

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD), defined as lipid infiltration inside the hepatocytes in the absence of severe alcohol consumption or viral hepatitis, is one of the most common liver diseases. The prevalence of NAFLD is estimated to be 20% to 30% in western countries1 and 12% to 33% in Asia.2345 In recent decades, a number of studies have suggested an association between NAFLD and metabolic disease, such as insulin resistance, cardiovascular disease, and obesity in non-pregnant subjects.6789 Based on this evidence, NAFLD is now considered a hepatic manifestation of metabolic syndrome.
The enzyme alanine aminotransferase (ALT) is commonly related to NAFLD in the absence of viral hepatitis or alcohol abuse,7 and NALFD can be firstly detected by elevated liver enzymes in the general population.1011 Considering this relationship between NAFLD and elevated ALT levels, previous studies have reported that elevated ALT is associated with diabetes, high blood pressure, or cardiovascular disease in adults.7121314
Until now, the clinical significance of NAFLD or elevated ALT levels in pregnancy has not been well determined, although a few studies have reported the possibility of increased risk for adverse pregnancy outcomes with NAFLD or elevated ALT levels.15161718 The objective of this study was to determine the association between elevated ALT in early pregnancy and the development of gestational diabetes or preeclampsia in late pregnancy.
METHODS
Study design
A retrospective cohort study was conducted including pregnant women who met the following inclusion criteria: 1) singleton pregnancy; 2) ALT levels were measured in antenatal outpatient clinic at 4–20 weeks of gestation; 3) patients were screened for gestational diabetes and delivered in Cheil General Hospital and Women's Healthcare Center between January 2014 and December 2014. Women with pregestational diabetes, chronic hypertension, and those with known chronic viral hepatitis B, hepatitis C, or other liver diseases were excluded.
Measurement of ALT
Measurement of ALT at the time of initial laboratory tests in early pregnancy is the routine practice in Cheil General Hospital and Women's Healthcare Center. Patients were divided into two groups according to their ALT levels (normal ALT [≤ 95th percentile] and elevated ALT [> 95th percentile]).
Diagnosis of gestational diabetes and preeclampsia
The frequency of gestational diabetes and preeclampsia was compared between the groups. According to the recommendations of the American College of Obstetricians and Gynecologists (ACOG), two-step approach with universal screening was used to screen and diagnose gestational diabetes.19 For the 50 g screening, the plasma glucose level was measured one hour after 50 g glucose loading, and women with glucose levels of 140 mg/dL or higher were defined as screening positive. For women with positive screening results, a 75 g 2-hour oral glucose tolerance test (OGTT) was conducted. In our institution, the World Health Organization (WHO) criteria is usually adopted for the diagnosis of gestational diabetes (95 mg/dL for fasting glucose, 180 mg/dL for 1-hour glucose, 155 mg/dL for 2-hour glucose; two or more of these must be met or exceeded for diagnosis).20 In the analysis of the current study, the frequency of gestational diabetes according to the newly suggested criteria by the International Association of Diabetes and Pregnancy Study Groups (IADPSG) was also evaluated (92 mg/dL for fasting glucose, 180 mg/dL for 1-hour glucose, 153 mg/dL for 2-hour glucose; at least one of these must be met or exceeded for diagnosis).21
For the diagnosis of pregnancy-associated hypertension, the criteria suggested by ACOG were adopted.22 Pregnancy hypertension included gestational hypertension, preeclampsia, and eclampsia. The frequency of preeclampsia (including preeclampsia and eclampsia) was also evaluated.
Statistical methods
Proportions were compared using Fisher's exact test and comparisons of continuous variables between groups were performed with the Mann-Whitney U test. Logistic regression was conducted for multivariate analysis. The association between elevated levels and the risk of preeclampsia was assessed by logistic regression with the Firth personalized likelihood to avoid bias due to small number of cases with preeclampsia. Statistical analysis was performed by SPSS software (version 22.0; IBM Corp., Chicago, IL, USA) and R (version 3.6.2; R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org). P value < 0.05 was considered as significant.
RESULTS
During the study period, there were a total of 5,223 singleton deliveries. Among these, 3,007 women visited our institution in early pregnancy and received initial laboratory tests, including ALT. After excluding cases with pregestational diabetes (n = 53), chronic hypertension (n = 25), chronic hepatitis B or C (n = 78), those in which screening and diagnostic testing for gestational diabetes were performed in other institutions (n = 516), and those in which patient rejected 75 g OGTT after a positive result in 50 g OGTT (n = 10), 2,325 women were included in the analysis (Fig. 1).
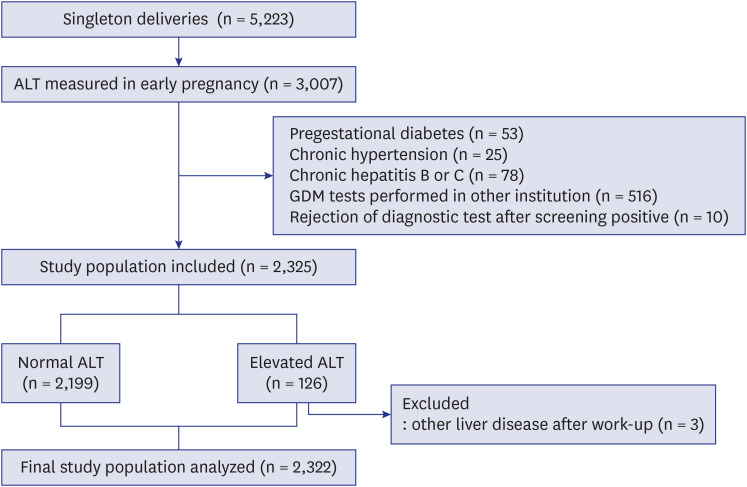
Women with ALT levels > 30 IU/L were designated as the elevated ALT group (> 95th percentile values). According to this cut-off value, 2,199 women had normal ALT levels, and 126 women had elevated ALT levels. After excluding 3 women who were diagnosed with other liver diseases after work-up for elevated ALT levels, a total of 2,322 women were included in the final analysis.
Table 1 shows the clinical characteristics and laboratory results according to the ALT levels. Cases with elevated AST levels had higher median pre-pregnancy body mass index (BMI) and a higher proportion of nulliparity. In addition, cases with elevated ALT levels had higher median concentrations of AST, cholesterol, and alkaline phosphatase.
Table 1
Characteristics and laboratory results according to the early ALT levels
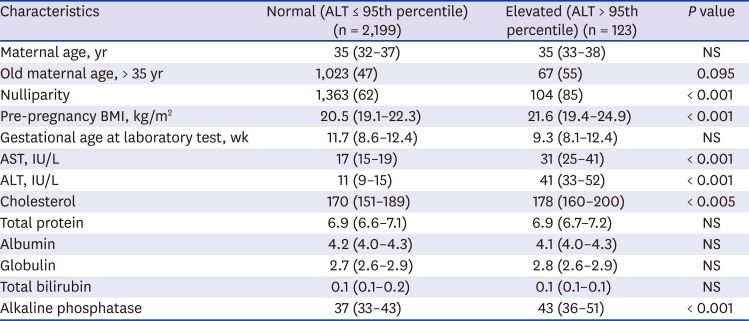
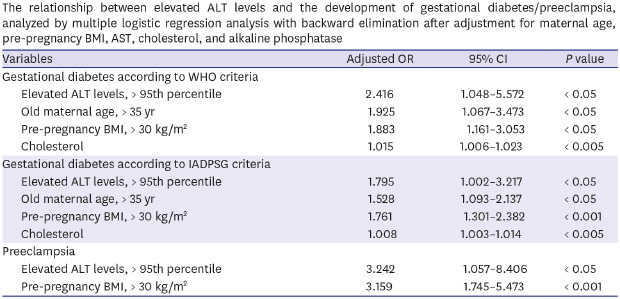
Table 2 compares the pregnancy outcomes between the two groups of cases. Cases with elevated ALT levels had a higher risk for the subsequent development of gestational diabetes mellitus (GDM) by both WHO and IADPSG criteria. In addition, cases with elevated ALT levels also had higher risks for both pregnancy hypertension and preeclampsia. Supplementary Tables 1 and 2 shows that the frequency of women with elevated ALT level were also higher in cases with gestational diabetes or preeclampsia. This relationship between elevated ALT levels and the development of GDM and preeclampsia remained significant after adjustment of confounding variables (Table 3).
Table 2
Pregnancy outcomes according to the early ALT levels
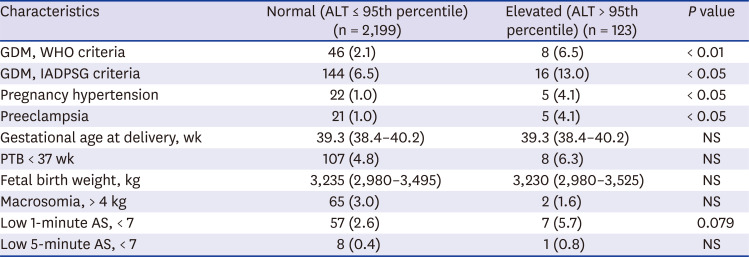
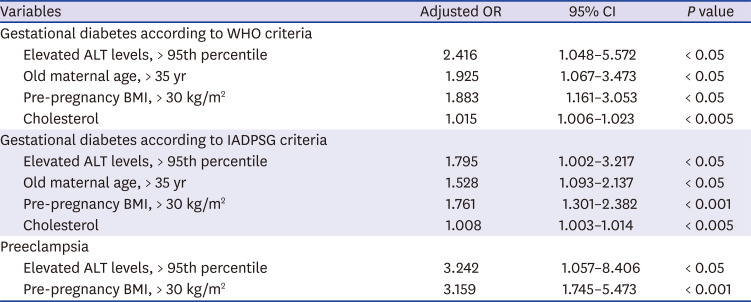
Table 3
The relationship between elevated ALT levels and the development of gestational diabetes/preeclampsia, analyzed by multiple logistic regression analysis with backward elimination after adjustment for maternal age, pre-pregnancy BMI, AST, cholesterol, and alkaline phosphatase
Among the study population, 2,312 women had the result for ALT levels during late pregnancy (measured after 20 weeks of gestation, median gestational age at measurement 36.7 weeks). Women with elevated ALT levels during late pregnancy also had increased risk for the development of GDM and preeclampsia (Supplementary Table 3). This increased risk of GDM and preeclampsia in women with elevated ALT levels during late pregnancy remained significant after adjustment of confounding variables.
DISCUSSION
The principal findings of this study were: 1) cases with elevated early ALT levels (> 95th percentile) had a higher risk of subsequent gestational diabetes or preeclampsia; 2) this relationship between elevated ALT and an increased risk of gestational diabetes/preeclampsia remained significant after adjustment.
In spite of firm evidence on the association between NAFLD and metabolic syndrome, the clinical significance of NAFLD or elevated ALT levels in pregnancy is not well determined. Recently, a large Swedish national cohort reported that women with a diagnosis of NALFD are at high risk for adverse pregnancy outcomes, such as gestational diabetes, preeclampsia, preterm birth, and cesarean delivery.15 In this study 110 women were identified with a pre-pregnancy International Classification of Diseases, 9th Revision diagnosis of NAFLD among 1,960,416 births, although the prevalence of NAFLD is known to be about 20%–30% in western countries.1 The fact that this population was not routinely screened for NAFLD has been attributed to the lower detection of NAFLD in this study. Recently, in another nested case-control study, 83 women with gestational diabetes had elevated ALT levels when compared to 247 controls in early gestation.16 This study also reported that elevated ALT levels in early pregnancy increased the risk of large for gestational age birth weight even in the absence of clinical glucose tolerance.23 In a more recent study, De Souza et al.24 followed up the cohort of NAFLD diagnosed by ultrasound, and have shown that they are at risk of a composite outcome of mid-pregnancy dysglycemia, which was defined as impaired fasting glucose, impaired glucose tolerance, or gestational diabetes in 75 g OGTT.
The result of the current study on the association between elevated ALT levels and gestational diabetes/preeclampsia is consistent with these previous studies. The strengths of the current study, when compared to prior studies, are: 1) in this consecutive retrospective cohort study, we have evaluated ALT levels in all the women who visited our clinic in early pregnancy; 2) we have evaluated other metabolic markers, such as cholesterol and alkaline phosphatase, and have shown that elevated ALT is associated with the risk of gestational diabetes/preeclampsia even after adjustment of these markers; 3) we have also shown that elevated ALT levels are associated with the risk of preeclampsia development. To the best of our knowledge, this is the first study which has shown the association between elevated ALT levels and the subsequent risk of preeclampsia.
In addition to firm evidence on the association between NAFLD and diabetes, several reports have documented NAFLD as a risk factor for hypertension and cardiovascular disease in non-pregnant adults.252627 The current study's finding that elevated ALT in early pregnancy is associated with the risk of preeclampsia in late pregnancy will enhance our understanding on the pathophysiology underlying NAFLD and hypertension.
Then why are the elevated ALT levels in early pregnancy associated with subsequent risk of gestational diabetes/preeclampsia? There are accumulating evidences that NAFLD is a hepatic manifestation of metabolic syndrome,6789 which can result in the hypertension or insulin resistance. Considering that pregnancy itself is a window period of future metabolic risk,28 the association between NAFLD and metabolic disease can be clearly depicted during gestational period. The underlying mechanism between NAFLD and diabetes/hypertension is not clear, but several mechanisms have been suggested. First, the NAFLD and diabetes/hypertension may share common underlying metabolic dysfunction such as obesity.1524 However, the relationship between elevated AST levels and the risk of gestational diabetes/preeclampsia remained significant even after adjustment for pre-pregnancy BMI in the current study. This suggest that other mechanisms may be likely to be involved. Second, proinflammatory cytokines from adipose tissues may be transferred to the liver resulting in fat accumulation (NAFLD), and make adipose tissues more metabolically adverse, resulting in gestational diabetes and hypertension. Third, the fat accumulation can also happen in the maternal spiral artery suppling the placenta, leading to atherosclerosis and impaired vascular remodeling, which is a hallmark of preeclampsia.29
There are several points to be considered. First, we used elevated ALT levels as a crude marker of NAFLD, although the confirmative diagnosis of NAFLD is made by liver biopsy, which is hard to perform in pregnant women. Other diagnostic modalities, such as liver ultrasound or transient elastography may be needed to confirm the association between NAFLD and adverse pregnancy outcomes. And the cut-off value for elevated ALT was lower than that in non-pregnant adult (> 30 IU/L). It is well known that serum ALT levels are slightly lower compared with non-pregnant values.30 In addition, the AST was not elevated in cases with gestational diabetes in the current study population. Although AST was elevated in cases with preeclampsia, this relationship between elevated AST and preeclampsia did not remain significant after adjustment (Table 3). However, other liver enzymes such as γ-glutamyltransferase (γ-GT), which was not evaluated in the current study, should be evaluated in the context of NAFLD and gestational diabetes/preeclampsia. The γ-GT is a well-known biomarker for liver fat accumulation, and γ-GT also predicted well the risk of diabetes in non-pregnant population.31 Second, we could not evaluate alcohol consumption during pregnancy, but women with heavy alcohol consumption during pregnancy were reported to be nearly absent in Korea.32 Next, in our institution, we adopted a two-step approach for gestational diabetes (50 g OGTT with 140 mg/dL as a cut-off value, and 75 g OGTT with the WHO criteria for the diagnosis of gestational diabetes).20 There are controversies regarding the screening and diagnostic strategies in the diagnosis of gestational diabetes.192133 In the current study, we also analyzed the frequency of gestational diabetes according to the IADPSG criteria,21 and have shown that gestational diabetes also increased in women with elevated ALT levels according to this criteria. Third, the incidence of pregnancy hypertension in the current study is 1.2%. This incidence is relatively lower than those reported in previous studies. However, Korean pregnant women have been reported to have relatively low prevalence of preeclampsia in the literature.34 This lower prevalence of preeclampsia may be attributed to lower BMI, lifestyle factors or different ethnicity.3536373839 Further studies in other races/ethnicities are needed to confirm the finding of the current study. Lastly, other pregnancy complications also need to be evaluated in pregnant women with elevated ALT or NAFLD. In the current study, the risk of preterm birth or small for gestational age was not increased with cases with elevated ALT.
In conclusion, unexplained elevated ALT in early pregnancy was associated with the risk of subsequent development of gestational diabetes and preeclampsia in late pregnancy.
 XML Download
XML Download