

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Out-of-hospital cardiac arrest (OHCA) is a worldwide public health problem. More than 350,000 OHCAs occur annually in the United States.1 In Korea, more than 30,000 OHCAs occur annually with about 5% survival rate.23 Extensive scientific evidence in resuscitation has been presented in the last few decades, and guidelines for the various elements of resuscitation have been updated. However, there are no guidelines for a reasonable duration of resuscitation effort when considering prolongation or termination of resuscitation. This limitation can lead to variation in the duration of resuscitation among emergency medical services (EMS) systems. This can also affect the post-resuscitation process. Usually, OHCA patients who achieve a return of spontaneous circulation (ROSC) with prolonged cardiac arrest time have been recognized to have a poor prognosis. This might lead to reluctance in the provision of post-resuscitation care, such as targeted temperature management (TTM), extracorporeal membrane oxygenation (ECMO), and percutaneous coronary intervention (PCI).4
TTM, recommended as a standard treatment, ameliorates hypoxic brain damage after OHCA. The introduction of TTM has changed the predictive value of the neurologic prognostic markers of OHCA patients known before the implementation of TTM. Moreover, TTM may be beneficial for the neurologic prognosis of OHCA patients with prolonged cardiac arrest. However, there are few studies on the relationship between the neurological outcome and cardiac arrest time in OHCA patients treated with TTM.4567 Furthermore, there is a recent report that 59% of the protocols that determine the application of TTM use the time limit criteria of total ischemic time.8 Meanwhile, there are several studies that showed a good neurological outcome in more than 20% of OHCA patients treated with TTM, despite prolonged cardiac arrest time > 30 minutes.4567 Therefore, selecting patients based on the cardiac arrest time may exclude OHCA patients who may benefit from TTM. Because most EMS systems terminate resuscitation after CPR for about 30 minutes, patients with prolonged cardiac arrest time exceeding 30 minutes may be relatively rare.9 Previous studies included unwitnessed subjects that could not accurately identify the cardiac arrest time.467 With this background, additional large-scale studies are needed.
We hypothesized that favorable neurological outcome can occur even after longer cardiac arrest time in witnessed OHCA patients treated with TTM. Therefore, we evaluated the impact of cardiac arrest time on the neurologic outcome in witnessed OHCA patients treated with TTM using a nationwide OHCA registry.
METHODS
Data resources and study setting
This was a cross-sectional study based on data from a hospital-based nationwide registry of OHCAs in Korea. Data were collected from a registry of Out-of-Hospital Cardiac Arrest Surveillance, 2012 by the Korea Centers for Disease Control and Prevention (KCDC), and data on prehospital information, hospital care, and outcomes were extracted by medical record reviewers of the KCDC.10 The KCDC reviewed the medical records of all OHCA patients transported to hospitals by EMS personnel, and clinical information was extracted using structured forms based on the Utstein Style and Resuscitation Outcome Consortium Project.111213
In Korea, the EMS system is exclusively operated by the national fire department.101112 All EMS-assessed patients are transported to a hospital. EMS providers must start resuscitation efforts immediately for all OHCA patients except as instructed by a medical director to hold CPR when the victim is obviously moribund. EMS providers must continue resuscitation efforts until ROSC is achieved at the field or until arrival at the hospital, and they cannot terminate resuscitation efforts. Only a physician can make the decision of termination. All emergency departments, under attending physicians, generally perform advanced cardiac life support, acute cardiac care, and post-resuscitation care in accordance with the international standard guidelines.
Study population
Data of all EMS-assessed OHCA patients between January 2012 and December 2016 were analyzed. The inclusion criteria were all witnessed OHCA patients who were 15 years of age or older and treated with TTM. The exclusion criteria were as follows: did not achieve ROSC; proclaimed dead in the emergency department; unwitnessed cardiac arrest; unknown time interval; missing information regarding the neurological status at hospital discharge.
Data collection and endpoint
As in previous studies, we defined the downtime as the estimated time from the first recognition of a sign of cardiac arrest such as apnea or unresponsiveness to sustained ROSC.459 Sustained ROSC was defined as the restoration of a palpable pulse for at least 20 minutes.4 These time intervals were collected from a review of estimated times of collapse and times of ROSC from hospital medical records. When the time of collapse was available, but the prehospital ROSC time was not recorded in the registry, downtime was estimated by subtracting the median transport time of Korea EMS from prehospital time, which is the time elapsed from collapse to hospital arrival.111213 The downtime duration was divided into seven categories (0–10, 11–20, 21–30, 31–40, 41–50, 51–60, and > 60 minutes) according to 10-minute intervals. We collected additional information on gender, age, health insurance status, place of cardiac arrest, bystander CPR, prehospital defibrillation, PCI, ECMO, and neurologic outcome at discharge from the hospital. The age of patients was divided into three categories (< 50, 51–70, and > 70 years old). The initial cardiac arrest rhythms were reclassified as shockable (VF/pulseless VT) and non-shockable (PEA and asystole) rhythms. Causes of arrest were classified as cardiac or non-cardiac and defined as a presumed cardiac cause unless an obvious non-cardiac cause was elicited. The place of arrest was reclassified as public and non-public. Health insurance status was categorized into national health insurance and no insurance or medical aid. Neurologic outcome was assessed at time of discharge from the hospital using the Cerebral Performance Category (CPC), as determined by medical record reviewers of the KCDC. The CPC scale is a 5-point scale (1, good cerebral performance; 2, moderate disability; 3, severe disability; 4, vegetative state; and 5, death).14 Neurologic outcomes were dichotomized as either favorable (CPC 1 or 2) or unfavorable (CPC 3 through 5). The primary outcome of this study was a favorable neurological outcome at time of discharge from the hospital.
Statistical analysis
The data are presented as mean ± standard deviation or median with interquartile (IQR) range for continuous variables and as frequencies and percentages for categorical variables. Demographic and clinical characteristics across the categories of downtime duration were analyzed using one-way ANOVA or Kruskal–Wallis, χ2, or Fisher's exact test, as appropriate. We compared the demographic and clinical characteristics between groups with favorable and unfavorable neurologic outcomes using the t-test, the Mann-Whitney U test, the χ2 test, or Fisher's exact test, as appropriate. In the prolonged cardiac arrest group, a multiple logistic regression analysis was conducted to determine independent factors for favorable neurological outcomes and calculate the adjusted odds ratios (ORs) and 95% confidence intervals (CIs). After univariate analyses of the association between each covariate and neurologic outcome, covariates with P values of < 0.05 were included in the multiple logistic regression analysis. We plotted line graphs for the favorable neurologic outcome rates over downtime according to stratified CPR variables using Microsoft Excel 2016. The comparisons of stratified CPR variables in each category of downtime duration were analyzed using the χ2 test, Fisher's exact test, or linear-by-linear association test, as appropriate. A two-sided P value < 0.05 was considered statistically significant. All statistical analyses were performed using the IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Between 2012 and 2016, there were 142,905 EMS-assessed OHCAs in a registry of Out-of-Hospital Cardiac Arrest Surveillance, the following patients were excluded: 196 patients younger than 15 years of age at the time of cardiac arrest, 38,775 patients who did not achieve ROSC, 86,458 patients who were proclaimed dead in the emergency department, 5,958 patients with unwitnessed cardiac arrest, 280 patients with an unknown time interval, 24 patients with unknown CPC at discharge, and 9,251 patients who were not treated with TTM. There were 1,963 patients eligible for the final analysis (Fig. 1). The median age was 58 years (IQR, 47–70) and 74.1% were men. Favorable neurologic outcome rates were 30.5%. The median downtime was 33 minutes (IQR, 23–49).
Fig. 1
Study flowchart.
OHCA = out-of-hospital cardiac arrest, ROSC = return of spontaneous circulation, ED = emergency department, TTM = targeted temperature management, CPC = cerebral performance category.
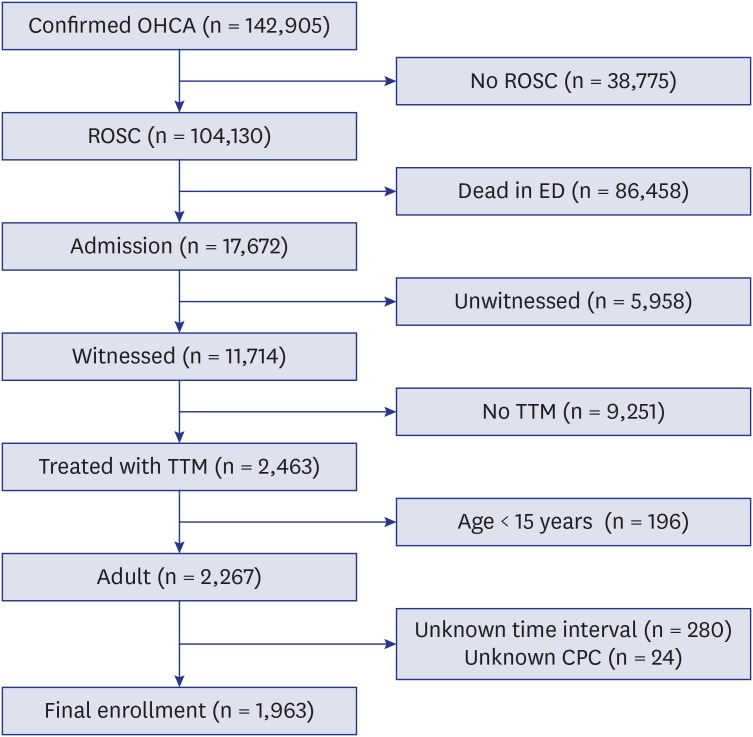
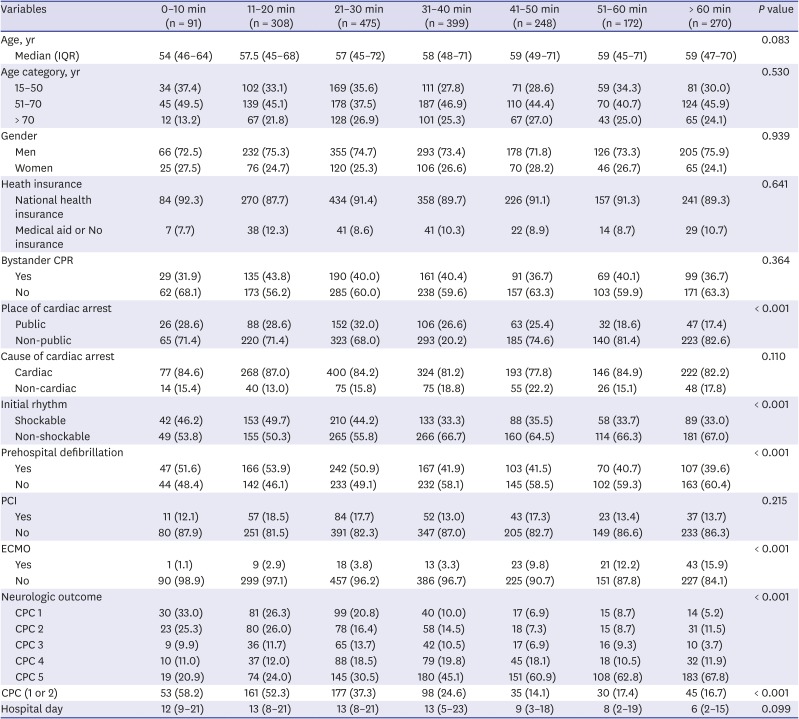
Table 1 represents demographic and clinical features stratified by intervals of downtime. Although there were few notable differences among the intervals, the proportion of patients with initial shockable rhythm and prehospital defibrillation decreased and those treated with ECMO slightly increased with an increase in downtime. In the seven downtime categories of 0–10, 11–20, 21–30, 31–40, 41–50, 51–60, and > 60 minutes, neurologically favorable outcome rates were 58.2%, 52.3%, 37.3%, 24.6%, 14.1%, 17.4%, and 16.7%, respectively (P < 0.001). Rates of favorable neurologic outcome were highest within 10 minutes and gradually decreased up to 40 minutes. However, the rates of the favorable outcome at downtime intervals after 40 minutes were comparable, and 19.1% (208/1,089) of OHCA patients with downtime > 30 minutes and 15.9% (110/690) of patients with downtime > 40 minutes had a favorable neurologic outcome.
Table 1
Demographic and baseline characteristics of the patients stratified by duration of downtime
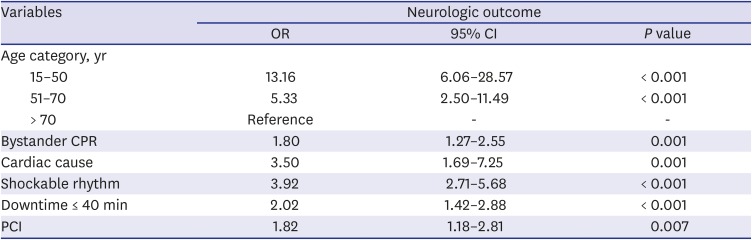
Comparison of demographic characteristic according to neurologic outcome in patients with downtime > 30 minutes are summarized in Table 2. Age, gender, bystander CPR, public location, cardiac cause, initial shockable rhythm, prehospital defibrillation, downtime ≤ 40 minutes, and PCI were significantly different between the two groups. The multiple logistic regression analysis revealed that age 51–70 years (OR, 5.35; 95% CI, 2.50–11.49), age ≤ 50 years (OR, 13.16; 95% CI, 6.06–28.57), shockable rhythm (OR, 3.92; 95% CI, 2.71–5.68), bystander resuscitation (OR, 1.80; 95% CI, 1.27–2.55), cardiac cause (OR, 3.50; 95% CI, 1.69–7.25), percutaneous coronary intervention (OR, 1.82; 95% CI, 1.18–2.81), and downtime ≤ 40 minutes (OR, 2.02; 95% CI, 1.42–2.88) were found to be independent prognostic factors for favorable neurologic outcomes (Table 3).
Table 2
Comparison of clinical features according to neurologic outcome in patients with downtime > 30 minutes
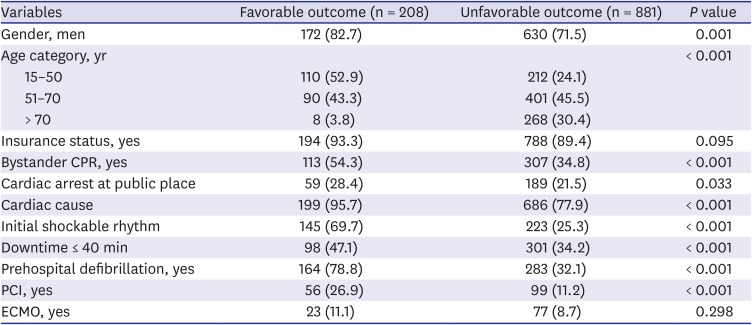
Table 3
Multiple logistic regression analysis for favorable neurological outcomes in patients with downtime > 30 minutes
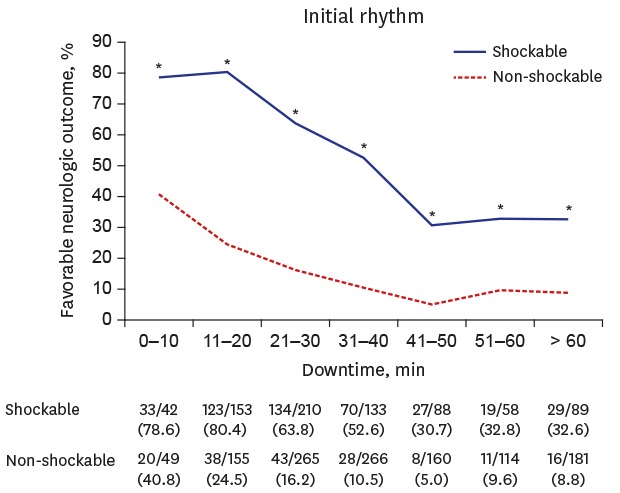
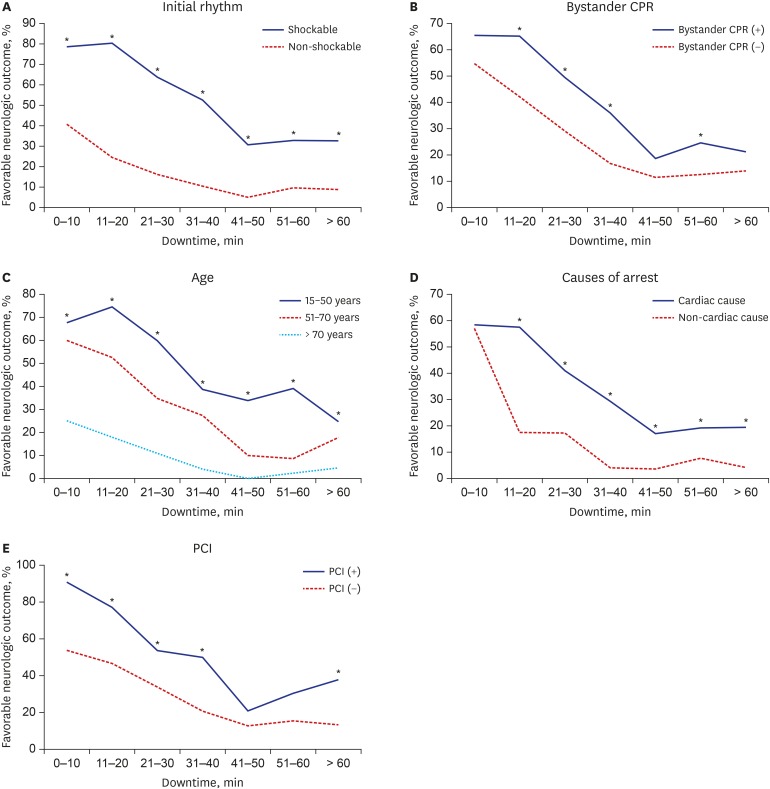
In Fig. 2, each panel shows the relationship between duration of downtime and favorable neurological outcome according to stratified CPR variables. In all downtime intervals, the favorable neurologic outcome rates were greater in cardiac arrest patients with initial shockable rhythm than in those with non-shockable rhythm and it was greater in patients who received bystander CPR than in those who did not. The favorable neurological outcome rates differed according to the three subgroups of age (15–50, 51–70, and > 70), and it decreased with increase in age; these patterns across all downtime intervals were maintained. In turn, the favorable neurological outcome rates according to cause of cardiac arrest and PCI were different in all downtime intervals; patients with cardiac cause and those who received PCI were higher than those who did not.
Fig. 2
Relationship between duration of downtime and favorable neurological outcome according to stratified cardiopulmonary resuscitation variables. (A) Initial rhythms. (B) Bystander CPR. (C) Age. (D) Causes of arrest. (E) PCI.
CPR = cardiopulmonary resuscitation, PCI = percutaneous coronary intervention.
*Significant differences between strata according to cardiopulmonary resuscitation variables.
DISCUSSION
The aim of this study was to determine the neurologic prognosis according to the downtime in witnessed OHCA patients who were treated with TTM, using a nationwide population-based registry. This study showed that with an increase in the downtime, the probability of a favorable neurologic outcome in OHCA patients decreased. However, 19% of the OHCA patients with a downtime > 30 minutes had a favorable neurologic outcome. In patients with a downtime > 30 minutes, patients with age ≤ 70 years, initial shockable rhythm, bystander CPR, cardiac cause, PCI, and downtime ≤ 40 minutes were associated with favorable neurologic outcome.
TTM has shown to improve the neurological outcome of comatose patients after cardiac arrest and current guidelines recommend its use as a standard treatment for post-cardiac arrest patients. Moreover, with reinforced evidence, the recommendation level has improved for patients with cardiac arrest of non-shockable rhythm.15 Camp-Rogers et al.8 reported variability in the patient selection criteria for TTM among the protocols used in different institutions; it was found that 59% of the institutions used specified total ischemic time, a concept similar to downtime, whereas 8% of the institutions utilized a limited total ischemic time within 30 minutes. In a questionnaire study for 96 intensive care units (ICUs) of the Nordic countries, patients presenting with downtime exceeding 30 minutes are not admitted in 11% of the ICUs.16 Based on the results of this study, limiting TTM treatment to patients with downtime < 30 minutes will lead to the exclusion of patients who may benefit from the treatment. Therefore, downtime should not be used as a selection criterion in the TTM protocol.
In 2000, the national association of EMS physician standards and clinical practice committee suggested that EMS responder resuscitation efforts could be terminated in patients who do not respond for 20–30 minutes in advanced life support (ALS).1718 In the 2010 resuscitation guidelines, resuscitation was terminated when there was no ROSC after 3 full rounds of basic life support or no ROSC after full ALS before transport.1819 Therefore, presently, in many EMS systems, patients with OHCA are declared dead at the scene after a predetermined CPR time interval (often 30 minutes).920 Our study suggests that many cardiac arrest patients are likely to achieve a favorable neurologic outcome even after a downtime > 30 minutes. However, there is a lack of evidence for the appropriate duration of CPR. A single-institution study by Kim et al.4 showed good neurological prognosis in 21.7% of patients with downtime > 30 minutes. Moreover, these findings were reproducible in their subsequent multicenter study, which included 858 adult OHCA patients; 18% of the patients with prolonged downtime > 30 minutes were discharged with neurologically intact survival.5 As in our study, these two studies included only OHCA patients treated with TTM. However, these studies included patients with unwitnessed OHCA. Reliable information regarding downtime during cardiac arrest is needed to confirm the relationship between clinical outcome and downtime. Patients with unwitnessed cardiac arrest may not accurately account for downtime because bystanders may not know the exact collapse time. Because our study included only patients with witnessed cardiac arrest, the results may provide more meaningful information on the relationship between downtime and clinical outcome than the previous studies. Meanwhile, the favorable neurologic outcome rate in the abovementioned studies is comparable with those in this study. Unwitnessed cardiac arrest may be an irreversible ischemic insult despite bystander CPR, and it is a well-known unfavorable neurologic outcome factor.21 Therefore, the studies which included both, witnessed and unwitnessed OHCA patients might strengthen the postulation that OHCA survivors with prolonged downtime over 30 minutes can considerably have favorable outcome. The population of the study by Soga et al.,6 which included only witnessed OHCA patients and patients treated with TTM, is similar to our study population. Although the definition of prolonged downtime is different, their study showed a neurologic intact survival rate of 31.5% in patients with resuscitation for more than 25 minutes.6
In addition, there are observational studies with much larger datasets than the present study. Reynolds et al. reported that 99% of subjects with a favorable outcome in 11,368 OHCA patients achieved ROSC within 37 minutes.21 However, CPR > 47 minutes was rarely performed in that study. In our study, patients with downtime > 50 minutes accounted for 22.5%, and 12.5% of these patients were discharged with a favorable neurologic outcome. In a nationwide population-based study which enrolled 282,183 adult bystander-witnessed OHCAs, Nagao et al.18 suggested that prehospital resuscitation efforts should be continued for at least 40–45 minutes to maximize the number of lives saved. However, their study did not account for hospital factors such as TTM and PCI. The difference in the probability of favorable outcome related to downtime according to shockable initial rhythm and bystander CPR is consistent in both the present study and the two large scale studies despite differences in the inclusion of patients who did not achieve ROSC, the witnessed status of subjects in the study population, and the prehospital environment in the study setting. In addition to these two CPR characteristics, we have identified several factors associated with favorable outcome in patients with downtime > 30 minutes in this study. Ahn et al.9 reported that age < 65 years was one of the factors associated with favorable neurologic outcome in patients with cardiac arrest time > 30 minutes. In this study, OHCA patients aged ≤ 70 years had a high probability of a favorable outcome. Especially, OHCA patients aged ≤ 50 years had a 13-fold higher probability of favorable outcome than those aged > 70 years. Previous studies observed an association between age and unfavorable neurologic outcomes in OHCA patients. Terman et al.22 reported that each decade of life was associated with a 21% decrease in the odds of a favorable neurological outcome. In a large dataset which enrolled 18,249 elderly OHCA patients (> 65 years old), survival in older persons decreased linearly by 3% every 5 years.23
In this study, OHCA patients with cardiac etiology had a higher probability of favorable neurologic outcome. This finding is in line with the results of previous studies that the outcome after OHCA of non-cardiac etiology is generally poorer than OHCA with cardiac etiology.2425 These differences were associated with the frequency of shockable rhythm and the proportion of younger patients.2526 More than 30 minutes to ROSC is an unfavorable resuscitation feature that adversely affects the procedural risk/survival benefit of PCI.27 In our cohort, multiple logistic regression analysis showed that PCI was associated with favorable neurological outcome in patients with a downtime > 30 minutes. This result indicates that downtime > 30 minutes is not an absolute predictor of poor outcome and cannot be used for risk stratification of patients for receiving PCI.27 Even if downtime is > 30 minutes, the findings of our study suggest that CPR characteristics should consider for prolongation of resuscitation efforts and the application of post-resuscitation care such as TTM.
The strength of this study is that the median downtime of patients (33 minutes) is longer than that of other studies (range, 13.5–30 minutes).4567182128 In addition, we used nationwide data to collect a large number of samples with prolonged downtime. This study has several limitations. First, the selection bias was inevitable because not all OHCA patients were subjected to the same CPR. Second, the downtime might have been overestimated in patients who experienced re-arrest without sustained ROSC. Third, because the data of this study were obtained from a national registry, there may be a variability in the TTM protocols between different institutions. Although most institutions in Korea follow the current international guidelines on the treatment of post-resuscitation, there are no national standard protocols for providing TTM. Fourthly, we only measured the functional outcome at the time of discharge and did not measure long-term outcomes. Long-term prognostic measures may ultimately be more important in assessing the prognosis of patients with resuscitation. Fifthly, the hospital-based registry did not fully reflect the information of prehospital management by EMS. However, in Korea, EMS responders cannot fully provide ALS, and cardiac arrest patients are transferred to the hospital regardless of ROSC. Therefore, this hospital-based registry would be enough to determine the relationship between downtime and neurological outcome. Sixthly, the downtime is the sum of no flow time and low flow time. No flow time may have a greater impact on neurologic outcomes than low flow time.28 No flow time may occur in witnessed arrest, but no flow time could not be estimated from the data in this study. Lastly, this study included only OHCA patients treated with TTM and did not include patients who died without ROSC. Thus, the overall effect of CPR duration on the neurological prognosis of OHCA patients cannot be addressed in this study.
In conclusion, in this cohort including witnessed OHCA patients treated with TTM, although the favorable neurological outcome rate decreased with an increase in downtime, favorable neurological outcome can occur at considerably prolonged downtimes. Moreover, in OHCA patients with downtime > 30 minutes, age ≤ 70 years, shockable rhythm, bystander CPR, cardiac cause, PCI, and downtime ≤ 40 minutes were associated with favorable neurological outcome. These data suggest that clinicians should not consider the cutoff value for downtime as the only determining factor to provide post-resuscitation care.
 XML Download
XML Download