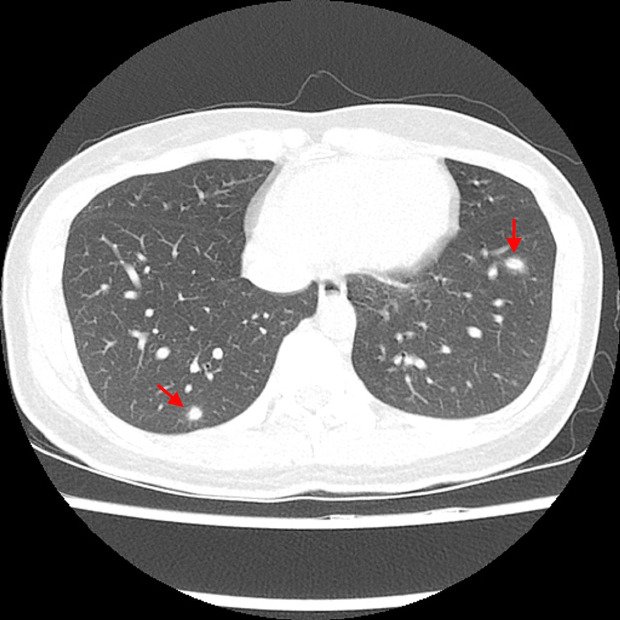
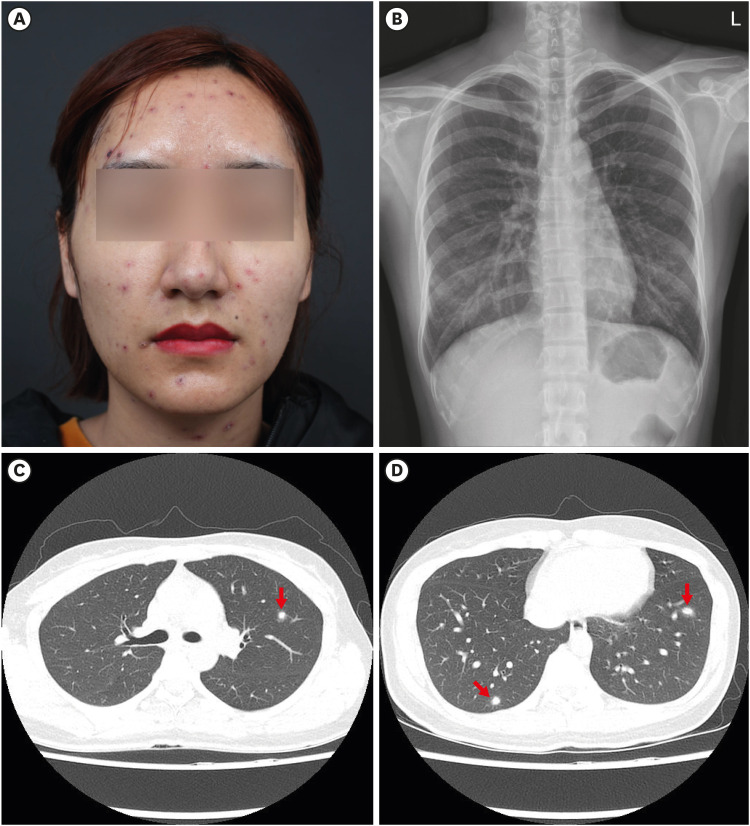
A 26-year-old female presented to the Emergency Department (ED) on March 16, 2019, with a 1-day history of fever and generalized, pruritic, maculopapular, and vesicular rash that began to appear on the face. Her 4-year-old son had been treated for chickenpox 2 weeks earlier. The patient received one dose of varicella vaccine in childhood and had no history of varicella. She had no significant medical history. At presentation, her body temperature was 37.4°C, and other vital signs were stable. Laboratory tests revealed a white blood cell count of 3,220 cells/mm3 with 3% atypical lymphocytes, a platelet count of 143,000/mm3, and an alanine aminotransferase level of 46 U/L, and a C-reactive protein of 20.57 mg/L. Chest radiography showed no definite abnormalities in both lung fields. Because the patient refused to be hospitalized for intravenous acyclovir therapy, we prescribed oral valacyclovir 1 g twice daily. She was discharged home with a plan for close follow-up in an outpatient clinic. On day 4 after discharge, the patient was afebrile, and some of the vesicular lesions had crusted (Fig. 1A); however, she complained of a mild cough and dyspnea. Repeated chest radiography (Fig. 1B) and computed tomography (CT) (Fig. 1C and D) demonstrated typical radiologic findings of varicella pneumonia in the early stages. Varicella-zoster virus (VZV) polymerase chain reaction in plasma performed at the ED was confirmed to be positive. After a 7-day course of oral valacyclovir therapy, cough and dyspnea were gradually improved and all skin lesions had fully crusted. One month later, the patient's symptoms were completely resolved, and repeated chest radiography and CT showed improvement of multiple inflammatory nodules in both lungs.
In Korea, a live attenuated varicella vaccine was first introduced in 1988 and universal one-dose varicella vaccination was recommended for children by the National Immunization Program since 2005. Despite the routine vaccine coverage, the nationwide varicella incidence in Korea has not declined substantially.1 Varicella can cause severe complications more often in adults, pregnant women, and immunocompromised hosts than in healthy children.2 Varicella pneumonia, one of the serious, life-threatening complications, occurs in 1 in 400 cases of infection among adults, compared with 0.3 in 10,000 cases of infection among children.34 Respiratory symptoms including cough, dyspnea, tachypnea, pleuritic chest pain, and hemoptysis usually develop within 1 to 6 days after the rash has appeared.56 Chest radiographs usually reveal multiple, bilateral, 1–10 mm in diameter ill-defined nodules with or without a surrounding halo of ground-glass attenuation.78 An overall mortality rate of varicella pneumonia in adults is between 10% and 30%.9 However, the clinical manifestations of varicella in vaccinated individuals are often mild.1011 It is presumed that this patient also had a mild clinical course due to past vaccination history. Therefore, to predict disease severity, it is important to check the vaccination status in immunocompetent adult patients suspected of varicella, especially if they were born between 1988 and 2005 in Korea. Also, patients who complain of new respiratory symptoms after the onset of rash should consider follow-up chest radiography with or without CT scans to confirm varicella pneumonia, even if the initial chest radiography was normal. Further large-scale studies are needed on the epidemiology, clinical features, and radiologic findings of varicella pneumonia in vaccinated adults.
 XML Download
XML Download