

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Gout is an inflammatory arthritis that occurs worldwide. The prevalence and hospitalization rates of gout are increasing,123 and gout carries a large national economic burden.4 Understanding the risk factors and pathogenesis of gout may help manage gouty arthritis appropriately and reduce its socioeconomic burden. Gout shows a seasonal variation that widely differs among geographic areas, and we previously reported a seasonal effect on gout in Korea.5 We previously suggested that these gout attacks were provoked by increased physical activity and dehydration in summer. However, we had no information regarding changes in diet and had only limited laboratory data because this was a retrospective study in patients receiving a urate-lowering therapy (ULT). Consequently, the relationship between gout attacks and provoking factors such as diet-meat/seafood/alcohol, etc., serum uric acid/lipid levels, or weather conditions, all of which had been reported as possible gout triggers,6 was difficult to determine. Therefore we designed this prospective study to elucidate the seasonality and associated factors of gout attacks in Korea.
METHODS
We prospectively enrolled patients with gout attacks who were treated at nine rheumatology clinics between January 2015 and July 2018 and followed them for 1-year. The study subjects consisted of patients who received treatment for gout attacks at rheumatology clinics, including initial attacks or flares during management or loss to follow-up. The diagnosis of gout attacks was made on the basis of findings of monosodium urate crystals on polarization microscopy or dual-energy computed tomography, or clinical classification criteria.7 Patients were excluded if they refused to be enrolled in this study.
Demographic data, clinical and laboratory features, seasonality and meteorological data were collected at baseline, consecutive flares, and 6-month and 1-year follow-up visits. All the patients provided information, including gout onset date, life habitual status-presence of smoking/alcohol/exercise, pain visual analogue scale (VAS) score, provoking factors of gout attacks, family history of gout, and demographic data such as age, height, and weight, by answering a questionnaire. A physical examination was performed by a rheumatologist at each visit. Blood sampling and analysis were performed at each institute according to routine practice. Laboratory data included complete blood count, biochemical analyses for uric acid level, fasting glucose level, liver function, lipid profiles, and serum cortisol at each time point and at the time of flares during follow-up if any.
Seasons were classified by 3-month time intervals (i.e., the period from March 1 through May 31 was defined as spring). Internet-based open source meteorological data were obtained from the Korea Meteorological Administration.
Statistical analysis
The season and month of gout attacks were tested using a goodness-of-fit test and point estimation with 95% confidence interval. The χ2, Mann-Whitney, and Kruskal-Wallis tests after testing normality (using Kolmogorov-Smirnov) were used. SPSS version 19 (SPSS, Inc., an IBM company, Chicago, IL, USA) was used for all statistical analyses. The null hypotheses of no difference were rejected if the P values were < 0.05.
Ethics statement
The Institutional Review Board (IRB) of each hospital approved this study (GCIRB 2015-16 Gachon University Gil Hospital; KNUH-2014-12-008-001 Kangwon National University School of Medicine; 2014-12-024 Gyeongsang National University School of Medicine; KMC IRB 1507-04 Kyung Hee University Hospital; AJIRB-MED-SUR-14-409 Ajou University School of Medicine; B1412/280-301 Seoul National University Bundang Hospital; 2014-12-021-003 Ewha Womans University College of Medicine; 1501-003-025 Pusan National University School of Medicine; C2014253 [1450] Chung-Ang University School of Medicine). Consent was obtained from the patients at the time of enrollment.
RESULTS
Two hundred-five patients (men, n = 193, 94.1%) were enrolled. The median age, body mass index, gout attack duration, serum uric acid level and VAS score for pain at enrollment were 50.0 years, 25.4, 5.0 days, 7.4 mg/dL, and 7.0 (range, 0–10), respectively (Tables 1 and 2). Hypertension was the most common comorbidity (41.0%). Tophus was found in 9.8% of the patients. One hundred thirty patients (63.4%) were alcohol drinkers, and 101 patients (49.3%) were current or past smokers. The proportions of patients with initial gout attack, flares during treatment, and flares during follow-up loss were 46.8% (n = 96), 44.9% (n = 92), and 8.3% (n = 17), respectively (Table 2). The median serum uric acid level was higher in the group with initial gout attack or flares without treatment than in the group with flares during treatment as expected (8.0 vs. 8.0 vs. 6.5 mg/dL). According to season, triglyceride level was significantly lower in the winter season at enrollment (137 mg/dL, interquartile range [IQR], 92.0; P = 0.030 by Kruskal-Wallis test), and serum cortisol level was lower in the spring season (7.8 μg/dL; IQR, 3.7; P = 0.011, data not shown).
Table 1
Demographic and clinical characteristics of patients at baseline
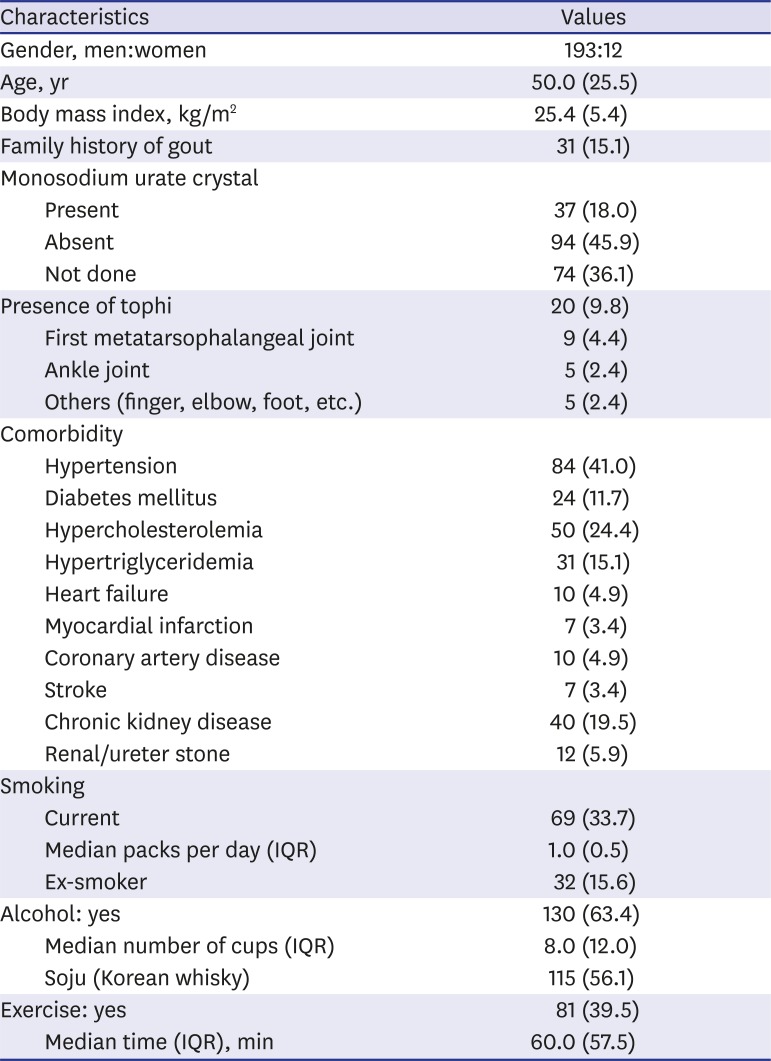
Table 2
Clinical features according to gout attack group at baseline
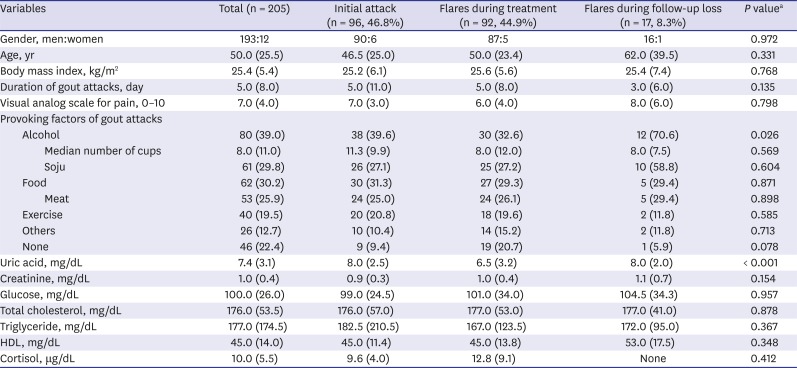
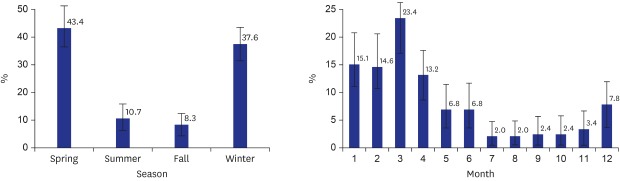
Gout attacks were most common in the spring season (43.4%, P < 0.001) and in March (23.4%, P < 0.001) (Fig. 1A and B). A similar pattern of seasonality was demonstrated in the initial gout attack group (Fig. 2A and B) and in the group of patients who completed 1-year follow-up (n = 125, data not shown). Alcohol was the most common provoking factor (39.0%) in the total cases, especially in the group with flares during loss to follow-up (70.6%, P = 0.026), followed by food such as meat (25.9%), and exercise (19.5%). The patients who reported no provoking factors accounted for 22.4% of the total cases (Table 2). Alcohol was the first provoking factor in all the seasons; however, the proportion of patients who reported alcohol as a provoking factor was highest in the summer (50%) (Table 3). Monoarthritis (79.5%) and first metatarsophalangeal joint (52.7%) were the most common pattern and site of joint involvement, respectively (Fig. 1C and D).
Fig. 1
Characteristics of the gout attacks in the total cases (n = 205). (A) Distribution of the gout attacks (point estimation, 95% confidence interval) according to season and (B) month, (C) pattern of arthritis, and (D) distribution of joint involvement. Season is classified by 3-month intervals. The P values for (A) and (B) are < 0.001 in the goodness-of-fit test.
MTP = metatarsophalangeal, PIP = proximal interphalangeal, MCP = metacarpophalangeal.
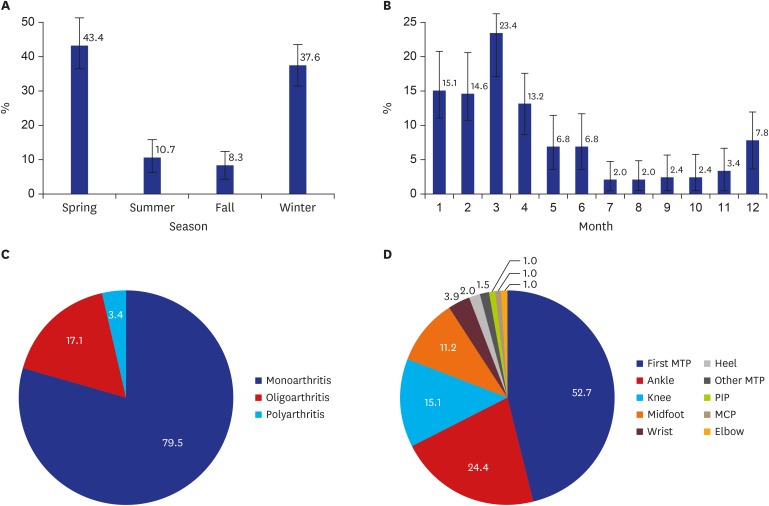
Fig. 2
Characteristics of the gout attacks in the initial gout attack group (n = 96). (A) Distribution of the gout attacks (point estimation, 95% confidence interval) according to season and (B) month, (C) prescription pattern, and (D) class of medications. Season is classified by 3-month intervals. The P values for (A) and (B) are < 0.001 in the goodness-of-fit test.
NSAIDs = nonsteroidal anti-inflammatory drugs.
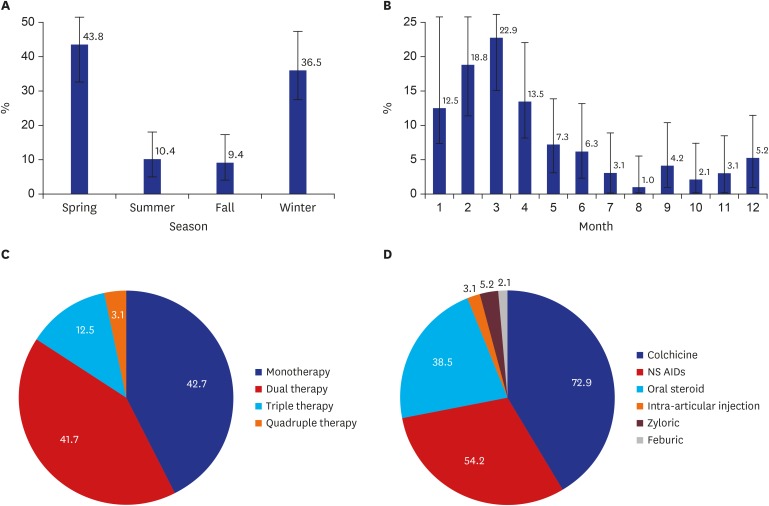
Table 3
Provoking factors according to season at baseline

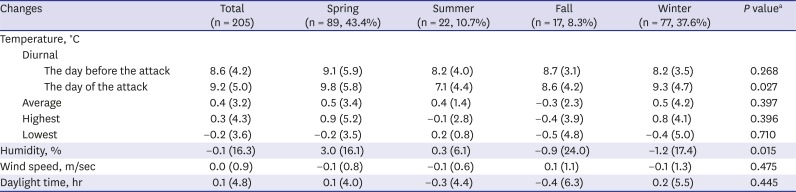
The median diurnal change in temperature on the day of gout attack was highest in spring (9.8°C) (Table 4). The median change in humidity between the 2 consecutive days (the day before and the day of the attack) was significantly different among the seasons (3.0%, spring; 0.3%, summer; −0.9%, fall; −1.2%, winter; P = 0.015). For the subgroup analysis, the same significant differences in meteorological factors were shown in the patients who completed 1-year follow-up (n = 125, data not shown).
Table 4
Meteorological factors associated with gout attacks
The patterns of prescription for the patients with initial gouty attack in Korea were variable, such as monotherapy (42.7%), and dual (41.7%), triple (12.5%), and quadruple therapies (3.1%) (Fig. 2C). The most commonly used medication for initial management was colchicine (72.9%, n = 70/96), followed by nonsteroidal anti-inflammatory drugs (NSAIDs; 54.2%, n = 52), oral steroid (38.5%, n = 37), urate lowering agents (ULT; 7.3%, n = 7), and intra-articular glucocorticoid injection (3.1%, n = 3) (Fig. 2D). Colchicine (35.9%, n = 33/92) was also the most common prophylactic medication in Korea, which was taken at enrollment in the group with flares during treatment, followed by oral glucocorticoid (8.7%, n = 8). Fifty-nine patients (64.1%, n = 59/92) in this group were treated with ULT (allopurinol, 21.7%; febuxostat, 40.2%; and benzbromarone, 2.2%). Oral glucocorticoid was the most common additional medication for flares (34.8%), followed by NSAIDs (29.3%), colchicine (22.8%), and intra-articular glucocorticoid injection (8.7%; data not shown).
The median total uric acid level at enrollment (7.4 mg/dL) decreased to 6.3 mg/dL at 6 months, and to 5.9 mg/dL at 12 months. Unlike the total cholesterol level at 6 months (lowest in the winter season, 164.0 mg/dL; IQR, 52.5; P = 0.010; data not shown), uric acid, creatinine, glucose, triglyceride, high-density lipoprotein, and cortisol levels showed no significant seasonal differences at 6 and 12 months. During the follow-up period, 64 gout episodes occurred in 51 patients and 21 flares occurred in 18 patients in the initial attack group. The median duration to the second episode after the first attack was 8.6 months (IQR, 8.9) in the initial attack group. Three patients had a third attack, and 5 had a fourth attack. One hundred twenty-five patients (61%) completed 1-year follow-up (51%, initial attack group; 71.7%, group with flares during treatment; and 58.8%, group with flares during loss to follow-up). Forty-five flares occurred during follow-up in 35 patients who completed 1-year follow-up.
DISCUSSION
To our knowledge, this is the first prospective study on gout seasonality. We found that spring and March were the most common season and month of gout attacks in Korea. Spring season was the dominant season of gout attack in many previous studies.8910 In Italy,11 the highest incidence was in spring (March to May) for both gout and pseudogout. In a UK study,12 by contrast, the incidence of gout increased from late April to mid-September (the summer period). Our previous retrospective study also showed that summer was the most common season in the patients who received a ULT for > 1 year after discontinuing prophylactic medications.5 However, in this study, we included patients with initial attacks, gout flares during management, or flares during loss to follow-up. A similar seasonal pattern was observed in the initial gout attack group, which suggests that in Korea, spring is the most common season especially in patients with initial onset.
Gout attack was associated with some meteorological factors in this study. The median diurnal change in temperature on the day of gout attack and the median change in humidity between 2 consecutive days were highest in spring. These findings suggest that diurnal change in temperatures and change in humidity are associated with gout seasonality in this study and are provoking factors of gout attacks. Park et al.13 reported that gout attacks occurred more frequently during the period in which the temperature significantly increased between neighboring days. They also reported that this period was spring by season and between March and July by month in the northern hemisphere, using a meta-analysis. According to a study from the United States, the risk of nocturnal gout attacks was 2.36 times higher than that of daytime gout attacks.14 They suggested that the lower body temperature at night and early morning is one of the potential biological mechanisms. Neogi et al.15 reported that high temperature and low humidity over the prior 48 hours were associated higher risk of gout attacks than moderate temperatures. They also reported that high ambient temperature and, possibly, extremes of humidity were associated with an increased risk of gout attack. Recently, the climate pattern has changed in Korea, getting hotter in the summer, and getting colder in the winter. However, the change in the meteorological factors during those seasons are minimal as compared with those in the spring. Dehydration and hot or cold temperatures could be associated with gout attacks, but our study shows that the changes in weather conditions such as temperature or humidity are factors related to gout attack.
The lifestyle-related risk factors of gout attack were also identified in this study. We found that alcohol was the most common cause of gout attacks in all seasons. Although no statistically significant difference was found, the highest proportion of alcohol consumption was observed in the patients with gout attacks in the summer, similar to our previous study.5 Purine-rich food intake such as meat or seafood increased serum uric acid level and provoked gout attacks.16 Food (30.2%) was the second cause of gout attack in our study. Among them, 53 patients reported (85.4%, n = 53/62) meat as a provoking factor. Seafood intake was 6.5% (n = 4).
In the comorbidity survey, the patients had combined hypertension (41%), chronic kidney disease (19.5%), and hypertriglyceridemia (15.1%). Low high-density lipoprotein level was an independent indicator of acute gout attack,17 and therapy for hypertriglyceridemia reduced the serum uric acid levels in gout patients.18 The serum cortisol levels in healthy men were higher in the winter,19 and low cortisol levels during spring might facilitate acute gouty arthritis.6 Serum cortisol level, which was lowest in the spring season, could be associated with the gout attacks in our cohort.
Only 61% of the patients completed 1-year follow-up, and the ratio was lowest (51%) in the initial attack group as expected. The median uric acid level during follow-up did not reach the ideal target level (< 5 mg/dL) in the total cases or in each gout attack groups. These findings indicate that physicians must provide more intensive care to achieve the target uric acid level,202122 and that patients need more education and an adherence program.2324
The strength of this study was the fact that it is the first prospective multicenter study for gouty attack. We identified risk factors precisely and clinical features at the time of gouty attack. Detailed aggravating factors elucidate the association factors of gout attack in Korea. Otherwise, this study has some limitations. First, this study was conducted exclusively in Koreans. However, this study was conducted in 9 representative rheumatology clinics geographically well distributed throughout Korea. Second, because our cohort was enrolled from tertiary hospitals, selection bias was possible, such as the dominance of severe or advanced gout cases.
In conclusion, the most common season and month of gout attack were spring and March, respectively, in this prospective study in Korea. Alcohol consumption was the most common provoking factor, especially in the summer. Diurnal changes in temperatures on the day of the attack and humidity changes between the day before and the day of the attack were associated with the gout attacks in our cohort. In addition to abstaining from alcohol consumption or heavy meat intake, physicians' recommendation for avoidance of extreme change of temperature or humidity in daily life could be helpful to decrease risk of gout attack.
 XML Download
XML Download