

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Sepsis is a subset of organ dysfunction caused by a dysregulated host response to infection1 and easily causes cardiomyocyte dysfunction.2 Although the clinical signs and symptoms of heart failure are challenging to identify in patients with septic shock, when cardiac function is evaluated, results commonly show cardiac dysfunction. The prevalence rate has ranged from 64% to 84%.34
Several studies have evaluated cardiac function in patients with sepsis5 with different parameters; cardiac biomarkers and left ventricular (LV) systolic function, diastolic function, and right ventricular (RV) function via echocardiography.678 However, the decrease in LV afterload and preload directly influence the systolic and diastolic function of LV, and the general condition of the patient with septic shock affects cardiac biomarkers. Therefore the objective parameters used in evaluating cardiac function did not properly reflect the actual cardiac function and did not show significant association with the prognosis of patients with septic shock.910 Special echocardiographic parameters of global longitudinal strain and tricuspid annular systolic excursion may reflect the prognosis of patients with septic shock, but more evidence is required.11
We hypothesized that the impairment of LV systolic function may have a non-linear relationship with intrinsic myocardial damage in sepsis but still influence the prognosis of patients with septic shock. Therefore, we aimed to identify the echocardiographic features that can reflect cardiac dysfunction independently from the heterogeneous hemodynamic conditions of patients with septic shock and to investigate its association with in-hospital mortality.
METHODS
Study population
Patients admitted to the intensive care unit (ICU) in our hospital due to septic shock from January 01, 2015 to June 30, 2018, were retrospectively screened. Patients who were 18 years or older and who presented with septic shock and underwent echocardiography within a week from shock development were included in the study. We excluded patients with tachycardia (heart rate, ≥ 150 beats per minute), patients under post-operative condition, and those who were previously diagnosed with structural heart disease such as valvular heart disease, congenital heart disease, and cardiomyopathies or heart failure with more than moderate systolic dysfunction. Patients with coronary artery disease were also excluded. Septic shock was diagnosed according to Sepsis-31; however, we also included patients without serum lactate level if they met the sequential organ failure assessment score, and required vaso-active agents, despite adequate volume resuscitation considering the inclusion period. The presence of coronary artery disease was defined by previous or current evaluation of coronary angiography or coronary computed tomography angiography findings showing more than 70% stenosis at any epicardial coronary artery with or without revascularization.
Data acquisition
Patient data including past medical history, cause of infection, vital signs, and laboratory findings along with cardiac enzyme levels were collected by reviewing their medical records. Then, Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were calculated using the data. Infection sources were categorized into respiratory tract, urinary tract, biliary tract, gastrointestinal tract, and others. When there were several results for the cardiac enzymes, the maximum values which were measured within 3 days from the echocardiographic evaluation were collected for the study. Echocardiographic data were retrospectively reviewed. The primary outcome of the study was in-hospital mortality.
Echocardiography
Conventional echocardiography was performed within 7 days from ICU admission or from the development of septic shock. Echocardiographic measurements were performed using a commercially available ultrasound system (VIVID-Q; GE Vingmed Ultrasound AS, Horten, Norway). Left ventricular ejection fraction (LVEF) was calculated using the biplane Simpson's method from apical four- and two-chamber views. We categorized LV systolic function into four groups: normal for ejection fraction (EF) ≥ 50%; mild systolic dysfunction for EF ≥ 40%; moderate dysfunction for EF ≥ 30%; and severe dysfunction for EF < 30%. Mitral inflow was obtained via pulse-wave Doppler echocardiography using the sample volume between mitral leaflet tips during diastole (E). Mitral annular tissue velocity (e′) was obtained using tissue Doppler imaging with the sample volume on the septal area of the mitral annulus during diastole. Then, LV filling pressure was substituted by E and e′ ratio.12 The patterns of LV wall motion impairment were categorized into four types: normal, diffuse wall motion impairment, ballooning of LV apex or mid walls (Takotsubo cardiomyopathy type)13 and focal wall motion impairment. Focal wall motion impairment was defined as regional wall motion abnormalities that do not follow the wall motion patterns of stress-induced cardiomyopathy, regardeless of whether it follows the territories of a coronary artery or not. To quantify the extent of wall motion impairment, wall motion score index was calculated.14
Statistical analysis
Continuous variables are expressed as mean ± standard deviation or median (from 1st to 3rd quantiles). Categorical variables are expressed as frequencies and percentages. Continuous variables between survivors and non-survivors were compared using the independent t-test and Wilcoxon rank-sum test. Categorical variables were compared using the χ2 test. Disease severity was assessed using the APACHE II score. Event-free survival was estimated using the Kaplan-Meier method and was compared using the log-rank test. Cox proportional hazard regression analysis was performed to evaluate the effect of LV systolic function and patterns of LV wall motion impairment on in-hospital mortality. The parameters that influenced patient survival in the Cox regression model were adjusted in the final model. Statistical analysis was performed using R 3.5.3 (The R Foundation for Statistical Computing, Vienna, Austria) for Windows. In all statistical analyses, a P value < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics of all patients and comparison of values by survival
A total of 208 patients were finally enrolled in the study. The mean age of the participants was 68.7 ± 14.3 years. The mean APACHE II score was 21.3 ± 6.8. Pneumonia was the leading cause of septic shock (126, 60.6%), followed by urinary tract infection (28, 13.5%). The time interval from the development of shock to transthoracic echocardiography was 1 (1–3) day.
In-hospital mortality was 102 (49.5%) in total. No significant difference was observed in age, gender, and underlying disease except for malignancies, which was not significant when Cox proportional hazard regression analysis was performed (Supplementary Table 1). The APACHE II score of the non-survivors was higher than that of the survivors, and the CK-MB and troponin-T levels were higher in the non-survivors than in survivors (Table 1).
Table 1
Baseline characteristics of patients with septic shock
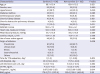
Data are presented as mean ± standard deviation or number (%).
APACHE II = acute physiology and chronic health evaluation II, TTE = transthoracic echocardiography, LOS = length of stay, BNP = B-natriuretic peptide.
aThe use of vaso-active agent when TTE was performed; bTime duration from the diagnosis of septic shock to echocardiographic evaluation.
Cardiac function of patients with septic shock
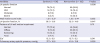
Among all patients, 141 (67.8%) had normal LV systolic function. The LV filling pressure as assessed using E/e′ and the pulmonary artery systolic pressure were slightly increased (13.1 ± 6.1 and 39.7 ± 12.5 mmHg, respectively). Among the patients with impaired LV wall motion, 34, 26, and 10 patients presented with diffuse pattern, ballooning pattern, and focal pattern of wall motion impairment, respectively. When parameters were compared according to patient survival, LVEF and pulmonary artery systolic pressure were significantly different between survivors and non-survivors (P = 0.047 and P = 0.017 respectively) in simple analysis (Table 2).
Table 2
Comparison of cardiac function evaluated by transthoracic echocardiography by survival
LV systolic dysfunction and in-hospital mortality in patients with septic shock
In univariate Cox proportional hazard regression analysis, severe LV systolic dysfunction with LVEF < 30% was significantly associated with higher in-hospital mortality (Supplementary Table 1). Kaplan-Meier curve analysis also showed significant log-rank test results (P = 0.037) (Fig. 1A), which was still significant when age, gender, APACHE II score, heart rate, use of vaso-active agent, and pulmonary artery systolic pressure were adjusted. Risk of in-hospital mortality of patients with severe LV systolic dysfunction with LVEF < 30% was significantly higher than that of patients with normal LV systolic function (hazard ratio [HR], 1.97; 95% confidence interval [CI], 1.04–3.75; P = 0.039), although the risk of in-hospital mortality did not change in patients with mild or moderate systolic dysfunction (Table 3).
Fig. 1
Kaplan-Meier curve for mortality in patients with septic shock. The overall survival in patients with septic shock was compared by the LV systolic function (A) and by the pattern of LV wall motion impairment (B).
ICU = intensive care unit, LV = left ventricular.
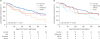
Table 3
The relationship between LV systolic function and in-hospital mortality; the result of multivariable Cox proportional hazard regression analysis adjusted for covariates

LV = left ventricular, HR = hazard ratio, CI = confidence interval.
aAdjusted for age, gender, APACHE II score, heart rate, use of vaso-active agent, and pulmonary artery systolic pressure; bAdjusted for age, gender, APACHE II score, heart rate, use of vaso-active agent, pulmonary artery systolic pressure, and severe LV systolic dysfunction.
Patterns of wall motion impairment and in-hospital mortality in patients with septic shock
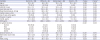
When patients were divided according to patterns of LV wall motion impairment, disease severity characterized by APACHE II score was not different. However, cardiac function, evaluated with B-type natriuretic peptide level and E/e′, was significantly lower and LV systolic function was greater in patients with normal LV wall motion (Table 4). In addition, the overall survival of patients was different according to the patterns of LV wall motion impairment, with lower overall survival in patients with the diffuse pattern of LV wall motion impairment in the Kaplan-Meier curve (log-rank test, P = 0.022) (Fig. 1B). The result did not change even when other covariates were adjusted with multivariate Cox regression analysis. The risk of in-hospital mortality was higher in patients with the diffuse pattern of LV wall motion impairment than in those with normal LV wall motion in multivariate analysis (HR, 2.28; 95% CI, 1.19–4.36; P = 0.013). Ballooning pattern wall motion impairment or focal wall motion impairment did not affect in-hospital mortality (Table 3).
Table 4
Comparison of demographic data and myocardial function of patients with septic shock by the pattern of LV wall motion impairment
DISCUSSION
We evaluated the cardiac function in patients with septic shock and identified the association between the development of myocardial dysfunction and in-hospital mortality via echocardiographic evaluation. In patients with septic shock, LV systolic dysfunction was common, and LV end-diastolic filling pressure and pulmonary arterial systolic pressure were slightly increased. In such condition, significant decrease in LV systolic function with an LVEF < 30% and diffuse pattern of LV wall motion impairment significantly influenced in-hospital mortality.
The development of myocardial dysfunction, referred to as septic cardiomyopathy, is one of the common findings in patients with septic shock. However, the characteristics of septic cardiomyopathy are challenging to define because different patterns of cardiac dysfunction are observed with varying degrees in patients with septic shock. Furthermore, septic shock affects the objective parameters that are used in evaluating cardiac function even when there is no myocardial damage; afterload and preload decrease in septic shock due to the decrease in peripheral vascular resistance.15 This decrease in afterload exaggerates LV systolic function while the decrease in preload reduces LV filling pressure, as reflected in E/e′, and influences stroke volume. With such complexity, conventional parameters, such as LVEF and E/e′, were not associated with the prognosis of patients with septic shock in previous studies. Then, further studies evaluated other parameters, such as myocardial performance index,16 mitral annular posterior systolic excursion, tricuspid annular posterior systolic excursion (TAPSE),17 and global longitudinal strain (GLS) as for prognostic factors in septic shock.1118 Although TAPSE and GLS showed promising results, they are still challenging parameters because they are not usually assessed and commonly reported in routine echocardiographic evaluations, moreover, they require additional high-quality images to get the values and needs more evidences.
With the interest in the development of myocardial damage in septic shock, LVEF was firstly focused as a prognostic factor4 but failed to reveal the significant influence on the prognosis because of the hemodynamic complexity of septic shock. Septic shock patients with normal LVEF may be masking the decreased LV systolic function because of decreased peripheral vascular resistance or may have normal LV systolic function with minimal changes in peripheral vascular resistance. Patients with hyperdynamic left ventricles may have relatively overestimated LV systolic function because of severely decreased peripheral vascular resistance. All these situations were reflected in previous studies with inconsistent relationships between LVEF and patient prognosis.369 However, we assumed that although the relationship between LVEF and the prognosis of the patient might not be linear, there might be a specific range of LVEF which reflects intrinsic myocardial damage, irrespective of the change in peripheral vascular resistance. A significant decrease in LVEF, with or without decreased peripheral vascular resistance, may indicate an absolute decrease in LV systolic function and remarkably influence the prognosis of patients with septic shock. In our study, that specific range was an LVEF < 30%.
When evaluating cardiac function in patients with sepsis, parameters that can reflect intrinsic cardiac function independently from hemodynamic conditions may have advantages. GLS may be better than LVEF as mentioned above.1118 However, high-quality additive images, and more evidence for practical use are required. Therefore, the result of our study that showed the clinical implication of LVEF in patients with septic cardiomyopathy is significant.
There is no consensus on the definition and clinical spectrum of septic cardiomyopathy, which is attributed to its complex and multifactorial pathophysiology. The type of wall motion impairment may also have been challenging to define in septic cardiomyopathy considering that most studies that evaluated the systolic function of LV in patients with septic shock did not present the patterns of wall motion impairment. We also expected the diffuse type in patients with septic shock,19 however, only 34 (16.3%) patients presented diffuse wall motion impairment followed by 26 (12.5%) patients with the ballooning pattern and 10 (4.8%) with focal pattern. The different patterns may differentiate the cause of the myocardial dysfunction in septic shock, but there is a lack of evidence to exclude the possibilities of combination of pathophysiologies for the cardiac dysfunction in the septic shock. Therefore, we may conclude that the dominant type of cardiomyopathy in patients with diffuse LV wall motion impairment is septic cardiomyopathy and that in patients with ballooning pattern of LV wall motion impairment is stress induced cardiomyopathy rather than differentiating patients into septic cardiomyopathy and stress induced cardiomyopathy. However, in patients with ballooning type wall motion impairment, women patients were dominant and 11 of 15 patients who underwent follow-up echocardiography showed improvement of LV systolic function. This implies that patients with the ballooning type of wall motion impairment may follow the characteristics of stress induced cardiomyopathy.
The present study had several limitations, primarily due to its retrospective nature. First, echocardiography was not performed in all patients with septic shock in our hospital. Therefore, the severity of the disease in the study population, who had echocardiography data, may be higher than the severity of average patients with septic shock. And, we were not able to predict the prevalence of septic cardiomyopathy nor to characterize the pattern of cardiac dysfunctions in septic cardiomyopathy. Second, although we excluded patients with coronary artery disease, our study population may still have included patients with coronary artery disease, which might have influenced LV systolic function and patient mortality. Third, the time interval from shock development to echocardiographic evaluation differed between cases. For this reason, the change in LV systolic function at the hyperacute stage of septic shock and its influence on patient outcome may have been missed. Fourth, we did not routinely evaluate central venous pressure. Therefore, we could not obtain data about peripheral vascular resistance and could not analyze the effect of peripheral vascular resistance on the change of LV function in the study patients.
LV systolic dysfunction was commonly observed in patients with septic shock. An LVEF < 30% and diffusely impaired LV wall motion were significantly associated with higher in-hospital mortality. The relationship between LV systolic dysfunction and the prognosis of septic shock became more distinct in this study. However, further evaluation in prospective settings is required for assessing of the prevalence and patterns of cardiac dysfunction considering peripheral vascular resistance.
 XML Download
XML Download