

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of acute kidney injury (AKI) is approximately 20–50% in patients with advanced liver cirrhosis (LC).123 AKI is associated with a four-fold increased risk of mortality.4 Prerenal azotemia (PRA) is the most common cause of AKI in patients with LC, followed by hepatorenal syndrome (HRS) and acute tubular necrosis (ATN), with prevalence rates of 68%, 25%, and 33%, respectively.1
The diagnostic criteria of AKI have changed over time. The prognosis of patients with LC and AKI is poor; AKI in patients with LC has attracted increasing attention. The recently revised definition of AKI in patients with LC highlights the need to address elevations in the serum creatinine (sCr) level immediately, even small elevations. The differential diagnosis of HRS still requires 48 hours of observation during albumin infusion.5 AKI management varies according to etiology. Therefore, biomarkers differentiating HRS from other diseases are needed. Recently, the levels of urinary neutrophil gelatinase-associated lipocalin (u-NGAL), L-type fatty acid binding protein (L-FABP), interleukin-18 (IL-18), and kidney injury molecule-1 (KIM-1) have been suggested to assist in the differential diagnosis of AKI in patients with LC.678910 Several studies have suggested that u-NGAL facilitates the early detection and differential diagnosis of AKI in patients with LC. The u-NGAL level in HRS is between that of ATN and PRA.671112 ATN has the highest level of u-NGAL protein because the u-NGAL protein is synthesized by an injured kidney epithelium.6 On the other hand, Korean data supporting the clinical utility of the u-NGAL level are scarce. Therefore, this study examined the utility of the u-NGAL level for AKI management in patients with LC.
SUBJECTS AND METHODS
1. Patients
Between October 2015 and June 2016, this study enrolled patients hospitalized with LC and grade 1 AKI (based on the recent International Club of Ascites-AKI criteria).13 During this period, consecutive LC patients with AKI, who were admitted to Sanggye Paik Hospital, were enrolled prospectively. In addition, LC patients with AKI who were hospitalized for other causes were included. The LC diagnosis was based on a combination of laboratory data, such as thrombocytopenia (platelet <100,000/mm3), hypoalbuminemia (albumin <3.5 g/dL), and PT prolongation (INR >1.7), in addition to abdominal imaging (liver surface nodularity, splenomegaly, and portosystemic shunting) and endoscopic findings (esophageal and/or gastric varices).14151617 AKI, which was defined using the new International Club of Ascites-AKI criteria, in patients with LC is characterized by an increase in the sCr level of ≥0.3 mg/dL (≥26.5 µmol/L) within 48 hours and/or ≥50% of the baseline value.35 The inclusion criterion was AKI in patients with LC who were over 18 years old. Of these, patients without baseline sCr data were excluded. The Institutional Review Board of the Inje University Sanggye Paik Hospital approved this study (IRB No. 2015-05-15). Written informed consent was obtained from all the participants enrolled in this study and/or their legal guardians.
2. Data collection
Blood samples were collected on the day of AKI diagnosis (on admission), and a complete blood cell count, PT, and levels of serum protein, albumin, AST, ALT, total bilirubin, and creatinine (Cr) were determined. Cr was measured at three time points. The baseline Cr level was the most recent stable measurement (within the 3 months prior to the index hospitalization). In patients lacking such data, the sCr level upon admission served as the baseline level.35 The event Cr level was that measured at the time of the AKI diagnosis. The peak Cr level was the highest Cr level during hospitalization. u-NGAL testing was performed at the time of the AKI diagnosis. Survival was monitored until December 2016.
Clinically, AKI patients were divided (by physician consensus) into three subgroups according to the etiology: PRA (group 1), HRS (group 2), and ATN (group 3). A diagnosis of PRA was made in patients with a history of volume depletion associated with the fractional excretion of sodium <1%, and a return of the sCr level to within 25% of the baseline by 48 hours after volume replacement.18 A diagnosis of HRS was made using the International Ascites Club criteria: if improvement was not evident after 48 hours of diuretic withdrawal and volume expansion with albumin; in the absence of shock; and in the presence of nephrotoxic medication, parenchymal kidney disease (absence of proteinuria >500 mg/day), microhematuria, and abnormal kidney imaging findings.5 A diagnosis of ATN was made in those exposed to nephrotoxic agents or exhibited volume depletion and fractional excretion of sodium >2%.19 Urine samples used for u-NGAL testing were collected at the time of the AKI diagnosis and were centrifuged immediately after collection at 2,000 G for 10 minutes. The supernatant was stored at −80℃ for batched analysis. The u-NGAL level was measured by an immunoassay (employing the ARCHITECT platform, Beckman coulter AU5800; Bioporto, Copenhagen, Denmark).
3. Endpoints
Based on the measurements of the u-NGAL level, this study examined whether there were significant differences between the three causes of AKI in LC patients in this study.
4. Statistical analysis
The categorical variables are expressed as numbers with percentages and continuous variables as medians with ranges. These parameters were compared using a chi-square test or Fisher's exact test and a Student's independent t-test. Comparisons between the three groups were performed using an ANOVA, and comparisons between any two of the groups were performed using a Student's independent t-test. Univariate Cox regression analyses of sex, age, etiology, natural logarithm (Ln) of PT, albumin level, Ln total bilirubin level, Ln baseline Cr level, Ln event Cr level, Ln peak Cr level, Ln u-NGAL level, model for end-stage liver disease (MELD) score, and the presence of hepatocellular carcinoma (HCC) were conducted to determine their association with in-hospital mortality. The total bilirubin and Cr levels were not distributed normally and were analyzed on a logarithmic scale. The MELD score has been used to predict the survival for patients with advanced LC. The score was calculated according to the bilirubin, PT, Cr, and dialysis. The event Cr level was applied to the MELD score calculation. Variables with significant differences in the univariate logistic regression analyses were subjected to multivariable regression analysis. A p-value <0.05 was considered significant and was used to select the variables for inclusion into multivariable Cox regression. All statistical analyses were performed using SPSS ver. 21.0 (IBM, Chicago, IL, USA).
RESULTS
1. Baseline characteristics
Fifty five patients with LC and AKI were enrolled, of whom 28, 9, and 18 were classified into the PRA, HRS, and ATN groups, respectively (Table 1). Seventy-five percent of the patients were male, and the proportions of males were similar in the three groups (61–80%). The median Child-Pugh and MELD scores were 10 (range, 5–14) and 21 (range, 7–47), respectively, and were comparable between the groups. Eighteen patients developed either a urinary tract infection or other infections. Urinary tract infection was the most common infection, and its incidence was similar in the groups. The median baseline sCr level differed significantly between the groups, particularly between the PRA and HRS groups and between the ATN and HRS groups. The median sCr levels in the PRA, HRS, and ATN groups were 1.44 (range, 0.60–3.40), 1.56 (range, 1.42–2.80), and 1.68 (range, 1.08–13.17) mg/dL, respectively. The difference in the event sCr level was significant only between the PRA and HRS (p<0.001) or ATN (p<0.001) groups. The event sCr level was similar in the HRS and ATN groups (Table 2).
2. u-NGAL levels of the three AKI groups
The median u-NGAL levels in the PRA, HRS, and ATN groups were 37 (range, 10–359), 134 (range, 48–477), and 2,625 (range, 247–3,000) ng/mL, respectively. The median Ln u-NGAL levels in the PRA, HRS, and ATN groups were 3.6, 4.9, and 7.9 Ln ng/mL, respectively (Fig. 1). The median Ln u-NGAL level was much higher in the ATN group than in the PRA and HRS groups (Table 2).
Of the 55 patients, 17 (30.9 %) died prior to discharge. The in-hospital mortality rates in the PRA, HRS, and ATN groups were 7.1% (2 of 28), 55.5% (5 of 9), and 55.5% (10 of 18), respectively. The median survival times of the patients who died prior to discharge were 18, 5, and 12 days in the PRA, HRS, and ATN groups, respectively. The cause of death in the two patients in the PRA group was HCC progression. The causes of death in the HRS group were HRS progression in four patients and esophageal varix bleeding in one patient. In the ATN group, the causes of death were sepsis due to spontaneous bacterial peritonitis in two patients, liver abscesses in two, varix bleeding in two, cardiac arrest in one, and HCC progression in three patients.
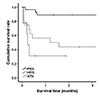
3. Survival curves according to the cause of the AKI and u-NGAL level
Regarding the survival curves according to the cause of AKI, the median survival times in the PRA, HRS, and ATN groups were unavailable (range, 9.8–12.7), 0.2 (range, 0.1–1.3), and 1.2 (range, 0–3.4) months, respectively. The difference in the median survival time was significant only be tween the PRA and HRS groups (p<0.001) (Fig. 2).
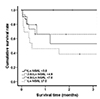
Survival analysis regarding the u-NGAL level was based on a logarithmic scale because the u-NGAL level was not distributed normally. The number of measurements of the u-NGAL levels was small. Therefore, they were divided into quartiles to confirm the cut-off value. The Ln u-NGAL level in <25% quartile (Q) 1, 25–50% (Q2), 50–75% (Q3), and ≥75% (Q4) was <3.6, 3.6–4.9, 4.9–7, and ≥7, respectively. The median survival time in Q1, Q2, Q3, and Q4 was 0.3 (range 0.1–0.5), 1.2 (range 0–3.2), 0.4 (range, 0–1.9) and 0.4 (range, 0–1.8) months, respectively. A significant difference was noted when Q1 was compared with the other groups (Fig. 3).
4. Factors predictive of in-hospital mortality
Univariate analysis revealed the prognostic factors for in-hospital mortality in cirrhotic AKI patients to be the Ln total bilirubin level (hazard ratio [HR] 2.79, 95% CI 1.47–5.28, p=0.002), Ln event Cr level (HR 14.60, 95% CI 2.14–99.51, p=0.006), Ln peak Cr level (HR 3332.16, 95% CI 19.28–572485.67, p=0.002), Ln u-NGAL level (HR 1.82, 95% CI 1.25–2.64, p=0.002), MELD score (HR 1.28, 95% CI 1.08–1.39, p=0.001), and uncontrolled HCC (an indication of currently viable HCC) (HR 5.87, 95% CI 1.54–22.37, p=0.010) (Table 3). The Ln total bilirubin, Ln event Cr level, and Ln peak Cr level were strongly correlated with the MELD score and were excluded because of multiple collinearity. Consequently, only the Ln u-NGAL level, MELD score, and uncontrolled HCC were analyzed in multivariable Cox regression, which showed that the Ln u-NGAL level (HR 1.77, 95% CI 1.05–2.98, p=0.031) and MELD score (HR 1.17, 95% CI 1.02–1.35, p=0.027) were independently prognostic of in-hospital mortality (Table 3).
DISCUSSION
AKI in patients with LC commonly triggers intensive care unit admission. AKI affects the prognosis significantly, and the treatment of AKI in patients with LC is based on the cause.320 Therefore, it is important to identify the cause of AKI early, particularly for patients with HRS and ATN.
u-NGAL has emerged as a potential diagnostic biomarker for AKI. This protein is a 25-kDa protein encoded by the lipocalin-2 gene and is expressed in a number of tissues and cell types, particularly neutrophils.212223 u-NGAL expression is upregulated markedly in the kidney after injury and is secreted at the early stages of AKI.7212223 In patients with LC and AKI, the u-NGAL level is elevated prior to the increase in Cr level.4 In a previous study, the u-NGAL level was significantly higher in ATN patients than in non-ATN patients and was useful for detecting AKI early in hospitalized cirrhotic patients.46712 According to Verna et al.,6 the median u-NGAL levels in PRA, HRS, and ATN groups were 20 (15–45), 105 (27.5–387.5), and 325 (100–700) ng/mL, respectively. In such situations, a range of urinary biomarkers, including u-NGAL, IL-18, KIM-1, and L-FABP, have been used extensively in the context of the early detection of kidney injury and differentiation of ATN from HRS.19242526 Belcher et al.2 used five biomarkers (u-NGAL, IL-18, L-FABP, KIM-1, and albumin) to distinguish clinically evident ATN in patients with LC and AKI. Most urinary biomarkers require laboratory testing, making it difficult for physicians to obtain rapid test results.2 On the other hand, u-NGAL is easier to assay than other biomarkers, and the test results are available fast. In the current study, the u-NGAL range differed greatly according to the AKI etiology (10–359, 48–477, and 247–3,000 ng/mL for PRA, HRS, and ATN, respectively) in cirrhotic patients. On the other hand, the event sCr level was similar in the HRS and ATN groups. Therefore, the u-NGAL level may aid in the differentiation of HRS from ATN.
Earlier reports aimed to determine if the u-NGAL level is prognostic,422 but no study has explored the relationship between the u-NGAL level and in-hospital mortality. Multivariable analysis performed after correcting for the MELD score showed that the Ln u-NGAL level was an independent prognostic factor for in-hospital mortality in patients with LC and AKI.
This study had some limitations. First, the study comprised of relatively few patients, making it difficult to obtain the u-NGAL cut-off value. Multicenter studies involving more patients will be needed to derive the u-NGAL cut-off levels according to the AKI etiology. Second, histological data that could shed light on the clinical course and pathological findings were unavailable. On the other hand, a kidney biopsy would have been unethical because patients with advanced LC and AKI tend to hemorrhage. Third, the patients with AKI were divided according to the clinical diagnosis, but ATN aggravates HRS development significantly. Tubular ischemia and (eventually) ATN may develop if strong renal vasoconstriction persists in HRS patients. Therefore, it can be difficult to distinguish HRS from ATN in clinical settings.27 Finally, approximately one-third of the study participants were diagnosed with HCC. Because the presence of HCC seriously affected the survival rate of the patients, it was a limitation in predicting in-hospital mortality.
In conclusion, the u-NGAL level distinguished the three AKI groups better than the sCr level. Furthermore, the u-NGAL level predicted the in-hospital mortality independent of the MELD score. Therefore, measurements of the u-NGAL level in patients with both LC and AKI can assist in making an early diagnosis of the cause of AKI and may be prognostic. If the u-NGAL level is high in patients with LC and AKI, serial follow-up will be needed to determine if HRS will progress to ATN and if early renal replacement therapy is necessary in such patients, thereby improving their prognosis.




 XML Download
XML Download