

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ischemic heart disease (IHD) is one of the most burdensome chronic diseases in Korea.1 With an improvement in survival after IHD,2 more efforts are being channeled towards secondary prevention.3 Cardiac rehabilitation (CR), an aspect of secondary prevention program, is highly recommended after IHD in national clinical practice guidelines,456 (based on the evidence of CR) for improving clinical outcomes.789 Nevertheless, CR participation rate after IHD has been low and shows disparities between countries10 and individuals on account of various barriers.11 According to a global report based on the responses of experts in CR from countries in 2017, and IHD burdens report from the Institute for Health Metrics and Evaluation, CR was available in only half of all countries, and the number of CR facilities for patients with IHD was insufficient in Korea.1213 The number of incident IHD cases per year per CR facility in Korea was 22, higher than the median value among countries worldwide (n = 21) and the mean of the Organization for Economic Cooperation and Development countries (n = 17).12
In Korea, CR was primarily introduced around the late 1990s. There has been expert- and government-led efforts to promote CR. Regional cardiocerebrovascular centers have been established since 2009, and a total of 14 centers are being operated to improve the quality of cardiovascular treatment, including CR. CR services after IHD have been reimbursed as medical treatment benefits since February 2017. Despite these efforts, the rate of CR participation remains low in the hospitals actively delivering CR (14%–35%).11 Nationwide CR participation rates are expected to be lower, considering the insufficient number of CR facilities12; however, this has not been estimated in Korea. Understanding the current status of nationwide CR use may be an important first step to establish an effective strategy towards the promotion of CR in Korea.
Therefore, this study was designed to measure the nationwide hospital-based CR participation rate, the current numbers of hospitals delivering CR services among patients after acute myocardial infarction (AMI), and the insufficiency in the number of CR facilities in Korea compared to those of other high-income countries. The Korean National Health Insurance Service (NHIS) database from 2017 was used, because only claim codes starting from February 2017 could be identified. Similarly, the risk factors for CR nonparticipation after AMI were identified in hospitals considered as actively delivering CR.
METHODS
Data source
The NHIS, the only insurer operated by the Korean government, covers 97.0% of the Korean population.14 The NHIS database contains eligibility information (income-based insurance contributions, demographic variables, date of death), healthcare utilization information (diagnosis, length of stay, treatment costs, services received), and healthcare provider information (types of institutions, human resources, equipment).15 With permission to access the database, one can collect information about demographics, inpatient and outpatient medical service claim data, and disorders diagnosed per the International Classification of Diseases, 10th revision, Clinical Modification (ICD-10-CM) codes.
Operational definitions of AMI patients and CR participation
Patients were diagnosed with AMI if they were 1) aged between 40 and 80 years, and 2) hospitalized according to the ICD-10-CM based diagnosis of AMI (I21). In a previous study, this definition had a range between 71.4%–73.1% accuracy and fair-to-good reliability.16 The index admission occurred between July 1, 2017 and June 30, 2018 (Fig. 1). This period was selected with consideration for National Health Insurance coverage of CR starting in February 2017.
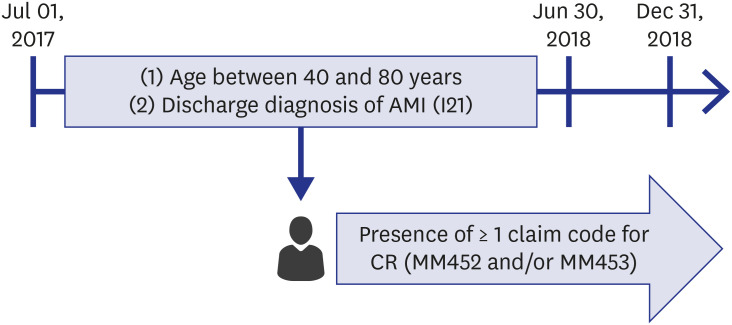
The CR participation was defined as the presence of at least one outpatient-based claim code for ‘MM452 (cardiac rehabilitation evaluation)’ or ‘MM453 (cardiac rehabilitation therapy)’. To avoid irrelevant claims, the claim code had to be presented within 6 months after the diagnosis of AMI until December 31st, 2018 (Fig. 1). During the analysis period, the medical costs of CR were fully insured by the NHIS.
Other variables
Age, sex, and the amount of health insurance premium were identified from the NHIS database. Age was categorized as follows: 40–60, 61–70, and 71–80. Based on the amount of health insurance premium per patient, the income status among all Korean citizens was estimated as quartile. All subjects were classified into urban and rural residents according to their place of registration, which was Si-Gun-Gu (administrative districts in Korea). Urban residents were defined as people living in ‘Si’ or ‘Gu’, whereas rural residents were those who live in ‘Gun’.
The classification variable in the NHIS database was used in the identification of hospital types. The hospitals were classified into three divisions according to the Korean medical law as follows: tertiary hospital, general hospital, and hospital.
For the identification of underlying comorbidities of patients, Charlson comorbidity index (CCI) was obtained by reviewing ICD-10-CM diagnoses.17 In this study, CCI was categorized as 0–4, 5–6, and ≥ 7.
Data analysis and outcomes
Based on the definition, as mentioned earlier, the number of AMI patients and CR participants were estimated. The crude CR participation rate was calculated using the formula below:

CR density, which was first suggested by Turk-Adawi et al.,12 means the number of AMI cases per year per CR facility. Higher numbers represent less sufficient capacity of CR services.

The numbers below the decimal point were rounded off. In addition, the number of CR facilities could be identified from the administrative data. Median annual capacity per facility was adapted from the report from Turk-Adawi et al.12 It was estimated by surveying the average number of annual patients-per-center to CR experts in each country. In Korea, this number was 250. CR participation rate and density was calculated both nationally and by administrative division.
Statistical analysis
Baseline characteristics of the study participants according to CR participation were expressed as the number and percentage, and each variable was categorized. Values were compared using χ2 tests. Logistic regression analyses were conducted to identify the influencing factors of CR only in hospitals with more than 10 CR participants per year, considering the volume threshold for the supply pattern of CR. The SAS software (version 7.1; SAS Institute, Cary, NC, USA) was used, and a 2-sided P value of < 0.05 was considered statistically significant.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Seoul National University Bundang Hospital, Korea (IRB No. X-1901/514-901), the need to obtain informed consent was waived due to the retrospective nature of the study. Data in the Korean NHIS were fully anonymized for analyses.
RESULTS
Baseline characteristics
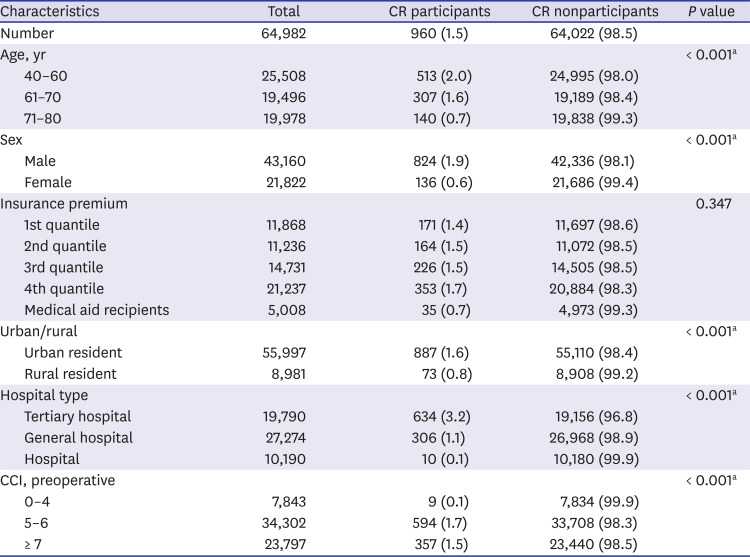
During the index period, 64,982 patients were hospitalized following the clinical diagnosis of AMI in Korea, including 43,160 (66.4%) males and 21,822 (33.6%) females. Table 1 shows the characteristics of the study population according to CR participation. Significant differences were observed between the participants and the nonparticipants following classification by age, sex, residential area, hospital type, and CCI. High ratios of older age, female, rural resident, hospital (non-tertiary, non-general), and low CCI were observed in the nonparticipant group.
Table 1
Baseline characteristics of study participants
CR participation rate and density
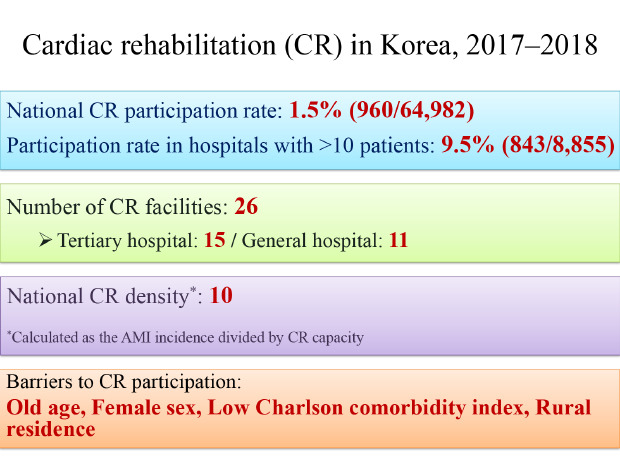
In the 64,982 study subjects, the national CR participation rate was 1.5% (960/64,982). There were 26 CR-providing facilities (15 tertiary hospitals and 11 general hospitals). In the calculation of the CR density, the number of study subjects was treated as annual AMI incidence. According to this parameter, the national CR density was approximately 10 AMI incidence/capacity/year, which means 10 times more CR facilities are needed to accommodate the incidence of AMI.
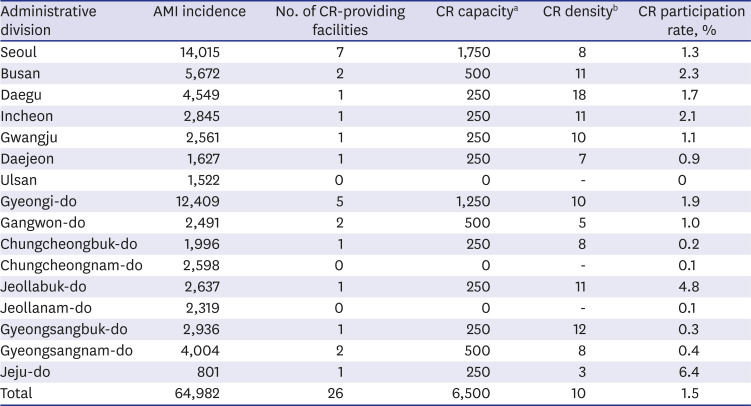
The CR use, according to the administrative divisions, is presented in Table 2. The CR participation rate widely varied across the nation, ranging from 0.0% to 6.4%. Similarly, variation was observed in CR density, with values ranging from 3 to 18.
Table 2
Hospital-based CR utilization by administrative division
Among 8,855 patients who were treated in hospitals with more than 10 participants per year, the participation rate increased to 9.5% (843/8,855).
Factors associated with CR participation
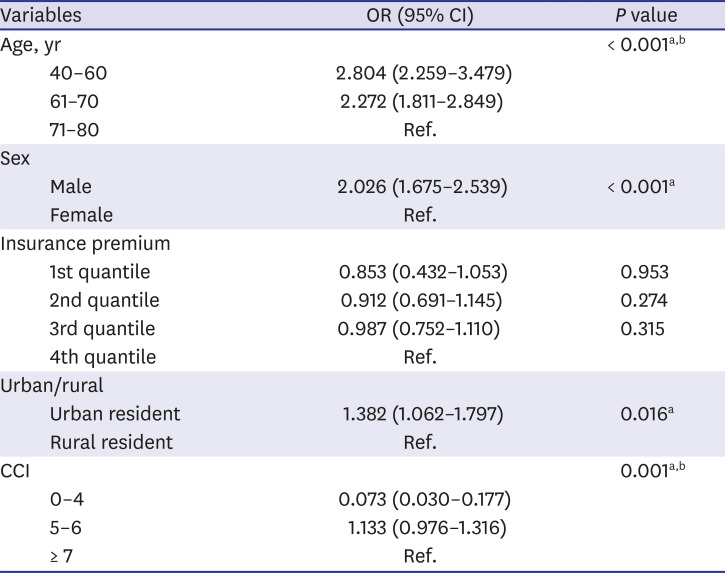
Factors associated with the CR participation are shown in Table 3. The younger age group demonstrated a higher odds ratio of CR participation than did the older age group. Male patients participated more in CR than female patients did. In addition, urban residents seemed to participate more in CR than rural residents. Patients with the lowest CCI ranging from 0–4 participated less in CR than those with CCI ≥ 7. No significant difference was observed in CR participation between the groups classified based on insurance premium quantile.
Table 3
Logistic regression analysis for CR participation
DISCUSSION
Despite the recommendations accentuating the role of CR in AMI patients,456 only 1.5% of these patients participated in the CR program in Korea. There was geographical variance in participation, ranging from 0.0% to 6.4%. The relatively high AMI incidence obtained in this study compared to that of the Statistics Korea18 and a range of 71.4%–73.1% accuracy of the operational definition for diagnosing AMI16 could have resulted in the underestimation of the participation rate. Nevertheless, even considering these limitations, the participation rate of 1.5% was remarkably lower than that of Europe (30%–50%)19 and the United States (10.3%–16.3%).20 According to our calculation, the CR density in Korea was about 10. This means that approximately 234 more CR facilities should be established to cover the annual incidence of AMI.
In hospitals with > 10 CR participants, the CR participation rate was similarly insufficient (9.5%). This suggests that efforts are required to promote CR participation even in actively-operating CR facilities; the identification of CR barriers is important to plan effective promotion strategies. This study showed a markedly lower CR participation in patients with old age, female sex, and rural residence, in line with the results of previous studies.212223 The reasons for inadequate CR participation among these populations are multifactorial.2425 Proposed explanations for low participation in elderly patients include inadequate physician referral, comorbidity-associated mobility issues, and transportation issues.26 Poor CR participation in females might be attributed to insufficient physician referral, more familial responsibilities, and less spare time to attend CR programs.27 Self-reliant rural attitudes and low accessibility to medical facilities might have contributed to poor CR participation among rural residents.28 To overcome these issues, strategies should be implemented, including automated referral systems, improved awareness of CR, flexible therapy hours, and alternative CR delivery models such as home- and community-based CR.2429
In this study, no difference was observed between the participants and the nonparticipants with regard to income status; this is different from previous studies that revealed higher income earning patients attend CR more in Europe30 and the United States.31 One possible explanation for the unobserved difference is the decreased economic burden of CR due to its coverage by the National Health Insurance in Korea. Another possible explanation is that high income earning patients are more likely to be economically active with insufficient time to participate32; this can offset the beneficial effects of high income on CR participation. Therefore, further study is required to clarify the effect of socioeconomic status on CR participation in Korea. Similarly, CCI was not a significant factor in previous studies investigating CR barriers.233334 However, the fewer comorbidities group (the group with the lowest CCI ranging between 0–4) participated least often in this study; this could be due to the less motivation and fewer needs of these patients, which could have resulted in nonparticipation in CR.1135 In addition, CCI is determined by the number of comorbid diseases, and this may not directly reflect the patient's physical or cardiac function, which are important factors for CR participation.36 Therefore, a further study including variables such as cardiorespiratory fitness level or ejection fraction is needed.
In this study, only a limited number of potential barriers were retrospectively investigated. Nevertheless, various CR barriers have been reported in the literature213738 and they may differently affect CR participation depending on the particular clinical situation in each hospital or region. Therefore, efforts to identify CR barriers in each region and planning effective CR promotion strategies according to identified barriers are required.39
There are several limitations to this study. First, the diagnosis of AMI was operationally defined using medical claim records. In a previous study, this method has been known to have an accuracy ranging between 71.4%–73.1% and fair-to-good reliability.16 Nevertheless, there are possibilities of false exclusion or inclusion. Second, national CR density was calculated using the median capacity of Korean hospital-based CR facility participating in a previous global survey.12 Most of the hospitals used in the estimation of the CR capacity were tertiary or general hospitals that probably had larger CR capacity, and the CR density may have been underestimated. In addition, the distance from a CR facility to a patient's home is an important influencing factor for CR participation27 that was not considered. For example, a CR facility with a large capacity could be situated extremely far from the patient's home; therefore, the required number of CR facilities based on CR density in this study could have been equally underestimated. Third, there could be mismatch between procedure, benefits, and claim record. Because the period of index admission in this study was the transition period of the change in benefits type for CR, there is a possibility of incomplete reimbursement for any reason. Therefore, follow-up research until the post-transitional period is important. Fourth, other known factors that affect participation in CR, including physician referral pattern, the ability to drive, and education level, were not evaluated.2123 Further comprehensive studies should be performed to evaluate CR barriers. Fifth, indication for CR was confined to AMI in this study. Current indications for CR are broader, including other cardiovascular diseases such as unstable angina, valvular heart disease, heart failure, and peripheral arterial diseases.564041 Therefore, the possibility of unrevealed demand for CR exists. Further studies, including these group of patients, are needed. Finally, this is the initial report of CR utilization (in the period of CR utilization) in Korea. Three more regional cardiocerebrovascular centers were installed in 2019, and more hospitals may provide CR at this time. Therefore, a follow-up study is required.
In conclusion, hospital-based CR participation rate after AMI was only 1.5% nationally, and the overall supply was insufficient in Korea, despite coverage by the National Health Insurance, compared to CR use in other high-income countries. To overcome these problems, more CR facilities and effective strategies to overcome CR barriers are required. Therefore, a follow-up study with a more comprehensive evaluation of barriers to CR is needed in the future.
 XML Download
XML Download