

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Venous thromboembolism (VTE), including pulmonary thromboembolism (PTE) and deep vein thrombosis (DVT), is a global public health problem, and its prevalence is increasing steadily.1 A substantial proportion of individuals with VTE go unrecognized; these untreated patients experience high mortality and morbidity.2 However, timely diagnosis is difficult because the initial symptoms of VTE are varied and nonspecific.3 Although several radiologic tests are useful for diagnosing VTE, they are not appropriate for screening due to limited availability, high cost, and safety issues.45
The plasma D-dimer test, which is performed easily in an outpatient clinic, is used to screen for VTE. The D-dimer test detects a degradation product of cross-linked fibrin, which is an essential component of a thrombus.5 A positive D-dimer test result suggests significant thrombus formation and degradation. Previous studies report that the sensitivity and specificity of the test range from 85%–96% and 48%–74%, respectively.6 Therefore, the D-dimer test is used widely to determine the need for confirmatory radiologic examination.5 However, the test is nonspecific and D-dimer values may increase in those who are pregnant, have recently undergone surgery, or have cancer, or systemic inflammatory conditions.78
Systemic lupus erythematosus (SLE) is an autoimmune disease characterized by damage to multiple organs caused by autoantibodies and immune complexes.9 Among autoimmune diseases, SLE conveys the greatest overall risk of VTE (3–4-fold higher than for the general population), which is caused by common occurrence of anti-phospholid (APL) antibody.10 Therefore, prompt detection of VTE in patients with SLE is highly important. However, the D-dimer test may not work well for SLE because D-dimer levels can vary depending on the degree of inflammation.11 Therefore, the present study aimed to assess the utility of the D-dimer test as a screening tool for VTE in SLE patients.
METHODS
Study subjects
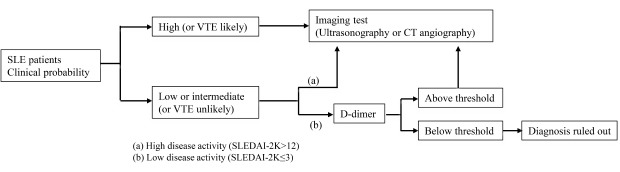
The catchment population comprised patients who underwent D-dimer testing at Seoul National University Hospital between January 2000 and July 2017. The SLE group comprised patients diagnosed with SLE according to the classification criteria revised by the American College of Rheumatology in 1997.12 After excluding patients with common rheumatologic diseases (antiphospholipid syndrome, inflammatory myositis, rheumatoid arthritis, mixed connective tissue disease, SLE, Sjögren's syndrome, systemic sclerosis, Behcet's disease and vasculitis), control subjects were randomly selected. Wells scores were calculated retrospectively from the selected SLE and control subjects, and then, we divided into “VTE unlikely” and “likely” group according to Well’s criteria predicting probability of VTE.1314 “VTE likely” patients were excluded since imaging study should be performed immediately without D-dimer test in these patients. After exclusion, a total of 276 SLE patients were enrolled. Among the control group, 4-fold age, and sex matched subjects (n = 1,104) were selected.
Data collection
All data were retrieved from electronic medical records held at Seoul National University Hospital. Demographic data, including age, sex, body mass index (BMI), previous history of VTE, major surgery within the previous 12 weeks, and comorbidities were collected. Comorbidities were categorized according to the presence of the following conditions: malignancy (receiving treatment for cancer [currently or within the previous 6 months]), hypertension (HTN), cardiovascular disease (CVD; heart failure, ischemic heart disease or coronary artery occlusive disease), atrial fibrillation, dyslipidemia, diabetes mellitus (DM), cerebral infarction, chronic kidney disease (CKD [epidermal growth factor receptor < 60 mL/min/1.73 m2]), pulmonary artery hypertension (PAH), interstitial lung disease (ILD), other lung diseases (chronic obstructive lung disease, pulmonary tuberculosis, bronchiectasis), or liver cirrhosis. We also collected the following biochemical laboratory data including white blood cell (WBC), hemoglobin, platelet, cholesterol, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), fibrinogen, prothrombin time (PT), activated partial thromboplastin time (aPTT), lupus anticoagulant (LA), and other APL antibodies (anti-β2 glycoprotein I [anti-β2 GP I] antibody or anti-cardiolipin [aCL] antibody). The D-dimer test was performed by an immunoturbidimetric assay using the ACL 3000 (Beckman Coulter Inc., Fullerton, CA, USA).15 The cut-off value for positivity of D-dimer was defined as a 500 ng/mL previously reported.16 The SLE disease activity index 2000 (SLEDAI-2K) was calculated.17 The presence of VTE (PTE and/or DVT) was confirmed by imaging tests, which include pulmonary computed tomography angiography, lung perfusion scans, and duplex ultrasonography.
Statistical analysis
Continuous variables were expressed as the mean ± standard deviation (SD) or as the median (interquartile range, IQR), while categorical variables were expressed as a number (%). The χ2 test was used to compare the categorical data between SLE patients and matched control subjects. The Kolmogorov-Smirnov test was performed to determine the normality of the distribution of parameters. Continuous values were compared using the Student's t-test or Mann–Whitney U test. The sensitivity, specificity, and positive and negative predictive values (PPV and NPV) of the D-dimer test was calculated for both groups. Receiver operating curve (ROC) analysis was performed to examine the utility of the D-dimer test as a screening tool for VTE for both groups. To examine the relationship between D-dimer levels and clinical parameters in SLE patients, multiple linear regression analyses of D-dimer levels was also conducted. Selection of covariables was performed by the stepwise method. Variables that had a P value of < 0.1 on univariate analysis were selected for multivariate analysis. Finally, to define a subgroup of SLE patients in whom D-dimer test is useful, area under the curves (AUC) were calculated from the ROC curves constructed for different subgroups. All statistical analyses were performed using SPSS (version 23.0; IBM Co., Armonk, NY, USA). P values less than 0.05 were considered significant.
RESULTS
Baseline characteristics of SLE patients and matched control subjects
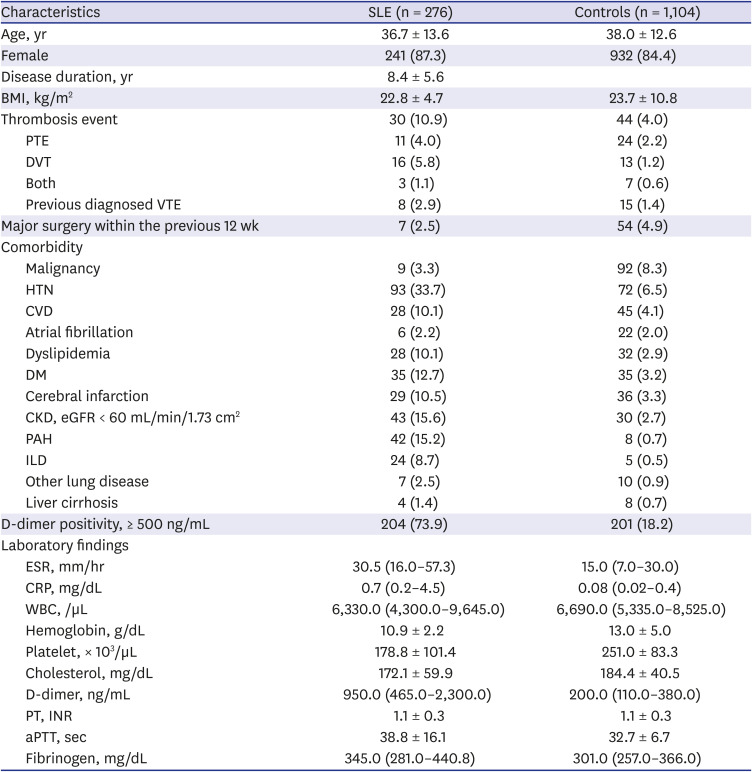
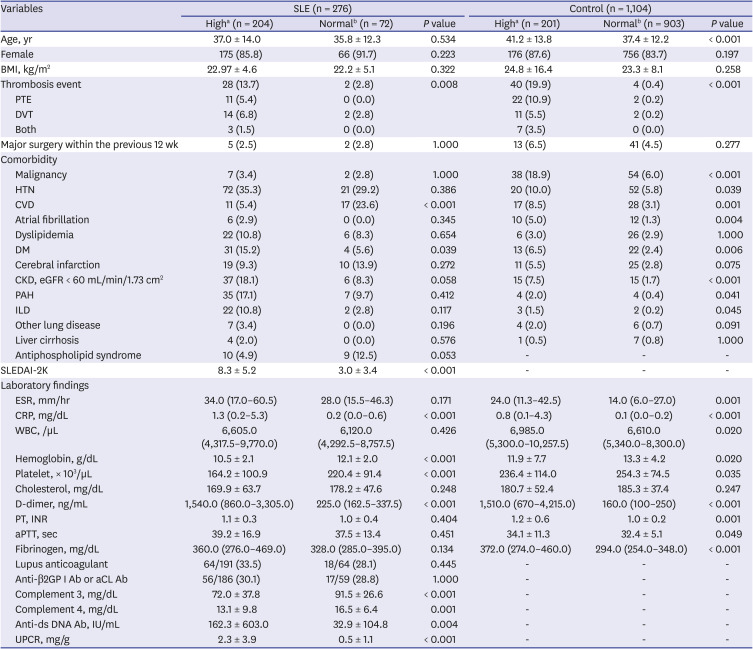
The baseline characteristics of SLE patients (n = 276) and matched control subjects (n = 1,104) are shown in Table 1. The mean ± SD age of SLE patients was 36.7 ± 13.6 years and that of controls was 38.0 ± 12.6 years. Comorbidities, including HTN, CVD, dyslipidemia, DM, cerebral infarction, CKD, PAH, and ILD were more prevalent in the SLE group than in the control group. ESR, CRP, aPTT and fibrinogen levels were higher in the SLE group than in the control group, whereas hemoglobin and platelet counts were lower in the SLE group than in the control group. The median D-dimer levels were higher in the SLE group than in the control group (950 [465.0–2300.0] vs. 200 [110.0–380.0]). Accordingly, D-dimer positivity (≥ 500 ng/mL) was more common in SLE patients than in control subjects (73.9% vs. 18.2%, respectively).
Table 1
Baseline characteristics of the study subjects
Results are expressed as the mean ± standard deviation, as the median (interquartile range), or as number (%).
SLE = systemic lupus erythematosus, BMI = body mass index, PTE = pulmonary thromboembolism, DVT = deep vein thrombosis, VTE = venous thromboembolism, HTN = hypertension, CVD = cardiovascular disease, DM = diabetes mellitus, CKD = chronic kidney disease, eGFR = epidermal growth factor receptor, PAH = pulmonary artery hypertension, ILD = interstitial lung disease, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, WBC = white blood cell, PT = prothrombin time, INR = international normalized ratio, aPTT = activated partial thromboplastin time.
Venous thromboembolisms in SLE and control groups
The incidence of VTE was higher in SLE patients than in controls (30/276, 10.9% vs. 44/1,104, 4.0%). There were 11 (4.0%) cases of PTE, 16 (5.8%) of DVT, and three concomitant case (1.1%) of PTE and DVT in the SLE patient group, compared with 24 (2.2%) PTE, 13 (1.2%) DVT, and 7 (0.6%) of both PTE and DVT cases in the control group (Table 1).
Low specificity of the D-dimer test as a screening tool for VTE in SLE patients
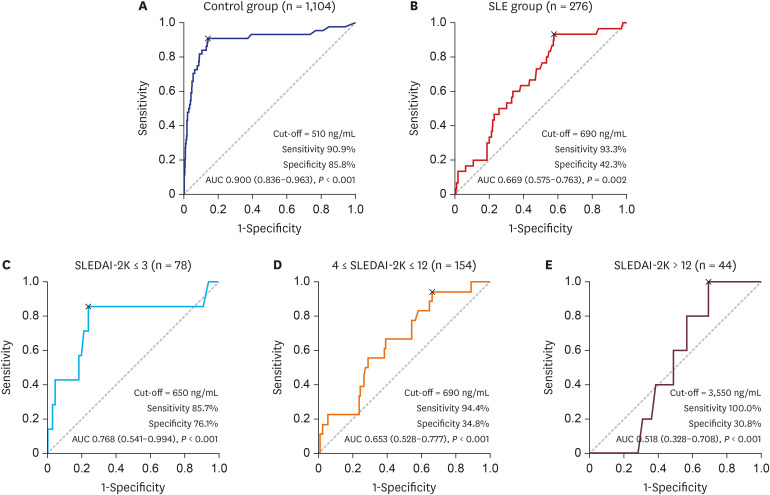
We compared D-dimer levels between SLE patients and controls with/without VTE. While D-dimer levels were similar in SLE patients with and without VTE, those were significantly different in controls (Fig. 1). We found that 204 (73.9%) of 276 SLE patients had a D-dimer level greater than the cut-off value of 500 ng/mL; of these, only 28 (13.7%) had confirmed VTE. Meanwhile, only 201 (18.2%) of 1,104 control subjects showed D-dimer more than 500 ng/mL and 40 patients (19.9%) among them were confirmed VTE. The sensitivity, specificity, PPV, and NPV of the D-dimer test for VTE in SLE patients were 93.3%, 28.4%, 13.7%, and 97.2%, respectively, compared with 90.9%, 84.8%, 19.9%, and 99.5%, respectively, in the controls (Table 2). ROC analysis for the D-dimer levels revealed that an AUC was 0.900 (95% confidence interval [95% CI], 0.836–0.963) for control subjects (Fig. 2A), but an AUC was only 0.669 (95% CI, 0.575–0.763) for SLE subjects (Fig. 2B). These findings suggest that D-dimer test for VTE was much less specific in SLE patients than in controls.
Fig. 1
D-dimer levels in SLE and control subjects according to the presence of VTE.
D-dimer levels were highly discriminative between VTE and no VTE group in control subjects. On the contrary, D-dimer levels were comparable between the two groups in SLE patients.
SLE = systemic lupus erythematosus, VTE = venous thromboembolism.
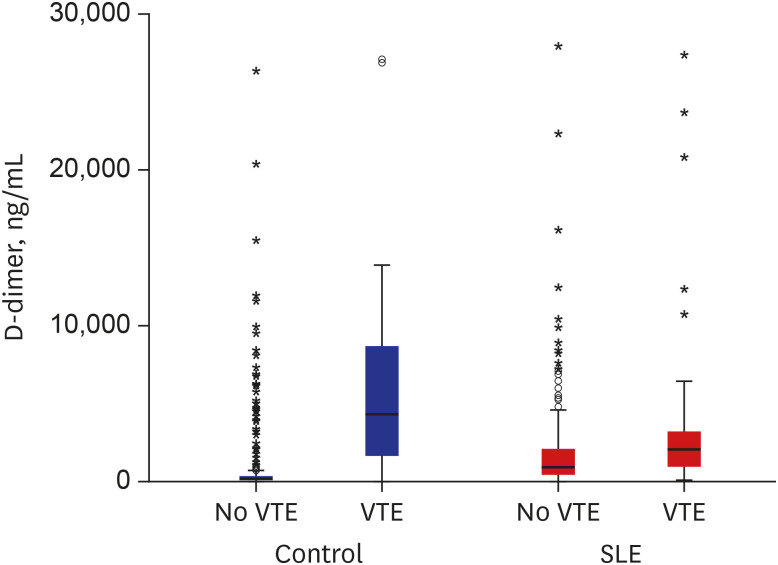
Table 2
Diagnostic utility of the D-dimer test in the SLE and control groupsa

| Variables | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|
| SLE | 28/30 (93.3) | 70/246 (28.4) | 28/204 (13.7) | 70/72 (97.2) |
| Control | 40/44 (90.9) | 899/1,060 (84.8) | 40/201 (19.9) | 899/903 (99.5) |
Fig. 2
ROC curves of D-dimer for VTE in study subjects.
On ROC curve analysis, (A) the AUC for predicting VTE was 0.900 (95% CI, 0.836–0.963) in control subjects, (B) 0.669 (95% CI, 0.575–0.763) in SLE subjects. When SLE patients were subdivided according to SLEDAI-2K, the AUC for the D-dimer in SLEDAI-2K ≤ 3 was (C) 0.768 (95% CI, 0.541–0.994), (D) 0.653 (95% CI, 0.528–0.777) in 4 ≤ SLEDAI-2K ≤ 12, (E) 0.518 (95% CI, 0.328–0.708) in SLEDAI-2K > 12.
ROC = receiver operating curve, VTE = venous thromboembolism, AUC = area under the curve, CI = confidence interval, SLE = systemic lupus erythematosus, SLEDAI-2K = SLE disease activity index-2000.
Clinical variables related to D-dimer levels in controls and SLE patients
Next, we evaluated the clinical factors affecting D-dimer levels in study subjects. Control subjects with a positive D-dimer test greater than 500 ng/mL were significantly older, had more comorbidities (including malignancy, HTN, CVD, atrial fibrillation, DM, CKD, PAH, and ILD) and showed higher levels of coagulation factors (including PT, aPTT, and fibrinogen) than those with negative D-dimer result. However, there was no significant difference in comorbidities (except CVD and DM) and levels of coagulation factors between SLE patients with positive and negative D-dimer test (Table 3).
Table 3
Variables affecting D-dimer values in the SLE group and control group
Results are expressed as the mean ± standard deviation, as the median (interquartile range), or as number (%).
SLE = systemic lupus erythematosus, BMI = body mass index, PTE = pulmonary thromboembolism, DVT = deep vein thrombosis, HTN = hypertension, CVD = cardiovascular disease, DM = diabetes mellitus, CKD = chronic kidney disease, eGFR = epidermal growth factor receptor, PAH = pulmonary artery hypertension, ILD = interstitial lung disease, SLEDAI-2K = systemic lupus erythematosus disease activity index 2000, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein, WBC = white blood cell, PT = prothrombin time, INR = international normalized ratio, aPTT = activated partial thromboplastin time, anti β2GP I Ab = anti-β2 glycoprotein I antibody, aCL Ab = anti-cardiolipin antibody, anti-dsDNA Ab = anti-double-stranded DNA antibody, UPCR = urine protein to creatinine ratio.
aHigh, D-dimer ≥ 500 ng/mL; bNormal, D-dimer < 500 ng/mL.
In SLE patients, anti-double stranded DNA antibody (anti-dsDNA Ab) titers, urine protein to creatinine ratio (UPCR), and SLEDAI-2K scores reflecting SLE disease activity were significantly higher in patients with a positive D-dimer result than those with a negative result. In addition, complement (C) 3 and C4 levels were significantly lower in patients with D-dimer levels greater than 500 ng/mL compared to those in patients with low D-dimer levels. Multiple linear regression analysis demonstrated that the SLEDAI-2K (β = 0.155; P = 0.022) was significantly associated with the D-dimer levels besides VTE (β = 0.185; P = 0.003), WBC (β = 0.200; P = 0.002), and platelet (β = −0.207; P = 0.002) in SLE patients (Table 4). These findings indicate that D-dimer levels in SLE patients are closely related with disease activity.
Table 4
Multivariate linear regression analysis of factors affecting D-dimer levels in the SLE and control groups
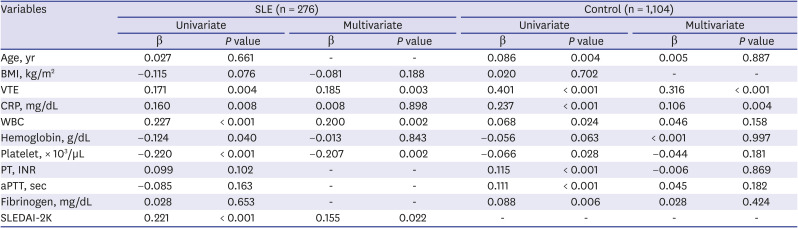
SLE = systemic lupus erythematosus, BMI = body mass index, VTE = venous thromboembolism, CRP = C-reactive protein, WBC = white blood cell, PT = prothrombin time, INR = international normalized ratio, aPTT = activated partial thromboplastin time, SLEDAI-2K = systemic lupus erythematosus disease activity index 2000.
ROC analysis of D-dimer levels in SLE patients according to disease activity
Since D-dimer level is affected by disease activity in SLE patients, we analyzed the effect of disease activity on the utility of D-dimer test for predicting VTE in SLE patients. When SLE patients were subdivided according to SLEDAI-2K, the AUC was 0.768 (95% CI, 0.541–0.994) in no flare patients (SLEDAI-2K ≤ 3) (Fig. 2C), 0.653 (95% CI, 0.528–0.777) in patients with mild to moderate flare (4 ≤ SLEDAI-2K ≤ 12) (Fig. 2D), 0.518 (95% CI, 0.328–0.708) in patients with high SLEDAI-2K (SLEDAI-2K > 12) (Fig. 2E). These findings demonstrated that in SLE patients with high disease activity (SLEDAI-2K > 12), D-dimer was less capable of predicting VTE than in those with low disease activity (SLEDAI-2K ≤ 3).
DISCUSSION
This is a case-control study to evaluate the role of D-dimer in predicting VTE in SLE patients. The results presented herein suggest that D-dimer test may not be a useful tool for the screening of VTE in SLE patients (AUC = 0.669 for the SLE group vs. 0.90 for the control group), because it is difficult to distinguish between true VTE and secondary elevation reflecting inflammation in SLE patients. However, present study also demonstrated that the D-dimer test can be useful for VTE screening in stable SLE patients.
Arterial or venous thromboembolic complications are frequent manifestations of SLE; indeed, 5%–10% of SLE patients have VTE.18 Incidence of thrombosis has been reported to be up to 51.9 per 1,000 patient-years and the risk is 3–4 fold higher than for the general population.19 This study showed that VTE was more frequently observed in SLE patients than in the control subjects (10.9% vs. 4.0%). An increased risk of thrombo-embolic complications can be due to the fact that SLE patients often experience a hypercoagulable status including positive APL antibodies, systemic inflammation, or anticoagulation deficiency.20 Previous reports have shown that inflammatory mediators, which are increased in SLE patients, can increase serum tissue factor levels and inhibit activation of protein C.2122 Patients with SLE have a deficiency in natural anticoagulant mechanisms and upregulation of coagulation factors associated with inflammatory mechanisms and endothelial damage.23 Thus, blood coagulation is easily activated in SLE patients with active inflammation.24
The D-dimer test is the standard screening tool for predicting VTE in general population with Wells probability score.142526 If VTE is ‘likely’ with Wells criteria, confirmatory imaging tests should be performed immediately, while D-dimer test should be performed to exclude VTE if it is ‘unlikely’ with Well’s criteria.142527 In this study, we found that the D-dimer levels cannot be clearly delineated between patients with and without VTE in SLE (Fig. 1), which lead to very low specificity of D-dimer test in this group. Therefore, if a clinician follows the general algorithm for VTE, then patients may be subjected to unnecessary imaging tests, which are not only costly but can be dangerous because of unnecessary radiation exposure.
False elevation of D-dimer levels can arise from different conditions such as aging, cancer, co-morbidities (including heart failure, chronic obstructive pulmonary disease, and atherosclerosis), and systemic inflammation.28293031 In this study, we found that in SLE patients, a positive D-dimer test is closely associated with high SLE disease activity, as reflected by a higher SLEDAI-2K including higher anti-dsDNA titers, low complement levels, and a high UPCR (Table 3). Therefore, utility of D-dimer test can be affected by disease activity in SLE patients; AUC value for D-dimer in ROC is high in SLE patients with low SLEDAI-2K, while it is low in patients with high SLEDAI-2K (Fig. 2C-E).
Taken together, disease activity should be considered in the interpretation of D-dimer test in SLE patients. In low disease activity, positive D-dimer test result can be regarded as in general population. So, confirmatory imaging test should be performed if D-dimer test is positive in this group of patents. However, D-dimer level can be elevated without association with VTE in SLE patients with high disease activity.
This study has several limitations. First of all, the study is retrospective in design. Therefore, some patients with VTE might have gone undetected because not all enrolled patients underwent imaging studies. However, the result of this study represents the real world situation. In addition, the study population was composed of only Koreans; therefore, the results may not be generalizable to other ethnic groups. Despite these limitations, the insights gained from this study should help clinicians use the D-dimer test more usefully in SLE patients.
In conclusion, our study demonstrated that the D-dimer test may not be useful for screening VTE in SLE patients, especially in those with high disease activity. Therefore, it may be necessary to interpret the result of the D-dimer test in relation to disease activity in patients with SLE.
 XML Download
XML Download