

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Tsutsugamushi disease, or scrub typhus, is an infectious disease caused by Orientia tsutsugamushi and its related bacteria such as Candidatus Orientia chuto. The disease is most commonly transmitted by infected chigger bites. Eschar, a characteristic sign of tsutsugamushi disease, is usually observed at the sites of infected chigger bites in temperate areas such as Korea or Japan, while this sign is infrequently observed in tropical areas. For this reason, Fletcher coined the term “scrub typhus” for a typhus-like illness exhibiting no eschar [1], whereas the term “tsutsugamushi disease” has been used for approximately 140 years in Japan for a febrile disease exhibiting eschar and regional lymphadenopathy [2]. Additionally, the mortality of the above two diseases is known to differ markedly, i.e., low in the former versus high in the latter disease at that time.
Recent reports on eschar in tsutsugamushi disease are focused on its incidence, location, number, pathogenesis, evolution, and usefulness for polymerase chain reaction. Previously, several articles described eschar size mainly in Japan [345678]. From these data, it could be summarized that the average eschar size was 2 – 6 mm and the largest one was 8 mm until the 1950s. Thereafter, there are no systematic studies on eschar, and occasionally case reports describe eschar sizes [9101112131415]. For example, the size in foreigners from non-endemic areas seems to be large; 15 mm in a British soldier and 20 mm in a Swedish traveler [1012].
The factors affecting the size and morphology of eschar have not been thoroughly investigated. In an experimental human volunteers study, both the interval and antigenic relatedness between the initial and subsequent infections are involved in development of systemic symptoms and eschar. In subjects with recent previous infection with O. tsutsugamushi, erythema only was formed at the inoculation sites. In patients reinfected 1 – 2 years after recovery from tsutsugamushi disease, a papule was formed at the inoculation site and did not progress to a necrotic ulcer. In those who did not have previous tsutsugamushi disease, papules were formed around 4 – 5 days after the inoculation. The dermal lesions usually remained static with chloramphenicol therapy, which was administered 1 or 2 days after the development of fever, but three of the 14 inoculation lesions progressed to necrotic lesions. When the primary and reinfected tsutsugamushi diseases are compared, the sizes of the erythema and possibly of the eschar in reinfected tsutsugamushi disease are smaller compared to the primary tsutsugamushi disease [16].
O. tsutsugamushi organisms persist asymptomatically in humans after recovery from tsutsugamushi disease [1718], suggesting that this infection exerts prolonged immunologic and other biological effects than those due to non-persisting organisms. Additionally, persons who have the chronic infection and continuously reside in endemic areas of tsutsugamushi disease may contract this infection repeatedly; however, even in Japan, reports of patients who have suffered tsutsugamushi disease more than once are rare [56]. In countries other than Japan, there are only scattered cases of repeated symptomatic O. tsutsugamushi infection [161920]. Despite the rarity of clinically evident repeated tsutsugamushi disease, many patients in endemic areas who have no history of tsutsugamushi disease exhibit immunoglobulin G (IgG)-dominant antibody responses to O. tsutsugamushi [21], which may represent the symptomatic reinfection. Bourgeois and colleagues described that the serologic patterns of scrub typhus could be divided into two groups, i.e., the primary infection (immunoglobulin M (IgM) antibody response) and reinfection (IgG antibody response) types. Patients with the IgM antibody response type were younger, exhibited higher frequencies of rash and conjunctivitis, and had a good antibiotic response and a higher recurrence rate after completion of antibiotic therapy. Conversely, the IgG antibody responders were older, had lower frequencies of rash and conjunctivitis, and exhibited an excellent response to antibiotic therapy and a lower relapse rate [22]. The clinical features in patients with the IgG response type seem to be milder than those with the IgM response type, which is consistent with O. tsutsugamushi reinfection.
From the above evidence, we hypothesize that many of residents in endemic areas of tsutsugamushi disease might be reinfected with this bacteria frequently irrespective of the development of relevant symptoms and will exhibit the IgG antibody response type. If they develop fever, they will exhibit smaller eschars compared to the residents in areas with low incidence rate of tsutsugamushi disease. A papule as an inoculation lesion might be observed because the papule might persist and not progress to a necrotic lesion in patients with relatively high immunity.
Materials and Methods
Jeju Island is the largest island in Korea and is located approximately 100 km south from the Korean Peninsula. Its mean annual temperature and rainfall are the highest in Korea, i.e., 15.8°C and 1,497 mm, respectively. In this context, Jeju Island, particularly Seogwipo-si, is a subtropical area. These environmental conditions suggest that Jeju Island has the most suitable habitat for mite or tick population in Korea. The island consists of two cities, Jeju-si in the northern part and Seogwipo-si in the southern part. The former is a relatively urban area, whereas the latter is a rather rural area. The main industry of Seogwipo-si includes agriculture including citrus farming, livestock farming, tourism, and fisheries.
Although the number of tsutsugamushi disease in Jeju Island patients that is formally reported to the Korea Centers for Disease Control and Prevention is not the highest among all the provinces of Korea [23], the incidence rate of tsutsugamushi disease in Namwon County of Seogwipo-si was very high, i.e., 629 per 100,000 persons [24]. Additionally, the seropositive rate in asymptomatic persons on Jeju Island was the highest (11.7%) compared with that in other provinces of Korea (4 – 5%) [25]. Therefore, the incidence rate of tsutsugamushi disease on this island might be the highest in Korea, although it might be underreported, and it is unknown why the report is so low.
Seogwipo Medical Center is a 290-bed public general hospital that is mainly involved in performing primary care to patients. Any sick person within the city can visit the hospital within 60 minutes and can receive medical care without significant financial burden. Inha University Hospital is an 860-bed university hospital located in Incheon. Incheon is located northwest of the Korean Peninsula, is a metropolitan city, and includes 2.7 million people. City dwellers are rarely exposed to rural environment unless they visit the outskirts of Incheon, but sometimes, patients from nearby rural areas or islands including Ganghwa Island were admitted to the hospital. Thus, this city was chosen as an area endemic of tsutsugamushi disease with lower incidence.
1. Patients
In- or outpatients with relevant clinical features were screened with serologic tests. IgG and IgM antibodies against O. tsutsugamushi were measured using the indirect immunofluorescent (IF) assay at the Jeju Health and Environmental Institute. If this test is not possible, patients' sera were sent to a commercial laboratory for the measurement of the pooled IF antibodies. The positive cutoff titer in the present study was defined as 1:40 because the evaluated patients presented with typical clinical and epidemiologic features. All serum specimens were collected within 2 weeks after the onset of illness. The following factors were recorded: the size, location, and number of eschar, the duration of fever before hospital visit, and the presence of lymphadenopathy and rash, in addition to basic demographic and laboratory findings. Although patients who were managed at Inha University Hospital were not well systematically investigated, records on the eschar size were available in some patients.
The study protocol was reviewed and approved by the Inha University Hospital Institutional Review Board (registration number: INHAUH 2019-05-026-001). The need for patient consent was waived due to the retrospective nature of the study, but the consents were obtained from patients whose photographs were taken.
2. Statistical analysis
Continuous variables were expressed as median and 95% confidence interval (95% CI). Mann-Whitney U tests were used for the comparison of two independent values, and contingency tables were analyzed using Fisher's exact test. MedCalc Statistical Software version 18.11.6 (MedCalc Software bvba, Ostend, Belgium) was used for statistical analyses. All P values were two-tailed, and P <0.05 was considered statistically significant.
Results
1. General feature of tsutsugamushi disease on Jeju Island
From March 2018 to February 2019, 37 patients with tsutsugamushi disease were diagnosed at Seogwipo Medical Center, and 14 patients were excluded because of inadequate description on eschars. Thus, a total of 23 patients in Seogwipo-si were examined in this study (Table 1). One case was infected outside the island and was managed at Seogwipo-si. Two patients were not indigenous persons of Jeju Island; one was a construction worker and the other an immigrant who had resided on Jeju Island for 2 weeks and 3 years, respectively. In Incheon, 12 patients who had been managed between 2016 and 2018 were reviewed. Those who did not exhibit the presence of eschar were excluded.
Table 1
Characteristics of the enrolled patients and differences in some clinical features between Seogwipo-si and Incheon-si
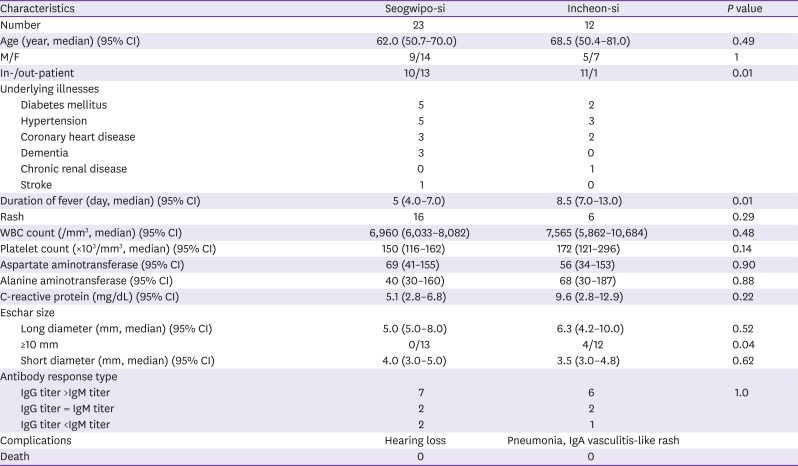
IgG and/or IgM antibodies were positive in 11 patients. Seven of the 11 patients revealed higher IgG titers than IgM titers, i.e., the antibody response to reinfection, two patients had equal IgG and IgM titers, and two patients displayed the IgM response type. Despite such a serologic evidence of past infection with O. tsutsugamushi, no patients recalled their previous episode of tsutsugamushi disease. The remaining 12 patients were diagnosed with tsutsugamushi disease with positive pooled IF antibodies.
2. Early inoculation lesions of tsutsugamushi disease
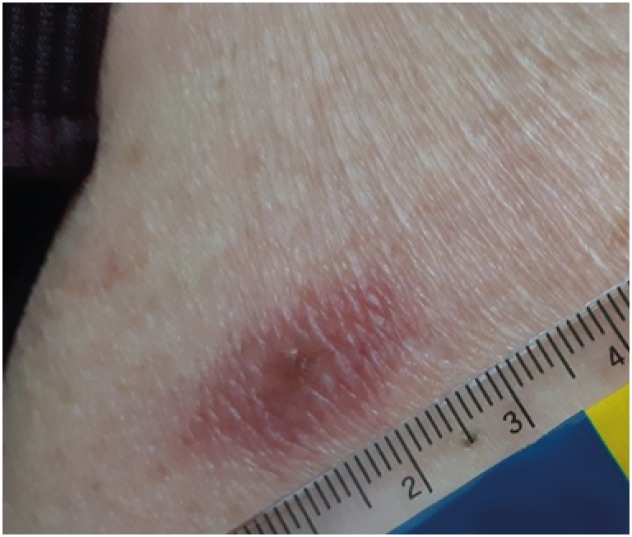
Six of the 23 Jeju Island patients presented with early inoculation lesions of tsutsugamushi disease, i.e., a papule or a vesicle. Three patients presented with papules. Case no. 1 was an 84-year-old man who presented to our hospital with a fever of 12 hours' duration. He harvested citrus fruits both 11 and 12 days before admission and developed rashes on the trunk before the onset of fever. A fever developed suddenly. A 2-mm-diameter papule was observed on the left side of the back, and the diameter of the surrounding erythema was 11 × 26 mm. Tender regional lymphadenopathy in the left axilla was palpated. One day after doxycycline therapy, the papule remained unchanged, but the erythema decreased to 11 × 20 mm (Fig. 1). Titers of the IgG and IgM antibodies were 1:64 and <1:16, respectively. Case no. 2 was an 84-year-old woman who visited our emergency room (ER) due to fever of 3 days' duration, and the patient developed shock, which was possibly related with antipyretic therapy. A 3-mm-diameter papule was observed on the left buttock. Erythema surrounding the papule was wide and rash was observed on the trunk. Case no. 3 was a 49-year-old woman who presented with a fever and a papule measuring 3×5 mm on the lateral cantus of her left eye on the first day of fever. Edema of the left eyelid was noticed, and regional lymphadenopathy in the neck was tender. With doxycycline therapy, the inoculation lesion did not progress to an eschar.
Figure 1
A 2-mm-diameter papule is observed on the back of the patient who presented on hospital 2 day after the onset of fever. Generalized macular rashes are already present. One day after doxycycline therapy, the surrounding erythema reduces in diameter from 11 × 26 mm initially to 10 × 20 mm.
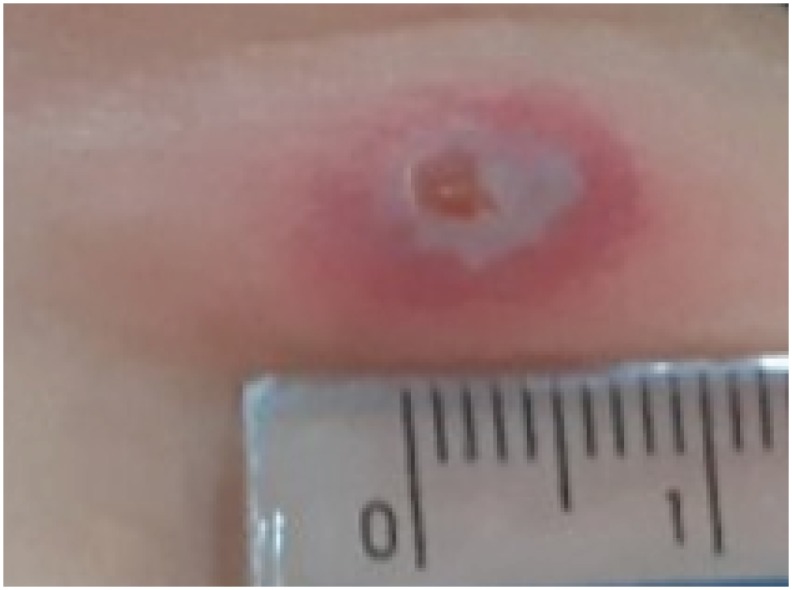
Three patients presented with ruptured vesicles. Case no. 4 was a 38-year-old woman who had been residing in Seogwipo-si. Severe myalgia developed 9 days after harvesting citrus fruits, and the patient presented to our outpatient clinic (OPD) with severe myalgia of 3 days' duration accompanied with mild night sweating, but a definite fever was not documented, i.e., the body temperatures were 36.6°C in the ER and 36.9°C in the OPD. A ruptured vesicle measuring 5 × 8 mm in diameter was noted on the right axilla, and the surrounding erythema was 10 × 18 mm in diameter (Fig. 2A). Tender regional lymph nodes were palpated, rash was not observed, and splenic dullness was increased. After doxycycline treatment for 4 days, the size of the inoculation lesion shrunk to 1×4 mm, and the lesion did not progress into a necrotic eschar; no vesicular membrane was observed (Fig. 2B). Case no. 5 was a 67-year-old woman who noticed an insect bite-like skin lesion 3 days before the onset of fever and visited our ER for a complaint of fever of 12 hours' duration. Tsutsugamushi disease was diagnosed, and a partially denuded, ruptured vesicle measuring 5 × 7 mm in diameter was observed on the right femoral area. Erythema surrounding the vesicle measured 8 × 12 mm in diameter (Fig. 3). Tender regional lymphadenopathy was palpated. After 4 days with doxycycline therapy, patient's condition improved, but her weakness remained. The vesicle became a dark necrotic lesion, and surrounding erythema decreased in width. Case no. 6 presented with chilliness for 3 days and rashes on the trunk. A ruptured 7-mm-diameter vesicle with rather narrow surrounding erythema was observed on the trunk. One patient in Incheon recalled that he initially noted a vesicular inoculation lesion, which later progressed into a necrotic lesion.
Figure 2
(A) A ruptured vesicle is observed on the left axilla, who presents on day 4 of myalgia. The size is 5×8 mm with the surrounding erythema of 10 × 18 mm. (B) Four days after doxycycline medication, the inoculation lesion regresses to 1 × 4 mm and does not progress to a necrotic lesion.
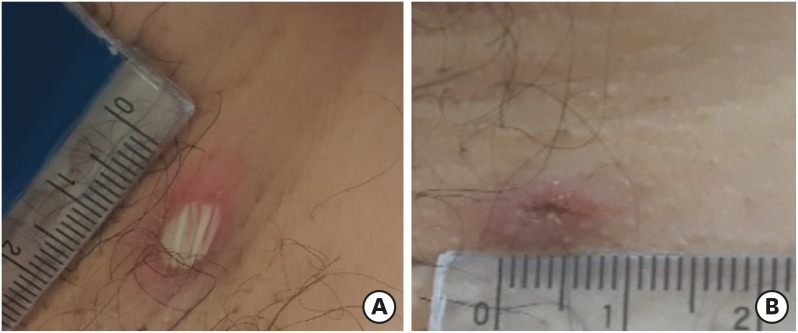
Figure 3
A partially denuded vesicle is observed on the right femoral area in a patient who presented on day 2 of fever. The size of the vesicle is 5 × 7 mm with the surrounding erythema of 8 × 12 mm. Four days after management with doxycycline, the vesicle progresses to a necrotic lesion of 3 × 5 mm in size.
3. Eschar
In Jeju Island patients, no inoculation lesions were found in three patients, and 14 patients had necrotic ulcers covered with dark scabs. The number of the eschar was only 1 in 13 patients, and multiple eschars were observed in one patient. In the patient with multiple eschars, a total number of definite eschars were 5; the largest one was located on the chest, with a diameter of 2 mm; and the remaining 4 eschars were 1 – 1.5 mm in diameter.
Locations of the eschar including the early inoculation lesions, after excluding one patient with multiple eschars, were in the abdomen (5 patients), axilla (3), inguinal area (3), chest (2), back (2), hip (2), face (1), and above the knee (1). All inoculation lesions were round or elliptical, and no spindle-shaped eschar was observed.
After excluding the early inoculation lesions (6 patients), multiple eschars (1), and absent eschar (3), the median long and short diameters of eschars in 13 patients were 5 (95% CI, 5 – 7.5) × 4 (95% CI, 3 – 5) mm, and the medians of the eschar sizes did not differ between the two cities (P = 0.46 by Mann-Whitney U test) (Table 1). When the eschar areas, instead of eschar diameters, were compared, this comparison was also not significantly different (data not shown). Notably, 4 of the 12 patients had eschars ≥10 mm in size in Incheon, whereas none of the 13 patients had eschars ≥10 mm in size in Seogwipo-si, which was significantly different (P = 0.04 by Fisher's exact test).
The median diameter of eschars in patients with the IgG antibody response type was 5 mm (95% CI, 4 – 8), while that in the IgM responders was 6.5 mm (95% CI, 6.1 – 6.9) (P = 0.483 by Mann-Whitney U test). The eschar size in two immigrants from the Korean Peninsula seemed to be larger compared to that in indigenous Jeju Island residents (8 mm vs. 5 mm in Jeju indigenous patients), though the difference was not statistically significant (P = 0.058 by Mann-Whitney U test).
Discussion
One feature of tsutsugamushi disease on Jeju Island is that the early inoculation lesions are occasionally observed. Nowadays, an eschar usually means a necrotic ulcer covered with a dark scab or less frequently a shallow ulcer, while the old Japanese literatures on tsutsugamushi disease described that a mite bite site could be presented as a papule, vesicle, pustule, ulcer, or necrotic dark scab [5]. Tanaka asserted in 1929 that one of papule, vesicle, or eschar, with tender regional lymphadenopathy, was a constant feature of tsutsugamushi disease [26], while there are very few clinical reports on these lesions in the English literatures. Inoculation experiments more clearly depict the evolutional changes of infected mite bite sites. Vesiculo-papules were formed at the inoculation sites 5 days after the inoculation, and then, these lesions progressed to necrotic lesions in an experimental infection using rhesus macaque [27]. Papules and necrotic lesions were observed in human volunteers [16]. Thus, the papular and vesicular lesions observed in the present study are definitely the initial cutaneous lesion after infected mite bites. Furthermore, the antibiotic effect on evolution of the early inoculation lesions was observed in the present study. We followed up the two patients with papules, which did not progress into necrotic lesions with doxycycline therapy. Suto described a patient with tsutsugamushi disease, with a papule of 4 mm in diameter that did not progress to a necrotic lesion with minocycline therapy [28]. Contrary to the papules, the vesicles in two of three patients in the present study progressed into necrotic lesions under doxycycline therapy. From these observations, if antibiotic therapy is administered early at the time of vesicle formation, progression of vesicle into necrotic lesion might be prevented.
It remains unclear why the early inoculation lesions were so frequently observed in Seogwipo-si. We hypothesize that the situation in Seogwipo-si might be similar to that in Japan. This island is still a rural society, and many residents are involved in citrus farming, which is comparable to silk farming on Izu Shichito Islands. Additionally, scrub and/or citrus trees are abundant around Jeju Island residents' houses, similar with mulberry trees on Izu Shichito Islands [29]. Pesticides are least used in both areas because of organic farming in citrus farms on Jeju Island and silk farming on the Shichito Islands. Insects and insect bites, therefore, are common. As for “classical type tsutsugamushi disease” (i.e., tsutsugamushi disease in Japan before the 1950s), Niigata, Yamagata, and Akita Prefectures were endemic of this type of tsutsugamushi disease; riverside areas were abundant of bush and tall grasses, and workers entering these areas were heavily exposed to mites. Pesticides were not available at that time in Japan. In addition to the above risk factors for mite bites, Yokote Hospital, the hospital that Tanaka had practiced for approximately 50 years in Akita Prefecture, and Seogwipo Medical Center are municipal hospitals, so these hospitals are similar in many aspects. The hospitals exist in close proximity with the residents and pose light financial burden, so patients visited these hospitals early in their illness. The duration of illness in the present study, therefore, was somewhat shorter compared to that in Incheon (5 vs. 8.5 days).
Although the present study did not observe an ulcer-like eschar, it is occasionally observed in the clinical practice particularly when it occurs on the armpit or genital area [3031]. Possibly inflammatory exudate on necrotic ulcers is continuously moistened by sweat and thus cannot be hardened to be firmly attached to the ulcer base. Due to its locality and morphology, it can be misdiagnosed as a chancre of syphilis, particularly in young soldiers or persons [330].
Apart from the above early inoculation lesions, eschars in Jeju Island patients presented with another feature, i.e., they are small in diameter compared to those in Incheon. The eschar sizes in Jeju Island patients seemed to be similar or slightly larger by 1–3 mm compared to those observed in Japan before the 1950s. More studies are needed to know the exact distribution of the eschar size, and until then, tentatively, 9 or 10 mm may be the size that differentiates a large eschar from a small one. Eschar size is affected by immunity [16]; however, no convenient method to measure the degree of protective, particularly cell-mediated, immunity against O. tsutsugamushi is available currently. Although IgG and IgM antibodies, as a marker of immunity, were measured in the present study, these antibodies are merely a surrogate marker for cellular immunity and have poor values predicting the immunity. Hence, we did not find any association between IgG antibody positivity and the eschar size. It will be better to measure markers representing cell-mediated immunity, such as CD8+ T cells or interferon -γ, instead of those for humoral immunity [32]. However, even such tests cannot differentiate frequent O. tsutsugamushi reinfection from infrequent one.
The third feature of tsutsugamushi disease in Seogwipo-si is a benign nature of this illness. In the present cases, death and serious complications including pneumonia, acute kidney injury, and encephalitis were not observed. The previous study at a university hospital that was located in Jeju-si also reported that death among the 138 patients was not observed [33]. Furthermore, the low mortality was achieved in the present patients that included a large number of elderly patients and patients with comorbid conditions. We propose that eschar size may be one index to predict the prognosis of tsutsugamushi disease, as Ueno suggested in 1956 [7].
The fourth feature of tsutsugamushi disease in Seogwipo-si is that certain patients take an atypical course. In typical tsutsugamushi disease, mite bites are followed by fever 7–10 days after, then rash becomes apparent 3 – 5 days after the onset of fever, and various complications including pneumonia and encephalitis occur 7 days after the fever. However, in case no. 1, a rash developed before the onset of fever. The patient who presented with multiple eschars also presented with rash at the time of the fever. If a rash was a presenting symptom in the absence of fever, it might be misdiagnosed as a dermatologic disease.
This study had some limitations. First, although we used IgG and IgM antibodies for differentiating the primary infection from the reinfection, there are many cases of undetermined antibody response type, i.e., equal IgG and IgM titers. Second, the association between the eschar size and various indices including past infection (i.e., IgG and IgM antibodies) and antigenic relatedness (immigrants) was investigated, although very few patients had these features. Third, no eschar was found in some patients, which is due to either true absence of eschar or our failure to find it. This ambiguity is present in all studies on eschar of tsutsugamushi disease and cannot be resolved with certainty, and therefore comparison of eschar size may be less prone to error than comparison of just its presence or absence.
 XML Download
XML Download