

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Two primary treatment modalities are used for ruptured cerebral aneurysms, surgical clipping and endovascular coiling. Since the introduction of Guglielmi detachable coils (GDCs; Boston Scientific Corp., Marlborough, MA, USA) in the early 1990s, prospective clinical studies, including the International Subarachnoid Aneurysm Trial (ISAT)1 and the Barrow Ruptured Aneurysm Trial,23 have supported an increasing role for coil embolization of ruptured aneurysms. The rapid development of endovascular coiling in recent years has been attributed to the development of coils and instruments that can overcome the shape and location challenges of aneurysms. The results of the analysis of clipping and coiling trends in Korea in recent years also show that the rate of coiling is gradually increasing.45 However, there have been no papers statistically analyzing these trends according to sex and age. Therefore, we tried to investigate recent trends in treatment for ruptured cerebral aneurysms using the age-adjusted method.
METHODS
Data acquisition
We collected data between 2010 and 2017 from the National Health Insurance Service (NHIS), the Korean Statistical Information Service (KOSIS), and the Health Insurance Review and Assessment Service (HIRA) in Korea. Annual reports of statistics from the NHIS of Korea were used. The data were collected according to the Korean Standard Classification of Disease and Cause of Death, 6th edition. We used several codes to identify the samples in this study, S4641-S4642 for surgical clipping and M1661-M1662 for endovascular coiling. We also collected the number of males and females in Korea from 2010 to 2017 from the KOSIS.
Measurement outcomes
The primary outcomes of this study were the relationships between annual trends in operation rates and structural age changes. To investigate these two outcomes, cumulative age-standardized prevalence rates per year according to age groups, cumulative age-standardized operation rates per year according to age groups, age-standardized operation rates/patients per year according to age groups, the correlation between patient rates per year and the percentage of the population, the correlation between operation rates per year and the percentage of the population, and the correlation between operations/patient rates per year and the percentage of the population were measured. We subdivided age into the following groups: less than 40 years old, 40s, 50s, and over 60 years old. We described all outcomes as rates standardized per 100,000 people using the actual general population for the relevant year.
Data analysis
The total number of males per year was calculated for each age group in Korea using data from the National Statistical Office. The total number of operations per year according to the age groups were calculated based on diagnosis codes. The cumulative patient and operation rates were analyzed according to year. Cumulative age-standardized patients and operations according to year and age groups were also analyzed. Generalized linear models (GLMs) were used for the analyses. Poisson regression analysis was used for analysis and stratification analysis by sex was used. In model 1, effect sizes of overall time trend were adjusted for age group. Model 2 was analyzed by adding interaction effect (year × age group) to model 1 to identify whether the time trend estimates differ between age groups.
The results are displayed as estimates with standard errors (SEs) and were plotted as line graphs. For age-standardization, we used the formula as follows: number of patients (for the year) × 10,000/total population (for the year). Analyses were performed for the cumulative age-standardized patient rates per 100,000 people, operation rates per 100,000 people, and procedure/patient rates according to year and age groups. GLM was used and the results were displayed as the estimated with SE and plotted as a line graph. A piecewise linear regression model was used to compare trends before and after 2011. Analyses were performed to derive the correlation coefficients between patient rates and the percentage of the population, between operation rates and the percentage of the population, and between operation rates/patient rates and the percentage of the population per year using Pearson correlation analysis. Statistically significant differences were considered for P values of less than 0.05. All data were analyzed using R software (v3.1.2; R Foundation, Vienna, Austria).
RESULTS
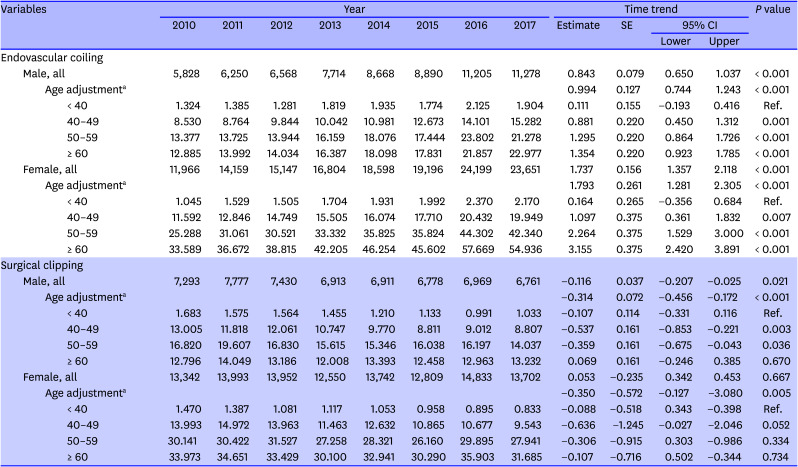
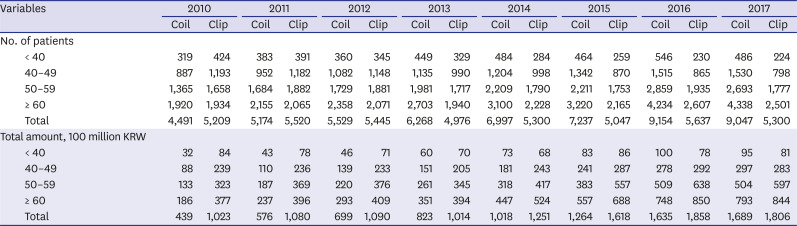
Table 1 shows the procedure trends for all aneurysm patients after age adjustment according to age groups.
Table 1
The trend for procedures of all aneurysm patients after age-adjustment according to age groups
Annual trend in coiling procedure
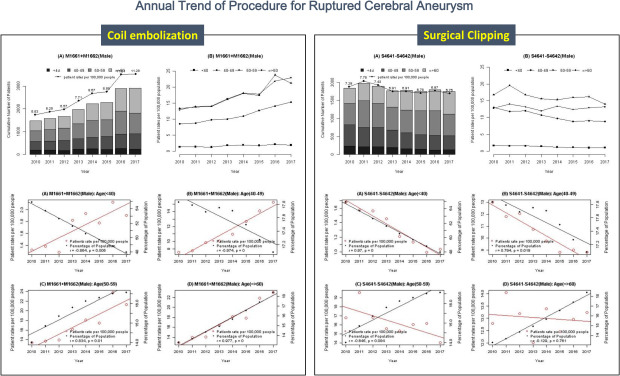
We presented the overall trends of each procedures in male and female groups in Fig. 1, and the analysis of the patients rate and the percentage of population by year according to each age group in Fig. 2.
Fig. 1
Overall trends of the coiling and clipping procedures in male and female patients. (A) Overall trends of the coiling procedures in male patients. The cumulative number of patients regardless of the population or age group showed an increase over the study period. The patient rate per 100,000 population showed an increase in all age groups, except in patients less than 40 years old. (B) Overall trends of the coiling procedures in female patients. The cumulative number of patients regardless of the population or age group showed an increase. The patient rate per 100,000 population showed an increase in all age groups, except for in patients younger than 40 years, which showed a steady trend. (C) Overall trends of the clipping procedures in male patients. There was no increasing or decreasing trend in the cumulative number of patients over the study period. The patient rates also show trends toward decreases or no change. The patient rates by year showed decreases in all age groups. (D) Overall trends of the clipping procedures in female patients. The cumulative number of patients and the patient rates showed decreases or no change.
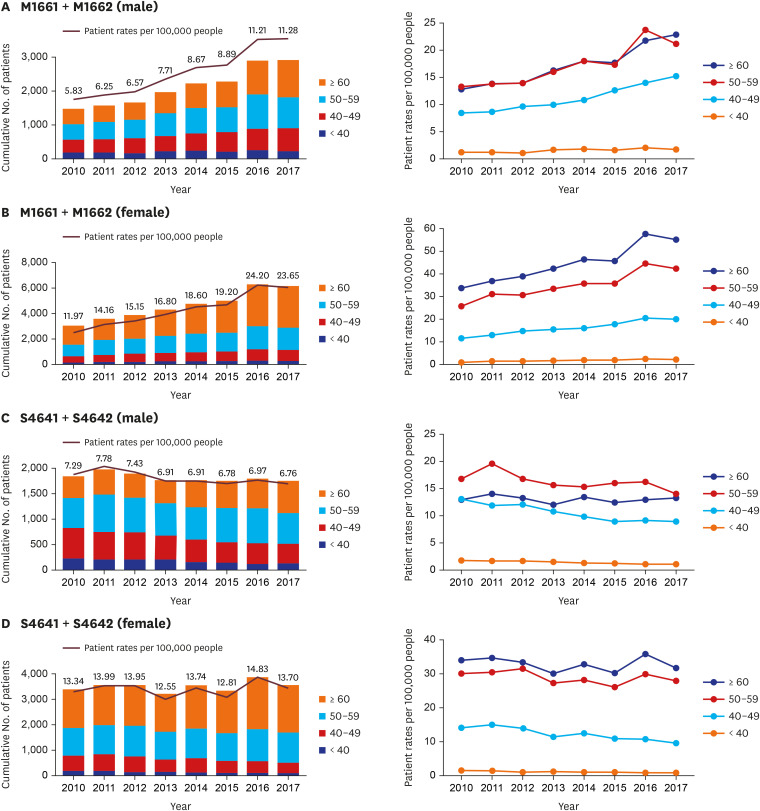
Fig. 2
Analysis of the patient rates and the percentage of the population by year according to each age group. (A) Male patients treated by coiling procedure. There was a negative correlation in the under 40 and 40s age groups and a positive correlation in the 50s and over 60-year-old age groups with statistical significance in all age groups. (B) Female patients treated by coiling procedure. There was a negative correlation in the under 40 and 40s age groups and a positive correlation in the 50s and over 60 age groups with statistical significance in all age groups. (C) Male patients treated by clipping procedure. There was a positive correlation in patients under 40 and in the 40s age group and a negative correlation in the 50s and over 60 years age groups. It was statistically significant in the under 40 and 40s age groups. (D) Female patients treated by clipping procedure. There was a positive correlation in the under 40 and 40s age groups and a negative correlation in the 50s and over 60 years old groups. It was statistically significant in the under 40 and 40s age groups.
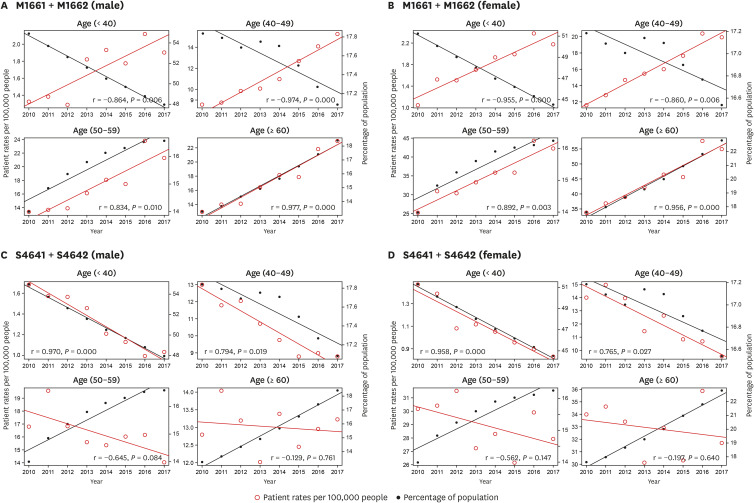
Fig. 1A shows the overall trends of coiling procedures in male patients. The cumulative number of patients regardless of the population or age group showed an increase over the study period from 5,828 in 2010 to 11,278 in 2017. The patient rate per 100,000 population showed an increase in all age groups, except in patients less than 40 years old. The patient rates by year showed an increase in all age groups indicated by a red line in the figure, as shown in Fig. 2A. The percentage of the population by year showed a decrease in patients under 40 and in the 40s age group and increases in the 50s and over 60-year-old groups. In analysis of the correlation between the patient rates and percentage of the population by year, there was a negative correlation in the under 40 and 40s age groups and a positive correlation in the 50s and over 60-year-old age groups (r = 0.864, P = 0.006 in under 40s; r = 0.974, P = 0 in 40–49; r = 0.834, P = 0.01 in 50–59; and r = 0.977, P = 0 in over 60s). The correlation was statistically significant in all age groups.
Fig. 1B shows the overall trends in coiling procedures in female patients. As with coiling in male patients, the cumulative number of patients regardless of the population or age group showed an increase over the study period from 11,966 in 2010 to 24,199 in 2017. The patient rate per 100,000 population showed an increase in all age groups, except for in patients younger than 40 years, which showed a steady trend. The correlation analysis showed the same result as in male patients, as shown in Fig. 2B. The patient rate by year showed an increase in all age groups and the percentage of the population by year showed a decrease in patients under 40 and the 40s age group and increases in the 50s and over 60 age groups. In the correlation analysis between the patient rates and the percentage of the population by year, there was a negative correlation in the under 40 and 40s age groups and a positive correlation in the 50s and over 60 age groups (r = 0.955, P = 0 in under 40s; r = 0.86, P = 0.006 in 40–49; r = 0.892, P = 0.003 in 50–59; and r = 0.956, P = 0 in patients over 60). The correlation was statistically significant in all age groups.
The results showed that, in both male and female patients, although the populations under 40 and in the 40s decreased, the proportion of patients in those age groups who underwent endovascular coiling increased. The population of patients in their 50s and over 60 increased and the patient rates also increased.
Annual trend in clipping procedures
Fig. 1C shows the overall trends in clipping procedures in male patients. There was no increasing or decreasing trend in the cumulative number of patients over the study period. The patient rates also show trends toward decreases or no change. The patient rates by year showed decreases in all age groups. In the correlation analysis between the patient rates and the percentage of the population by year, there was a positive correlation in patients under 40 and in the 40s age group and a negative correlation in the 50s and over 60 years age groups, as shown in Fig. 2C (r = 0.97, P = 0 in under 40s; r = 0.794, P = 0.019 in 40–49; r = 0.645, P = 0.084 in 50–59; and r = 0.129, P = 0.761 in patients over 60). It was statistically significant in the under 40 and 40s age groups.
Fig. 1D shows the overall trends in clipping procedures in female patients. As with clipping in male patients, the cumulative number of patients and the patient rates showed decreases or no change. The correlation analysis showed the same result as in male patients, as shown in Fig. 2D. There was a positive correlation in the under 40 and 40s age groups and a negative correlation in the 50s and over 60 years old groups (r = 0.958, P = 0 in under 40s; r = 0.765, P = 0.027 in 40–49; r = 0.562, P = 0.147 in 50–59; and r = 0.197, P = 0.64 in patients over 60). It was statistically significant in the under 40 and 40s age groups.
This means, in both male and female patients, the population of patients under 40 and in the 40s group decreased and the rate of patients who underwent surgical clipping also decreased. The population of patients in the 50s and over 60 groups increased, but the patient rate decreased.
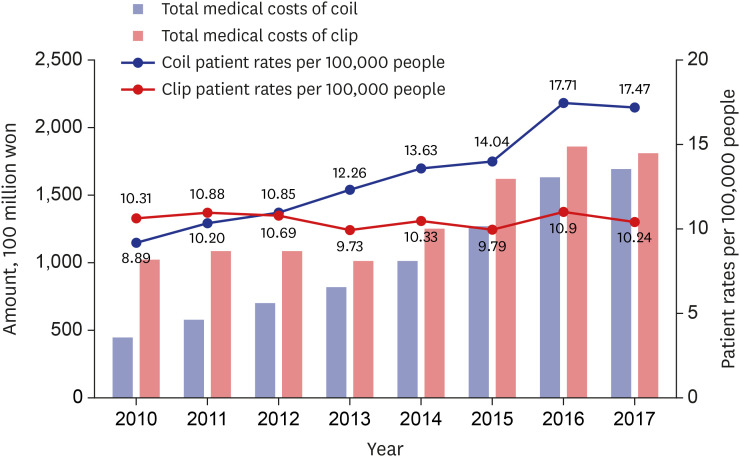
Trends in medical expenses
Table 2 shows the trends in medical expenses for endovascular coiling and surgical clipping acquired from HIRA. Fig. 3 shows that both the cost for clipping and coiling increased. Specifically, the increasing trend in medical expenses for endovascular coiling was more rapid than that for surgical clipping.
Table 2
The trend of medical expenses of endovascular coiling and surgical clipping
DISCUSSION
This research showed the national trend in endovascular coiling and surgical clipping with age shifts over the last eight years. To our knowledge, this is the first study to consider age shifts in comparing the trends between endovascular coiling and surgical clipping.
Since the introduction of endovascular treatment for intracranial aneurysms, there have been considerable changes in its uses and outcomes.67 In 2002, the results of the ISAT study performed as a multicenter phase III trial were published.1 The ISAT study compared endovascular and surgical treatments for 2,143 patients suitable for both treatments. Further patient recruitment was discontinued prematurely because the interim analysis showed a significantly low occurrence of disability and death in the endovascular treatment group. The surgical treatment group showed a higher probability of being dependent or dying compared to the endovascular treatment group (31% of 793 patients vs. 24% of 801 patients). Since the publication of the ISAT results, American and European guidelines have recommended endovascular treatment for ruptured cerebral aneurysms.89 In 2003, the Food and Drug Administration expanded its guidelines to permit the use of GDC coils for all brain aneurysms.10
After that, a steadily increasing percentage of patients have been treated by endovascular methods. The cumulative number of patients, as well as the ratio of patients undergoing endovascular coiling according to the population per year, jumped over the study period.111213 In 2010, Kim et al.14 performed a nationwide multicenter survey and reported the treatment of unruptured aneurysm. In their study, 49.9% of unruptured aneurysms were treated with clipping, 48.6% with coiling, and the remaining 0.5% with combined method. The increase in coiling procedures can be explained by the following reasons. The first reason is technological development. Widespread application of the coiling procedure due to advancements in treatment materials and techniques, as well as assisted coil embolization using stents or balloons, is more common.1516171819 The other cause is an increase in the experience of surgeons and institutions.2021 In recent years, coil embolization has been widely performed in secondary general hospitals and not limited to tertiary university hospitals.2223
Previous studies have compared the trends in endovascular coiling and surgical clipping using HIRA data.24 One study showed that neurointervention, including not only endovascular coiling for aneurysm, but also mechanical thrombectomy for ischemic stroke, and stenting and angioplasty for carotid and intracranial artery stenosis, continued to increase. Our research differed from previous studies in that it reflected changes in demographics by age groups. Our findings showed that the proportion of people under 50 decreased and that of people over 50 increased in the overall demographics. Endovascular coiling was significantly increased in all age groups and surgical clipping was decreased in all age groups, especially in patients under 50 years of age. Moreover, the number of patients undergoing surgical clipping was significantly decreased with a positive correlation. Considering these trends and the increasing trend in the elderly population, the area of endovascular coiling can be expected to increase gradually compared to surgical clipping.
This finding is not just limited to Korea, but is a global trend. In a 25-year observational study in the United States, the percentage of coiling was 3% in 1991 and jumped to 42% in the 2010s.25 In a European study published in the UK, the number of patients undergoing surgical clipping decreased from 51% to 31%, whereas the number of patients receiving endovascular coiling increased from 35% to 68% since the ISAT study results were reported.26
Our study revealed that the medical expense of coiling was higher than that of clipping, in spite of the shorter hospital stay and lower procedure cost in Korea. In Korea, the current procedure charge is 3,040,038 KRW (S4641, simple clipping) and 3,516,663 KRW (S4642, complex clipping) for surgical clipping, which is higher than that of endovascular coiling (M1661, assisted coiling; M1662, simple coiling). The cause of the higher cost of coiling might be associated with the medical devices themselves.2728 Under the current insurance system in Korea, both the total medical cost and the patient burden cost of endovascular coiling are higher than those of surgical clipping.29 In the previous study, it was found that in the case of surgical clipping, the hospitalization fee including the intensive care unit cost, and in the case of endovascular coiling, the cost of surgical material including multiple coils accounted for the largest portion.30
The strength of our study was statistical analysis using age-standardization by year. However, because we used data based on diagnostic codes and billed medical expenses, it did not reflect aneurysm information and cannot exclude the possibility of duplicated or missing data. In addition, because data acquisition was done using prescription codes, a separate analysis of ruptured aneurysms and unruptured aneurysms could not be performed. This is another limitation of this study that the unruptured aneurysms accompanying subarachnoid hemorrhage were not clearly excluded. Coil embolization is currently being performed by both neurosurgeons and interventional neuroradiologists, and selection bias due to the fact that neuroradiologists will prefer coils over clips should be considered. This study does not reflect the size of the hospital, so the fact that the coiling procedure in secondary hospitals has recently increased is another factor that can affect bias. Also, because of the nature of the data obtained from NHIS, KOSIS, and HIRA, we could not analyze procedure-related complications and long-term prognosis according to treatment modality because it was not possible to obtain complete information of the treatment process. In the same vein, because the variables related to the procedural complication were not considered, the cost of each item including procedure charge, medical device, and hospitalization cost, could not be analyzed from the total medical cost.
In conclusion, there was a significant increase in the proportion of patients with ruptured aneurysms undergoing endovascular coiling between 2010 and 2017, whereas the use of surgical clipping decreased. The endovascular coiling was significantly increased in all age groups and surgical clipping was decreased in all age groups, especially in patients under 50 years of age.
 XML Download
XML Download