

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome virus 2 (SARS-CoV-2), was first reported in China on December 31, 2019. Since then, it has spread throughout the world; consequently, the World Health Organization declared the COVID-19 outbreak as a pandemic on March 12. As of June 13, the pandemic disease had spread to 215 countries, resulting in approximately 7.5 million cases and over 423,000 deaths.1 In Korea, the first case of COVID-19 was confirmed on January 20.2 As of June 15, there were 12,121 confirmed cases of COVID-19, with 277 deaths.3
The clinical spectrum of COVID-19 encompasses asymptomatic infection, mild upper respiratory tract illness, pneumonia that may result in respiratory failure, multi-organ failure, and death. Most infections are non-severe: of 44,500 laboratory-confirmed cases, 81% were mild (no or mild pneumonia) disease.4 However, the clinical outcomes of patients with severe pneumonia vary widely. For example, in China, the case-fatality ratio (CFR) among critical cases was 49.0% (1,023/2,087).4 In the Lombardi region of Italy, 26% (405/1,581) patients admitted to the intensive care unit died.5 In New York City, 24.3% (665/2,741) patients were discharged to hospice care or died.6 In contrast, the overall CFR in Korea is 2.3%. The observed differences in clinical outcomes and CFRs in patients with COVID-19 in various countries may be related to patient demographics, surge capacity of the healthcare system, and medical care quality, as well as the case definition of COVID-19.
Towards a better response to the next wave of the pandemic, the clinical course and outcomes of COVID-19 patients need to be defined. Here, we have described the clinical characteristics, temporal progression, and fatality rate of COVID-19 in a large cohort of patients hospitalized during the first wave of the epidemic in Korea.
METHODS
Data sources
On February 3, 2020, to cope with the public health crisis caused by the COVID-19 pandemic, the Korea National Committee for Clinical Management of COVID-19 (KNCCMC) was founded. The KNCCMC consisted of 59 infectious disease specialists and attending physicians of patients with COVID-19 in Korea. In collaboration with the Korea Centers for Disease Control and Prevention (KCDC), the KNCCMC constructed a registry to collect clinical data of patients hospitalized with COVID-19. The KCDC requested that all of the designated hospitals for COVID-19 treatment were to submit clinical data to the registry.
For the registry, we developed a standardized clinical record form (CRF) that was modified from the World Health Organization Global 2019-novel coronavirus clinical characterization CRF.7 Clinical severity, based on an eight-category ordinal scale (described below), was also assessed every day. Based on the standardized CRF, the attending physicians of each participating hospital extracted data from medical records and entered them into a web-based, clinical research management system of the KCDC (http://icreat.nih.go.kr). If the core data were missing, requests for clarification were sent to the attending physicians. Given the high workload of the physicians, the laboratory results were not included in the data extraction request.
For this study, we extracted data from the registry for patients who had been confirmed to have COVID-19 between January 21, 2020 and May 31, 2020; the data cutoff point was June 1, 2020. For national epidemiologic data, we used publicly available data from the KCDC.8
Study definitions
According to the definition of the KCDC,8 a confirmed case was defined as a patient with a positive result in the real-time reverse transcription polymerase chain reaction (rRT-PCR) assay based test for SARS-CoV-2 in upper respiratory specimens (nasopharyngeal and oropharyngeal swabs), with or without a lower respiratory specimen (sputum), regardless of symptoms. The criteria for discharge from hospital and ending isolation were: 1) symptomatic improvement and afebrile; and 2) rRT-PCR negative tests at 24 hours intervals.
To measure the clinical progression and recovery of a patient with COVID-19, we modified an ordinal scale and defined the severity scores as follows9: 1) no limitation of daily activities; 2) limitation of daily activities but no need for supplemental oxygen therapy; 3) need for supplemental oxygen therapy via nasal cannula; 4) need for supplemental oxygen therapy via facial mask; 5) need for high-flow supplemental oxygen therapy or noninvasive mechanical ventilation; 6) need for invasive mechanical ventilation; 7) multi-organ failure or the need for extracorporeal membrane oxygenation (ECMO) therapy; 8) death. Recovery was defined as a score of 1 or 2, or discharge to home and release from isolation.
Statistical analysis
Baseline patient characteristics, treatments, and clinical course were presented as frequencies with percentages for categorical variables, and as the median with interquartile range (IQR; 25th, 75th percentiles) for continuous variables.
As data collection is ongoing, we provided the number of patients for whom information was collected in each variable as denominator. Categorical variables were compared using the χ2 test, although Fisher's exact test was used when the data were sparse. Continuous variables were compared using the Kruskal-Wallis test. All tests were two-tailed, and results with P values of < 0.05 were considered statistically significant. All data preparation and statistical analyses were conducted by using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
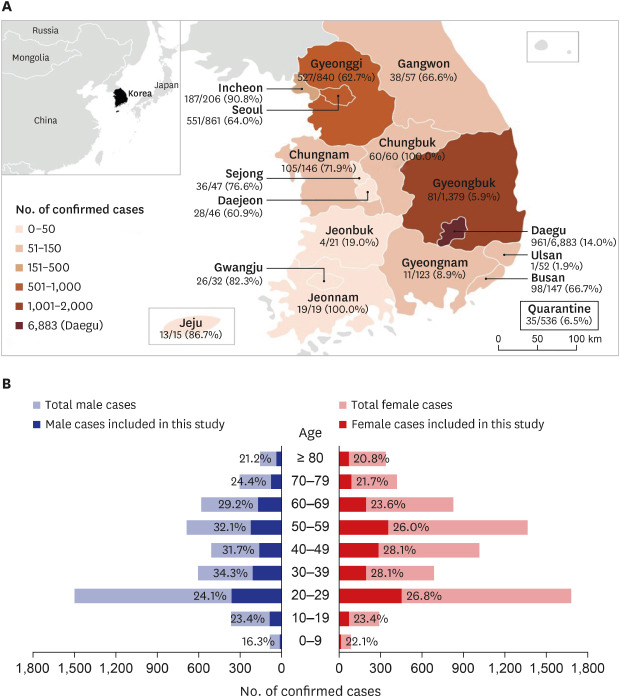
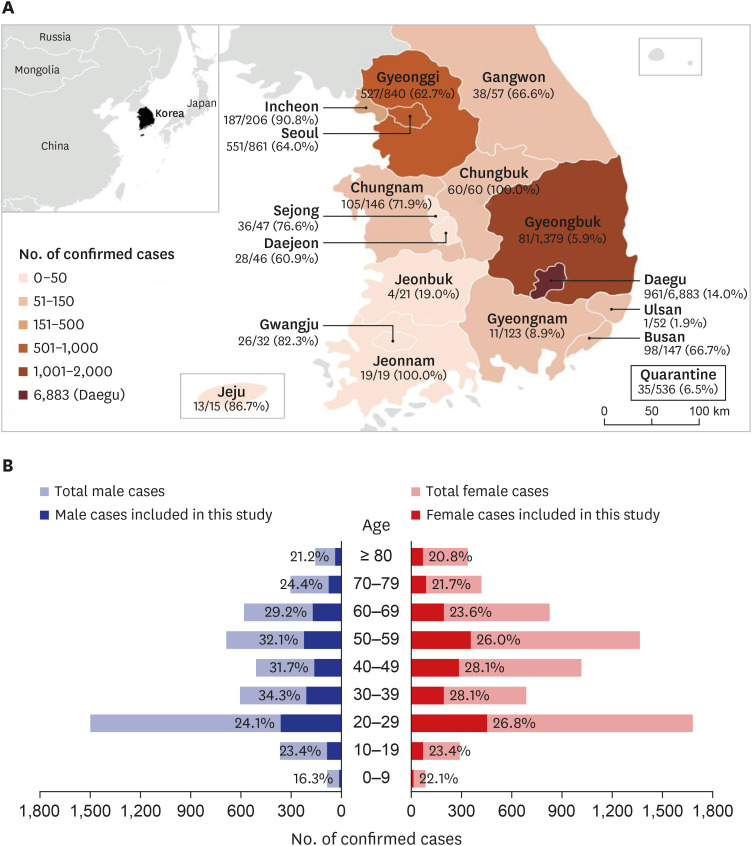
In total, 11,503 patients were confirmed to have COVID-19 before May 31, 2020; of these, 3,060 (26.6%) patients were included in this study. Of the 8,262 patients in Daegu city and Gyeongbuk province, where a large cluster of cases related to a religious group had occurred, only 1,042 (12.6%) patients were included (Fig. 1A). For each age group, approximately 20%–30% of the total number of patients in each age group was included (Fig. 1B).
Fig. 1
Geographic and demographic distribution of patients with COVID-19 in Korea, as of May 31, 2020. (A) The map shows geographical distribution of patients with COVID-19 in Korea, as of May 31, 2020. The numerator denotes the number of patients who were included in this study and the denominator denotes the number of laboratory-confirmed COVID-19 cases for each city and province. (B) Age and sex distribution. Dark bars and proportions denote cases included in this study.
COVID-19 = coronavirus disease 2019.
The median age of the patients was 43 years; 64 (2.1%), 1,515 (49.5%), 1,081 (35.4%), and 398 (13.0%) of the 3,058 patients were < 15 years of age, 15–44 years of age, 45–64 years age, and 65 years of age and older, respectively. In total, 1,334 (43.6%) patients were male (Table 1). The median time from illness onset to hospital admission was 5 days. The median time from illness onset to diagnosis was 4 days.
Table 1
Baseline demographic and clinical characteristics
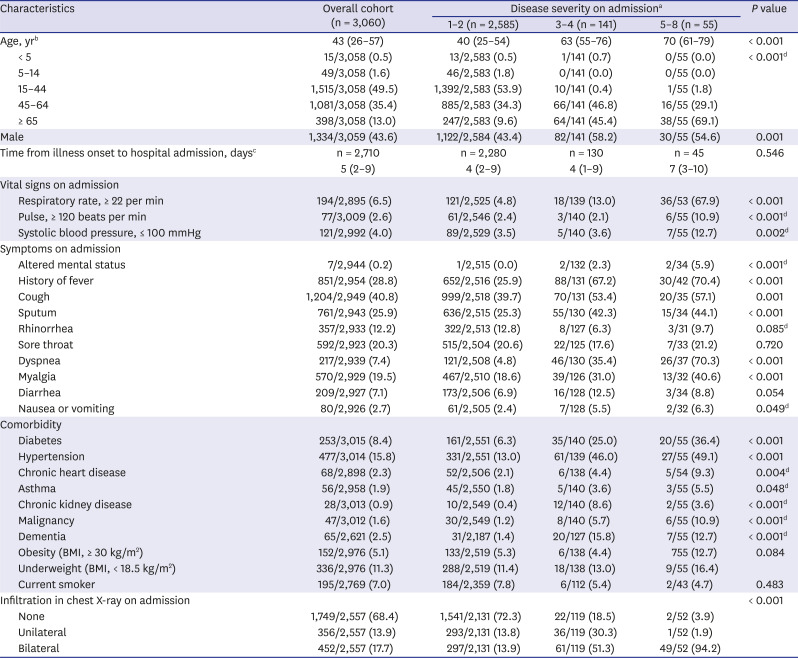
Data are presented as median (interquartile range) or number (%), unless otherwise indicated.
BMI = body mass index, ECMO = extracorporeal membrane oxygenation.
a1, no limitation of daily activities; 2, limitation of daily activities but no need for supplemental oxygen therapy; 3, need for supplemental oxygen therapy via nasal cannula; 4, need for supplemental oxygen therapy via facial mask; 5, need for high-flow supplemental oxygen therapy or non-invasive mechanical ventilation; 6, need for invasive mechanical ventilation; 7, multi-organ failure or need for ECMO therapy; 8, death. Patients with no disease severity score on admission day (279, 9.1%) were excluded from this analysis; bData regarding age were missing for 2 patients (0.1%); cData regarding illness onset were missing for 350 patients (11.4%); dFisher's exact test.
On the day of admission, disease severity scores for patients were 1–2, 3–4, and 5–7 in 2,585 (93.0%), 141 (5.0%), and 55 (2.0%) patients, respectively (total 2,781 patients). The median ages of the patients with disease severity scores of 1–2, 3–4, and 5–7 were 40, 63, and 70 years, respectively. In patients of 45–64 years of age, 1.7% (16/967) presented with a disease severity score of 5–8, whereas in patients of 65 years of age or older, 10.9% (38/349) patients presented with a disease severity score of 5–8.
The most common symptoms on admission were cough (40.8%), sputum (25.9%), and sore throat (20.3%). Only 851 (28.8%) of the 2,954 patients had a history of fever; diarrhea was rather uncommon (7.1%). Chest radiography showed no abnormality in 1,749 (68.4%) of the 2,557 patients. The most common comorbid conditions were hypertension (15.8%), diabetes (8.4%), and smoking (7.0%).
Antiviral agents were administered to 1,471 (48.1%) of the 3,060 patients: 1,108 (36.2%) received lopinavir/ritonavir, and 652 (21.3%) received hydroxychloroquine (Table 2). Sixty (2.0%) patients were treated with invasive mechanical ventilation. The median time from illness onset to the initiation of invasive mechanical ventilation was 8 days (IQR, 4–11 days). One-hundred and forty-eight (4.8%) patients were admitted to the intensive care unit. At the time of data cutoff (June 1, 2020), 2,421 (79.1%) of the 3,060 patients had been discharged, and 32 (1.1%) patients had died. The median time from illness onset to death was 5 days (IQR, 4–9 days).
Table 2
Treatments and clinical outcomes according to disease severity on admissiona
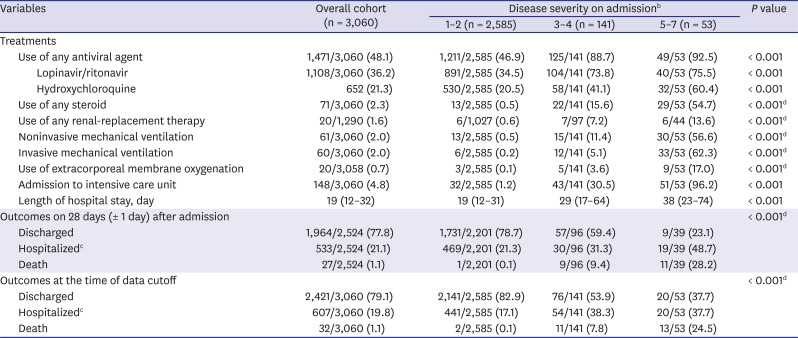
Data are presented as median (interquartile range) or number (%), unless otherwise indicated.
ECMO = extracorporeal membrane oxygenation.
aPercentages may not total 100 owing to rounding. Patients with no disease severity score on admission day (279, 9.1%) or who died on admission day (2, 0.1%) were excluded from this analysis; b1, no limitation of daily activities; 2, limitation of daily activities but no need for supplemental oxygen therapy; 3, need for supplemental oxygen therapy via nasal cannula; 4, need for supplemental oxygen therapy via facial mask; 5, need for high-flow supplemental oxygen therapy or non-invasive mechanical ventilation; 6, need for invasive mechanical ventilation; 7, multi-organ failure or need for ECMO therapy; cIncluding the patients hospitalized for isolation purposes, even if their severity score had improved to 1 or 2; dFisher's exact test.
Of the 1,905 patients with a disease severity score of 1–2 on admission, by illness day 28, the severity score had progressed to 3–7 in only 8 (0.4%) patients, and none died (Table 3). Of the patients with a disease severity score of 3–4, 42 (38.9%) of the 108 patients and 65 (71.4%) of the 91 patients had recovered by illness day 14 and day 28, respectively. Of the patients with a disease severity score of 5–7, by illness day 28, only 7 (19.4%) of the 36 patients recovered, and 8 (22.2%) patients died. None of the 1,324 patients of < 50 years of age died, whereas 0.5% (2/375), 0.9% (2/215), 5.8% (6/104), and 14.0% (7/50) of patients of 50–59, 60–69, 70–79, and ≥ 80 years of age died, respectively, by illness day 28 (Table 4). The clinical outcomes at hospital day 28 according to disease severity on admission are shown in Supplementary Table 1.
Table 3
Clinical outcomes according to disease severity on admissiona
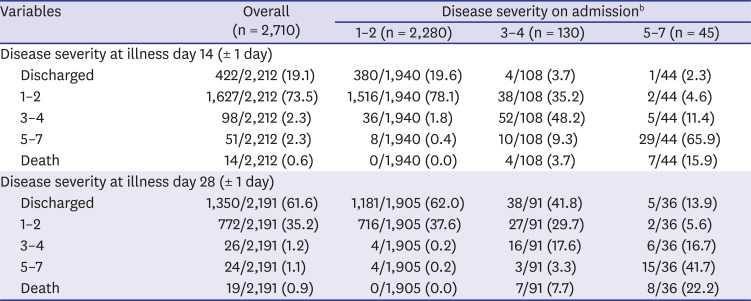
Data are presented number (%).
ECMO = extracorporeal membrane oxygenation.
aPercentages may not total 100 because of rounding. Patients without a disease severity score on admission day (279, 9.1%) or died on admission day (2, 0.1%) were also excluded from this analysis; b1, no limitation of daily activities; 2, limitation of daily activities but no need for supplemental oxygen therapy; 3, need for supplemental oxygen therapy via nasal cannula; 4, need for supplemental oxygen therapy via facial mask; 5, need for high-flow supplemental oxygen therapy or non-invasive mechanical ventilation; 6, need for invasive mechanical ventilation; 7, multi-organ failure or need for ECMO therapy.
Table 4
Clinical outcomes according to age groupa
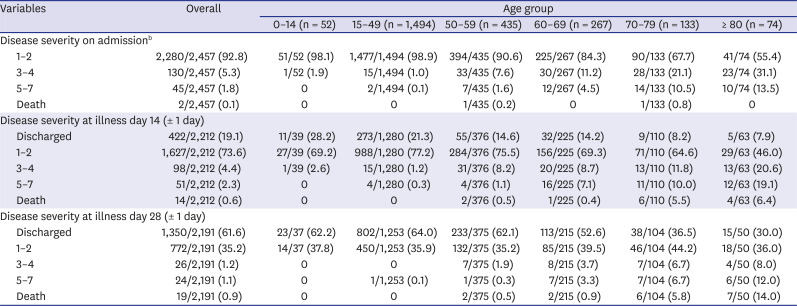
Data are presented number (%).
ECMO = extracorporeal membrane oxygenation.
aPercentages may not total 100 because of rounding. Patients with no data on illness onset (350, 11.4%), disease severity score on admission day (279, 9.1%), or age (2, 0.1%) were excluded from this analysis; b1, no limitation of daily activities; 2, limitation of daily activities but no need for supplemental oxygen therapy; 3, need for supplemental oxygen therapy via nasal cannula; 4, need for supplemental oxygen therapy via facial mask; 5, need for high-flow supplemental oxygen therapy or non-invasive mechanical ventilation; 6, need for invasive mechanical ventilation; 7, multi-organ failure or need for ECMO therapy.
DISCUSSION
In this report, we have described the clinical characteristics and disease progression of 3,060 patients hospitalized with laboratory-confirmed COVID-19 in Korea, between January and May 2020, inclusive. The median age of the patients was 43 years of age. Almost all patients of < 50 years of age with COVID-19 recovered without supplemental oxygen, whereas by illness day 28, 0.5%, 0.9%, 5.8%, and 14% of patients of 50–59, 60–69, 70–79, and 80 years of age and older, respectively, died. Of the patients who needed noninvasive or invasive mechanical ventilation, 24.5% died.
The most common symptoms on admission were cough (40.8%), sputum (25.9%), and sore throat (20.3%). Only 28.8% of the enrolled patients had a history of subjective fever, and diarrhea was uncommon (7.1%). Radiologic pneumonia was not evident on simple chest radiography in 68.4% of patients. Our previous study also showed that patients with radiologic pneumonia did not feel unwell and were able to carry on their daily activities (“walking pneumonia”).10 As the presenting symptoms were non-specific, the early detection and isolation of patients with COVID-19 was challenging.11
Disease severity on hospital admission was mild in 91% of patients, and almost all of them recovered without supplemental oxygen. In China, the proportion of mild disease (i.e., no pneumonia and mild pneumonia) was 81% (in a study of 44,415 patients4), and they recovered within approximately 2 weeks.12 Previous studies showed that the severity of COVID-19 increased with age.613 In our study, half of the patients were 15–44 years of age; and only 13% were 65 years of age or older. This age distribution may reflect aggressive contact tracing and the comprehensive testing of a cluster of members in the Shincheonji religious group, of which the majority comprised young adults.14
Our study showed that disease severity on hospital admission increased with age. The fatality rate also increased with age. These results were in line with the estimated case fatality rates in China, which was 6.4% in patients of ≥ 60 years of age, and increased to 13.4% in patients of ≥ 80 years of age.13 In contrast, in the New York City area, the fatality rate in patients of ≥ 65 years of age who did not receive mechanical ventilation was 26.6%.15 In the Lombardy region in Italy, the fatality rate in patients of 64 years of age and older admitted to the intensive care unit was 36%.5 The differences in mortalities among the countries may be explained by the differences in the prevalence of the comorbid conditions of the patients, as well as overwhelmed healthcare systems.
Few natural history studies have reported the clinical progression of patients with COVID-19. In our study, 98% of the patients who did not need supplemental oxygen on admission recovered by illness day 14, and no patients died. Of the patients requiring supplemental oxygen via nasal cannula or facial mask, 71.5% recovered and 7.7% died. This recovery rate was congruent with that from the ACTT-1 remdesivir trial,16 which reported that 70.2% of the patients in the placebo arm who required supplemental oxygen recovered. Our data suggested that patients of < 50 years of age and those who did not need supplemental oxygen at presentation may safely be treated at outpatient clinics. Indeed, during the height of the COVID-19 epidemic in Korea, the government decided to prioritize treatment of severe cases at hospitals,17 and mild cases were successfully managed at the designated/repurposed facilities in the community.18
There are several limitations in this study. First, we were not able to extract laboratory data for this study, as many clinicians from the participating hospitals were overburdened owing to the heavy burden of clinical activities. There were also many missing values for clinical progression data. However, before the sudden increase of the epidemic curve in Korea, we compiled detailed laboratory, radiologic, and virus shedding data from the first 28 patients with COVID-19 and reported these data.10 Second, in Korea, a huge cluster of cases related to a religious group had occurred in Daegu city and Gyeongbuk province, and health system in the region was overwhelmed during late February to March. But, only 12.6% of the patients were included in this study, therefore our study might under-represent severe cases from the region. Third, some of our patients were treated with hydroxychloroquine and lopinavir/ritonavir; however, these were later proven to be of little benefit.1920 Approximately half of the severe patients received steroid treatment, and this might affect the outcomes. Lastly, most people wore face masks in Korea, and this practice might reduce inoculum size of infecting viruses and therefore the severity of pneumonia.
In conclusion, during the first wave of the COVID-19 epidemic in Korea, patients with COVID-19 who were of < 50 years of age recovered without supplemental oxygen. Among patients of ≥ 50 years of age, the fatality rate increased with age, reaching 14% in patients of ≥ 80 years of age. Our results may help to better prepare health system and clinical management for the next waves of the COVID-19 pandemic.
 XML Download
XML Download