

 PDF
PDF ePub
ePub Citation
Citation Print
Print



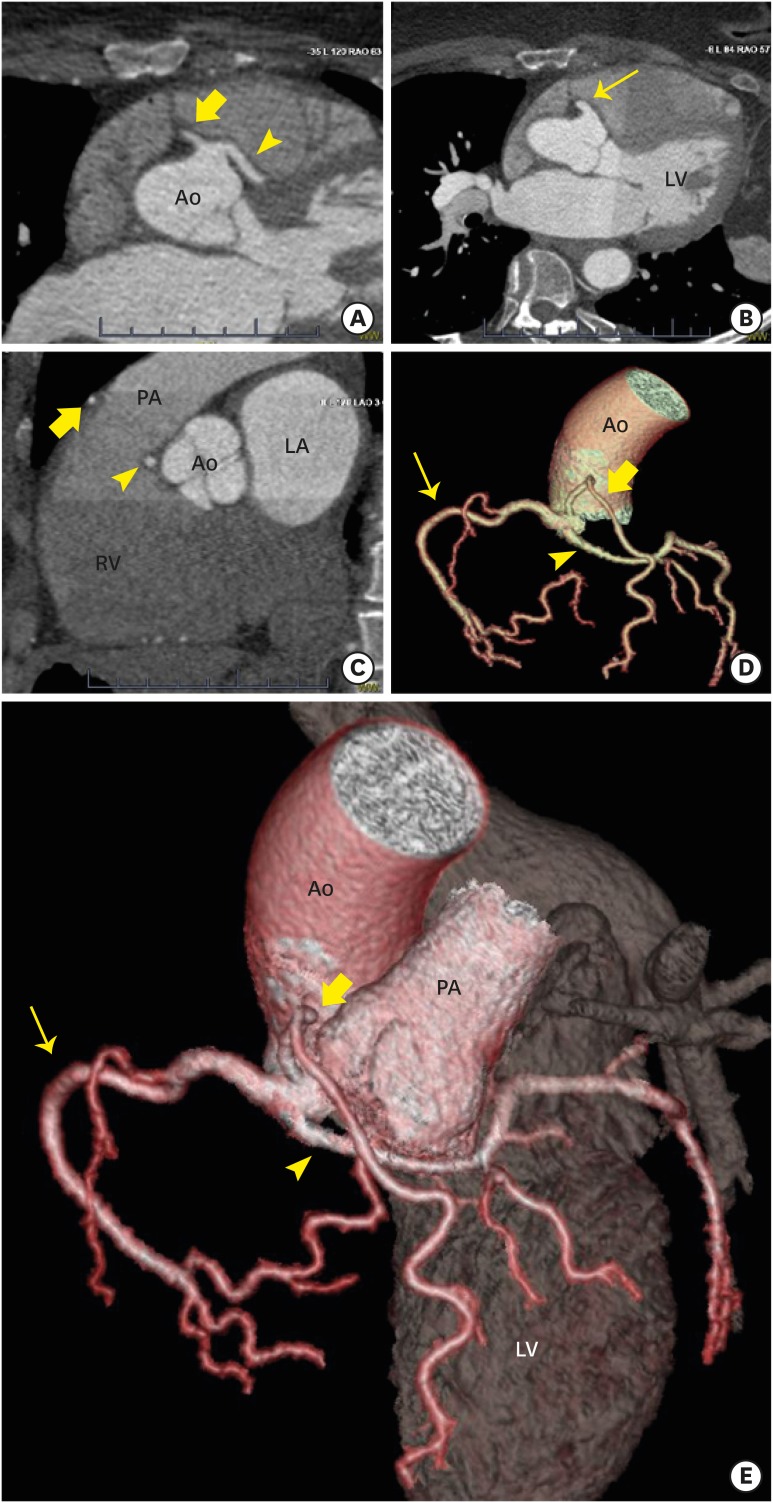
A 63-year-old female, with atypical chest pain had an elevated serum troponin T at 0.05 ng/mL (lab upper limit of normal 0.03 ng/mL) which normalized upon serial testing. As part of her initial workup, she underwent computed tomography (CT) pulmonary angiography which was initially thought to be unremarkable, though secondary analysis suggested an anomalous coronary origin. Subsequently, a dedicated coronary CT angiogram illuminated the coronary anomalies including: anomalous, distinct origins of the left main and long, dual left anterior descending arteries along with a normal right coronary artery emanating from a common ostium off the right coronary cusp without atherosclerotic disease otherwise (Figure 1). Despite a mild initial troponin elevation, the patient’s lack of exertional symptoms, normal myocardial perfusion SPECT, normal 12-lead electrocardiogram even during an episode of chest pain, and relatively older age at the time of discovery suggested a benign prognosis. As such, she was managed conservatively (without surgery) and continues to do well at short-term clinical follow-up.
Coronary anomalies are observed in less than 1% of patients referred for coronary imaging.1) Dual left anterior descending variants are encountered at an even lower rate (0.1% in one series).2) Anomalous left coronary arteries which course in-between the aorta and pulmonary artery (interarterial) and those with acute take-off angles of less than 45 degrees are associated with increased risk of sudden cardiac death while other variants are generally considered benign.1) This case highlights the often occult nature of coronary anomalies, which may be life threatening, and offers a reminder that chest CTs, even when performed for other reasons, may offer a first-glimpse of such anomalies. Fortunately, the particular anomaly discovered here is likely benign though is exceedingly rare, having only been described once before.3)
 XML Download
XML Download