

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite the fatal natural history of symptomatic patients with severe aortic stenosis (AS), the benefits of a surgical strategy are well established in these patients. However, the management of asymptomatic AS patients remains disputed; wide variation in individual outcomes, the potential risk of complications related to the prosthetic valve, and the risk of valve surgery make it difficult to decide whether to operate (1). Currently, aortic valve replacement has been limitedly applied to patients: those undergoing surgery for coronary artery or concomitant valve disease or aorta or those with associated significantly obstructed coronary artery disease, left ventricle (LV) dysfunction, or progressive decline of LV ejection fraction (LVEF). Although LVEF is well established as an independent predictor of adverse outcome in heart failure, reduced EF is often a late consequence of valve dysfunction. Recent studies suggest that strain imaging reflecting myocardial deformation may identify myocardial injury at an earlier stage before decline in EF (2).
Cardiac magnetic resonance feature tracking (CMR-FT) enable us to evaluate myocardial strain, using routinely acquired CMR cine images. CMR-FT has been validated against speckle-tracking echocardiography, and CMR myocardial tagging techniques, which need sophisticated additional imaging sequences, and burdensome post-processing (345). Furthermore, clinical applicability of CMR-FT has been demonstrated in diverse cardiovascular diseases (367).
Therefore, the purpose of this study was to determine the most valuable CMR strain parameters for evaluating AS, and to assess whether they predict clinical cardiac events (CCEs) in asymptomatic AS patients with preserved EF (pEF).
MATERIALS AND METHODS
Patient Population
The protocol for this prospective cohort study was approved by Institutional Review Board, and all subjects gave written informed consent for the study. Out of the 137 patients with moderate or severe AS enrolled to the prospective registry, 14 patients were excluded for the following reasons: more than a moderate degree of concomitant aortic regurgitation (n = 6), a previous history of cardiac surgery (n = 1), myocardial infarction (n = 7), and suboptimal CMR quality (n = 4). Four subjects had overlapping exclusion criteria. Finally, patients with moderate or severe AS (123 in total; 60 males, mean age, 68 years [range, 31–87 years]; 63 females, mean age, 69 years [range, 42–86 years]) were included in this study (8) (Fig. 1). Patients underwent echocardiography, and CMR imaging within a month. Moderate to severe AS was defined with echocardiography as a maximal transaortic velocity higher than 3 m/sec or a mean transaortic pressure gradient of more than 30 mmHg and an aortic valve area of up to 1.5 cm2 (9). In addition, 32 healthy volunteers (mean age of males, 68 years [range, 61–74 years]; mean age of females, 68 years [range, 60–76 years]) without cardiovascular disease or risk factors, were enrolled prospectively in the control group. The control subjects were matched for age, sex, and body surface area (BSA) with AS patients (10).
Follow-Up
For analysis of the prognostic value of CMR-FT strain parameters in asymptomatic AS patients with pEF, 56 of 123 patients were excluded for the following reasons: 1) patients with LVEF of less than 50% at CMR imaging (n = 15); and 2) patients with dyspnea or other symptoms of heart failure (class III or IV according to the New York Heart Association functional classification system), and patients with typical exertional chest pain or syncope (n = 41) (Fig. 1). Finally, 67 asymptomatic AS patients with pEF were followed-up. The primary endpoint was a composite of CCEs, defined as cardiovascular death, heart failure, and AS-associated symptom development (1112).
CMR Imaging Acquisition and Analysis
CMR imaging was performed using a 3T imager (Trio, Siemens, Erlangen, Germany) equipped with six-channel phased-array coils using standard protocols (13). After acquiring cine images, T1 mapping sequences were obtained. Detailed image acquisition, and analysis can be found in the Supplementary Materials.
CMR-FT Analysis
CMR-FT analyses were performed using a dedicated software (cvi42 version 5, Circle Cardiovascular Imaging Inc., Calgary, Canada). Two-, three-, and four-chamber, and short axis images were used to reconstruct a three-dimensional (3D) model that is used for analyses of LV strain. The preferred images were loaded into the analysis/viewer frame of the software, and analyzed in a random order by two blinded investigators (17 years and 5 years of CMR experience) in consensus.
FT analysis was manually performed by drawing the endocardial and epicardial surfaces in the end-diastolic and end-systolic phases (reference phases), using short axis and long axis cines. Three horizontal long-axis cines including four-chamber, two-chamber, and three-chamber views were tracked to derive longitudinal strain, while short-axis cines were used to derive radial and circumferential strains. Reference points were manually delineated at the right ventricle upper and lower septal insertions into the LV for regional and global analysis of strain and for the generation of polar map views. Cvi42 software interpolated the myocardial contour from the endocardial and epicardial contours of the reference phases and traced its myocardium voxel points throughout the remainder of the cardiac cycle. Strain parameters including peak strain (PS) were obtained automatically in all slices in two-dimensional (2D) as well as 3D manners. A seventeen-segment model was used for assessments of regional and global myocardial mechanics (Fig. 2) (14). 3D longitudinal, radial, and circumferential strain components were derived from averaging the 17-segmental strain curves separately.
Statistical Analysis
Continuous variables are presented as means ± standard deviations and compared using Student's t test. Dichotomous variables are presented as number (percentage) and compared by using the chi square (χ2) test. Bivariate correlation analysis between the various CMR and echocardiographic parameters was performed, using either the linear or the quadratic equation. The strength of correlation is presented as a Pearson correlation coefficient. The cutoff value of CMR strain parameters in discriminating a prognostic effect was determined using receiver operating characteristic (ROC) curve analysis. The prognostic factor of CCE in asymptomatic AS patients with pEF was chosen by logistic regression. The multicolinearity of variables in multivariate analysis was evaluated with colinearity statistics tolerance. The cut-off value of variance inflation factor for detecting multicolinearity was greater than 10 (15). For survival analysis, a log-rank test was performed. Analysis was conducted with SPSS version 23.0 software (IBM Corp., Armonk, NY, USA), with the exception of ROC curve analysis (MedCalc version 9.3.1, MedCalc Software, Mariakerke, Belgium). A two-tailed p value of less than 0.05 was considered statistically significant.
RESULTS
Clinical Characteristics
The entire AS population was categorized according to the degree of AS. None of the clinical characteristics described in Table 1 were significantly different between moderate and severe AS groups. In 32 control subjects with 14 males (45%), mean age was 67.9 ± 4.4 years and mean BSA was 1.64 ± 0.13 m2.
Echocardiographic and CMR Parameters
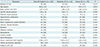
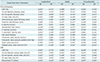
The measurements from echocardiography and CMR are listed in Table 2. The mean LVEF and the mean LV mass index (LVMI) by CMR of the entire AS population were 62.1 ± 14.0% and 96.2 ± 35.9 g/m2, respectively. The LVEF estimated by CMR in the moderate AS group was significantly higher than that in the severe AS group, in contrast to the insignificant result in echocardiographic LVEF. Echocardiographic and CMR LVMIs in the severe AS group were higher than those in the moderate AS group. There were significant differences between moderate and severe AS groups in the following echocardiographic and CMR parameters: echocardiography, interventricular septal thickness, posterior wall thickness, e′ velocity, transaortic peak velocity, mean pressure gradient, aortic valve area, CMR:LV end diastolic and systolic volume indices, and non-contrast T1 (p < 0.05 for all the parameters).
Association between AS and CMR Strain Parameters
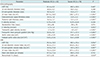
The absolute mean values of global radial, circumferential, and longitudinal PS were significantly reduced in both 2D and 3D measurements in AS patients compared to the controls (p < 0.05 for all) (Table 3). Severe AS patients showed more impaired global PS values than moderate AS patients did (p < 0.05). All 2D and 3D segmental strain parameters showed no significant differences between subgroups (p > 0.05 for all parameters). Trend analysis of control, moderate AS, and severe AS subgroups was performed with a Jonckheere-Terpstra test. The post-hoc analysis demonstrated that the absolute mean values of 2D global radial and longitudinal PSs revealed a significant gradual decreasing trend in the order of control, moderate, and severe AS groups (p < 0.001).
Correlation of Strain Parameters and Other Imaging Indices
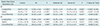
There were significant linear correlations between the global PSs, and various other cardiac imaging indices (p < 0.05) (Table 4). All global strain parameters showed significant linear correlations with all of the CMR measurements including EF, LVMI, LV end-diastolic and end-systolic volume indices, and non-contrast T1 and echocardiographic EF, LVMI, LV end-diastolic and end-systolic diameters, deceleration time, left atrial (LA) diameter, and (indexed) aortic valve area. Especially, EF on CMR and echocardiography, CMR LVMI, and echocardiographic LV end-systolic diameter had moderate to strong linear correlations with all global PSs.
Prognostic Value of Strain Parameters in Asymptomatic AS Patients with pEF
Among total AS patients, 67 asymptomatic patients with pEF were analyzed to find the effective and predictive parameters for prognosis. Their mean age was 68.4 ± 9.6 years. The mean LVEF and LVMI by CMR were 69.0 ± 6.7% and 89.3 ± 32.6 g/m2, respectively. The median follow-up period was 31.1 months (interquartile range, 17.8–41.7). Twenty-two of the 67 patients experienced CCEs during the follow-up period (cumulative event rate 32.8%). Two patients died due to cardiac causes. Heart failure occurred in nine patients. Twenty patients developed AS-associated symptoms, such as chest pain, syncope, and dyspnea. Eight patients suffered from more than one CCE.
Clinical and imaging data of asymptomatic AS patients with pEF are listed in Supplementary Table 1, in terms of presence or absence of CCE. There were significant statistical differences between two groups by using student t test or χ2 test in following: history of diabetes mellitus (DM), echocardiographic LVMI, interventricular septal and posterior wall thickness, e′ velocity, transaortic peak velocity and mean pressure gradient, CMR EF, LV end-diastolic/systolic volume indices, LVMI, non-contrast T1, and all global PS parameters (p < 0.05 for all parameters).
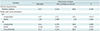
The univariate logistic regression revealed that history of DM (p = 0.015), and all global PSs, except 2D global circumferential PS (p = 0.065), were determined as predictors of CCEs among all clinical and imaging variables (Table 5). Multivariate logistic regression analysis was performed using those predictors for evaluating the prognostic factors for CCE. As a result, the 2D global longitudinal PS (GLPS) remained as a single independent risk factor for CCE {odd ratio = 4.3 (95% confidence interval [CI] = 1.8–10.3), p = 0.017} (Table 6).
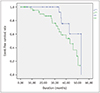
ROC curve analysis for 2D GLPS prediction of CCE revealed an area under the ROC curve of 0.656 and an associated criterion of −17.9%, with a sensitivity of 54.6% and specificity of 76.3% (Fig. 3). The relative risk for CCE was 3.9 (p = 0.016, 95% CI: 1.2–11.9) based on 2D GLPS with a cutoff of −17.9% from which a Kaplan-Meier graph was derived. Kaplan-Meier survival curves demonstrated that if the asymptomatic AS patients with pEF had an impaired value for 2D GLPS, they experienced worse event-free survival than those without impaired values (p = 0.041 by log-rank test) (Fig. 4).
DISCUSSION
The major findings of this study were that 1) 2D global longitudinal and radial PSs were significantly correlated to the degree of AS; 2) global PSs showed linear correlations with cardiac imaging functional indices; and 3) impaired 2D GLPS was associated with increased risk of CCEs.
2D global longitudinal and radial PSs showed increasing impairment from control to moderate AS to severe AS groups. This indicates that subtle changes in longitudinal and radial deformation progress gradually from mild to severe AS. Our result was similar to that using speckle–tracking echocardiography, which also showed a gradual decrease in global longitudinal strain as the severity of AS increases despite an unchanged LVEF (16). Previous studies in severe AS patients using echocardiography or CMR tissue tagging also revealed a significant reduction in circumferential and longitudinal function, even in patients who had no or only mild symptoms (1718). Thus, objective change in myocardial strain can be more sensitive than observable symptoms in detecting functional abnormality in AS.
On the other hand, all 3D strain parameters, even longitudinal ones, showed no statistical significance for predicting prognosis in asymptomatic AS subjects with pEF. This may be explained by dilution of each significant directional component in the data because the 3D strain parameters were derived from various segmental 2D measurements by software-dependent calculation with limited reliability validation (19).
We found significant linear correlations between global PSs. and other traditionally important cardiac indices on CMR and echocardiography in AS. EF showed the best correlation with the strain parameters which themselves reflected the dimensional change in different vectors during LV contraction. EF is a well-established prognostic factor of AS (20). A high LVMI was found to be independently associated with increased cardiovascular mortality in mild to severe AS (21). In AS, LA enlargement could suggest chronically elevated LV filling pressure. The LA diameter was reported to predict the occurrence of symptoms and mortality in severe AS (22). The non-contrast T1 value is known to indicate the degree of myocardial fibrosis as the anatomical change (23). CMR-FT and myocardial fibrosis determined by non-contrast T1 value were well-correlated (24). Considering those facts together, the strain parameters of CMR-FT may be useful outcome parameters of AS without additional T1 mapping or tagging sequences.
We confirmed that an impaired 2D GLPS was an independent predictor of worse clinical outcome in asymptomatic AS patients with pEF, but the other echocardiographic and CMR parameters, including the maximum velocity and mean pressure gradient of aortic valve, LVMI, and non-contrast T1 value were not. This result indicated that assessing the 2D GLPS using CMR-FT in AS patients may provide a further risk stratification over known predictors of clinical outcome. Several recent studies also demonstrated the significant role of longitudinal strain as a prognostic factor of preoperative or postoperative outcome (2425). In a large meta-analysis, global longitudinal strain, assessed by echocardiography, was shown to be more predictive of mortality than was EF in patients with LV dysfunction (26). Taken together, impaired longitudinal strain with equivalent subclinical dysfunction or borderline symptoms should be handled cautiously to avoid adverse delays in intervention (17).
The LV wall is not homogenous and is composed of endocardial, mid-myocardial, and epicardial layers (27). LV function is determined by the sum of contraction and relaxation in these three layers (28). The early stage of myocardial fibrosis in the progression of AS can develop from subendocardial layers. Only longitudinal function could detect the early progression of myocardial fibrosis. It has been reported that circumferential and radial strains cannot detect the early stage of fibrosis progression because they are related to mid wall function (24). Strain imaging has been demonstrated to be the most appropriate method to evaluate LV myocardial contractility properties and myocardial deformation, as strain may enable detection of subtle changes in LV performance in severe AS patients (29).
CMR-tagging has become the reference standard for the evaluation of myocardial strain, and may help to identify patients before the onset of overt myocardial dysfunction (303132). However, CMR-tagging requires specialized tagging sequences and lengthy breath-holds, and the post-processing procedure is laborious and time-consuming (33). It may suffer from progressive attenuation of the tag signal during the cardiac cycle (34). Meanwhile, CMR-FT is available for previously obtained CMR including basic steady-state free precession cine images, and useful for coherent follow-up for the strain parameters. It is also promising to assess strain especially in patients with suboptimal echocardiography quality (24). CMR is free from operator-dependency in contrast to the echocardiography (35).
CMR-FT has some technical limitations in clinical use. First, the FT software algorithm tracks pixels frame-by-frame at the tissue-cavity interface and tracks intra-myocardial pixels. However, the myocardium on CMR is homogeneous, and intrinsically lacks features (36). The second limitation is the temporal resolution, which may not be able to resolve short-lived phases of cardiac motion in CMR. The frame rate depends on the patient's heart rate and various acquisition parameters. Since CMR acquisitions obtain data over several heart beats, minor beat-to-beat differences are smoothed out, which in combination with suboptimal temporal resolution, will obscure rapid iso-volumic phases and might lead to an underestimation of displacement and strain values (303137).
The major limitation of this study is that it is a single center study with a small number of patients. Second, we didn't compare CMR-FT with CMR tagging, which is still considered as the gold standard for strain analysis for research purposes. However previous studies showed reasonable agreement between CMR-FT and CMR tagging in healthy subjects and different diseases including AS (373839). On the other hand, there is no standard reference for CMR-FT. Third, several known risk factors such as age, aortic valve area, and LV systolic function were not demonstrated as the prognostic factors in asymptomatic AS patients with pEF of this study. Because our study population was a heterogeneous mixture of asymptomatic moderate to severe AS patients, it is possible that some parameters that reached borderline significance would predict outcome in a subgroup analysis. Nevertheless, the population size of our final subgroup study was quite small, making further stratified analysis difficult. Lastly, our primary endpoint including the development of AS-associated symptoms was relatively subjective, in contrast to other studies using endpoints covering overt manifestations, such as mortality and heart failure (8). Because the aim of our study focused on early finding suggesting myocardial dysfunction and worse prognosis, the endpoint was designed to measure the subtlest change detectable in a clinical setting (17).
In conclusion, 2D global longitudinal and radial PSs are correlated with the degree of AS and can reflect cardiac dysfunction. 2D GLPS may be one of the most potent predictive factors for CCE in asymptomatic AS patients with pEF. If the asymptomatic AS patients with pEF show the absolute value of 2D GLPS less than 17.9%, they might have worse prognosis compared to the other asymptomatic AS patients with pEF.




 XML Download
XML Download