

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The success rate of surgical intervention for intermittent exotropia (X[T]) is reported to be in the range of 50%–79%.123456 A number of studies have investigated recurrence of X(T) and factors affecting the outcome of surgery. Thus far, type of exotropia, preoperative exodeviation angle, preoperative stereopsis and binocularity status, constancy of deviation (intermittent or constant), lateral incomitance, age at onset or at surgery, surgical method, and immediate postoperative deviation angle have been identified as factors affecting the risk of recurrence, but controversy remains.78910111213 On the other hand, the success rates reported after reoperation for recurrent X(T) range from 67.0% to 81.8%.7141516 There is few research on factors affecting the prognosis after reoperation for exotropia. Hahm et al.14 reported on the clinical course and some factors affecting the result after reoperation for X(T), but did not investigate various factors affecting the success or failure of reoperation.
Being aware of the factors influencing the prognosis after operation for recurrent X(T) would be helpful when shaping future treatment plans for the patient. Therefore, we performed this study to identify factors influencing the outcome of reoperation for recurrent X(T).
METHODS
Records of 50 patients diagnosed with exotropia, who have undergone primary surgery and secondary surgery afterwards for recurrent exotropia by a single surgeon (SJK, Seoul National University Children's Hospital) between 2008 and 2012 were retrospectively reviewed. Reoperation was considered only after confirming stabilization of the deviation angle by measuring the angle on at least two consecutive follow-up outpatient clinics for at least 1 year after the first surgery. The first surgery included bilateral lateral rectus (BLR) or unilateral lateral rectus (ULR) muscle recession or unilateral lateral rectus muscle recession and medial rectus muscle resection (R&R) procedure of one eye. X(T) patients with co-existent hyperopia who have undergone surgery for vertical rectus muscle were also included. Patients with recurrent X(T) who underwent reoperation were divided into two groups: a success group (with orthophoria, esodeviation ≤ 5 prism diopters (Δ), or exodeviation ≤ 10Δ at distance) and a failure group (esodeviation > 5Δ or exodeviation > 10Δ). Inclusion criteria for this study were as follows: recurrent exotropia ≥ 15Δ at distance; minimum follow-up of 1 year after the second operation if there was no recurrence; and age less than 18 years at the time of reoperation. Exclusion criteria were as follows: previous surgery for exotropia by other surgeons; coexistent restrictive or paralytic strabismus; congenital anomaly or neurological deficit; and convergence insufficiency-type exotropia. Convergence insufficiency was defined as an intermittent exotropia at near measuring at least 10Δ greater than that at distance.
Preoperative evaluations
All patients underwent complete and detailed ophthalmological examinations, including measurement of best corrected visual acuity, slit-lamp examination, cycloplegic refraction, fundus examination, and stereoacuity. The deviation angle was determined by the alternate prism cover test at distance and near (6 m and 0.3 m) for all fields of gaze using accommodative targets while the patient wore their best optical correction. We grouped the type of exotropia according to Burian's classification.17
Data were collected on the onset age of deviation, the interval between symptom onset and first surgery, patient sex, age of first and second surgeries, the interval between consecutive operations, type of exotropia and fixation preference at first surgery, and preoperative deviation at distance and near, and inferior or superior oblique dysfunction at the times of the first and second surgeries. The Titmus fly (Stereo Optical Co Inc, Chicago, IL, USA) and Worth's Four Dot (W4D; Reichert Ophthalmic, Leica Inc., Buffalo, NY, USA) tests were performed at the second surgery in cooperative subjects. Patients were divided into two groups according to the stereoacuity: those having < 100 seconds of arc (arcsec) (poor fusion) and ≥ 100 arcsec (good fusion).
Strabismus surgery
All surgeries were performed under general anesthesia by a single surgeon (SJK). At first surgery, BLR recession, ULR recession, or R&R was performed. The choice of surgical procedure was not based on specific guidelines but randomly decided. However, R&R was preferred if there was a fixation preference. Surgical dosages were based on the largest angle of distance deviation of out-of-period observation, as indicated in Table 1. The immediate postoperative target alignment was a small consecutive esodeviation within 10Δ. Indications for re-operation were 1) deviation angle > 15Δ at distance, 2) poor fusional control at distance, or 3) patients or their parents' desire for surgery due to cosmetic reasons, all with at least 1 year of follow-up after surgery. At the second surgery, R&R of the same eye or ULR recession of the opposite eye was preferred in patients with previous ULR recession. Bilateral medial rectus muscle resection was preferred in patients who underwent BLR recession previously. R&R or ULR recession of opposite eye were preferred in patients who underwent R&R previously. Superior rectus muscle recession was performed for concurrent hypertropia. Inferior oblique myectomy was performed at the same time if the inferior oblique muscle was overactive.
Table 1
Surgical dosage used for intermittent exotropia in this studya
| Prism diopters | BLR, mm | R&R, rec/res, mm | ULR, mm |
|---|---|---|---|
| 15 | 4 | 8 | |
| 20 | 5 | 5/4 | 9 |
| 25 | 5.5 | 6/4 | 9.5 |
| 30 | 6 | 6/5 | |
| 35 | 7 | 7/5 | |
| 40 | 8 | 8/5 | |
| 45 | 9 | 8/6 | |
| 50 | 9.5 | 9/6 |
BLR = bilateral lateral rectus recession, rec = recession of lateral rectus, res = resection of medial rectus, R&R = unilateral recession and resection procedure of 1 eye, ULR = unilateral lateral rectus recession.
aThe surgical doses used for treatment of intermittent exotropia in this study were based on the surgeon's experience.
Postoperative evaluations
A successful surgical outcome was defined as orthophoria, esodeviation ≤ 5Δ, or exodeviation ≤ 10Δ at distance at the last outpatient clinic visit. Immediate, 1-week, and 2-month postoperative and the last follow-up angle of distance deviation were analyzed. Follow-up duration was defined as the interval between the second operation and recurrence in the failure group and between the second operation and last outpatient clinic follow-up in the successful group.
Statistical analysis
Statistical analysis was performed using SPSS version 19.0K software (SPSS Inc., Chicago, IL, USA). Mann-Whitney U test, Pearson's χ2 test, and Student's t-test were used for intergroup comparisons. Kaplan-Meier survival analysis and log-rank test were used for comparison of the recurrence rate. Logistic regression was used to identify factors potentially affecting the recurrence rate.
Ethics statement
This study was approved by the Institutional Review Board of Seoul National University Hospital Clinical Research Institute (IRB No. 1610-106-801). The study protocol followed the tenets of the Declaration of Helsinki. Written informed consent was waived due to its retrospective nature.
RESULTS
Patient characteristics and demographics are summarized in Table 2. Among the 50 patients reviewed in this retrospective study, 22 were male and 28 were female. In all, 36 patients were assigned to the successful group and 14 patients to the failure group. Mean follow-up period after reoperation was 27.8 months. The success rate after reoperation for recurrent exotropia was 72%. The survival analysis showed that the recurrence rates after the secondary surgery increased with time and that the median interval between the second surgery and the recurrence of deviation was 41.10 months (Fig. 1).
Table 2
Characteristics of study participants and intraoperative factors at first operation

Fig. 1
Survival curves as a function of time after the second surgery. Survival analysis shows that the recurrence rates increased with time and that the median time from second surgery to recurrence of deviation was 41.10 months.
Preoperative and intraoperative factors at first operation
The mean age at onset of angle deviation for all subjects was 20.33 ± 17.78 months by parental report and the mean age at surgery was 4.86 ± 1.93 years (Table 2). The mean time elapsed between the onset of deviation and the first surgery was 42.67 ± 18.95 months. The mean preoperative deviation angle at distance was 29.31 ± 7.75Δ and at near was 29.31 ± 8.72Δ.
Preoperative and intraoperative factors at reoperation
The mean age at surgery was 8.49 ± 2.19 years (Table 3). The mean interval between the first and second operation was 43.68 ± 17.72 months. The mean preoperative deviation angle at distance was 21.06 ± 3.71Δ and at near was 22.88 ± 5.77Δ. One patient underwent BLR recession, 6 underwent bilateral medial rectus muscle resection, 23 underwent ULR recession, 14 underwent unilateral medial rectus muscle resection, and 6 underwent R&R. Twelve patients underwent surgery for oblique or superior rectus muscle simultaneously. The duration of follow-up after reoperation was 27.78 ± 12.02 months.
Table 3
Characteristics of study participants and intraoperative factors at second operation

Factors associated with outcomes after reoperation for recurrent X(T)
The mean age at the times of the first and second surgeries was 5.06 ± 1.72 years and 8.72 ± 1.73 years, respectively, in the successful group and 4.31 ± 2.39 years and 7.85 ± 3.13 years, respectively, in the failure group (Table 4).
Table 4
Factors associated with outcomes after the second operation for recurrent X(T)

Data are presented as mean ± standard deviation or number (%).
DVD = dissociated vertical deviation, VD = vertical deviation, IOOA = inferior oblique muscle overaction, BLR = bilateral lateral rectus recession, R&R = unilateral recession and resection procedure of 1 eye, ULR = unilateral lateral rectus, Δ = prism diopters.
aMann-Whitney U test; bχ2 test; cStudent's t-test; d+exodeviation, −esodeviation.
The time elapsed between symptom onset and first surgery was 43.93 ± 17.26 months in the successful group and 39.77 ± 18.11 months in the failed group. The mean duration between the first surgery and the second surgery was 44.39 ± 17.26 months in the successful group and 41.86 ± 19.39 months in the failure group.
The mean follow-up period after the second surgery was 29.61 ± 12.12 months in the successful group and 23.07 ± 10.75 months in the failure group.
At second surgery, in the successful group, stereoacuity measured using the Titmus fly test at the secondary surgery was smaller than 100 arcsec in 29 of 36 patients and larger than 100 arcsec in 5 of 36 patients; no result was available for two patients in the successful group because of their poor cooperation. In the failed group, stereoacuity was lower than 100 arcsec in 7 of 14 patients and higher than 100 arcsec in 2 of 14 patients. No result was available for 5 patients in the failed group because of poor cooperation. There was no significant difference in method of surgery between the first operation and the second operation. None of the above findings were statistically significant.
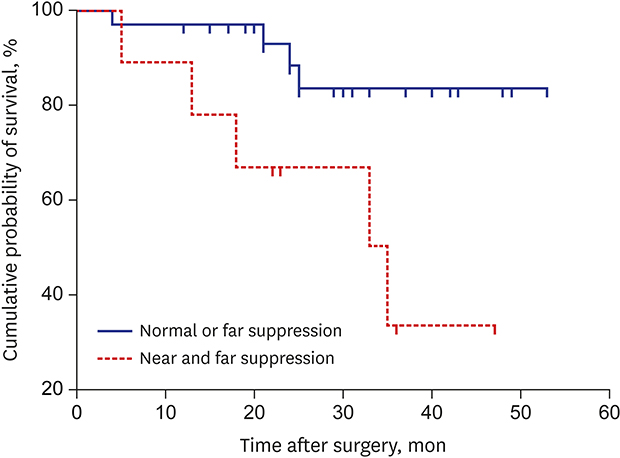
Fusion ability was measured using the W4D test at the time of the second surgery. Nine patients showed poor fusion at both near and far, 23 showed good fusion at near but poor at far, and 9 showed good fusion at both near and far. Four patients in the successful group and 5 in the failed group showed poor fusion at both near and far. A decrease in both near and far fusion ability was a statistically significant factor (P = 0.006, χ2 test). The median time to recurrence was 47.5 months in patients with normal or decreased fusion ability only at far and 31.0 months in those with both decreased near and far fusion ability (P = 0.010, log-rank test; Fig. 2).
Fig. 2
Survival curves for each of the two preoperative suppression groups. Preoperative suppression before second surgery significantly affected the outcome of surgery for recurrent intermittent exotropia. The survival curve indicates that the median time to recurrence was 47.5 months in patients with normal or decreased far fusion ability, and 31.0 months in those with decreased near and far fusion ability (P = 0.010, log-rank test).
The immediate postoperative deviation angle at the time of the second surgery was −5.82 ± 6.85Δ (range, −30, +4) at distance (+, exodeviation; −, esodeviation) (Table 5). Exodeviation occurred with time, and the deviation angle at 2 months after the second surgery was +1.17 ± 5.10Δ at distance. The final deviation angle after the second surgery was +5.50 ± 6.77Δ at distance. The smaller deviation angle at distance immediately after surgery and 2 months postoperatively were associated with higher success rate of the second surgery (P = 0.023 and P = 0.028, respectively). The deviation angle at distance 1 week postoperatively was not a statistically significant factor for surgery results.
Table 5
Results of second surgery

Additional analysis was performed using statistically approved factors (i.e., fusional ability, immediate and 2 months postoperative deviation angle). Patients with decreased fusion ability at both near and far had a 10-fold higher likelihood of a failed second operation than those with poor fusion ability only at near or normal fusion ability at near and far (P = 0.007, logistic regression). There was no statistically significant difference between patients with decreased fusion ability only at far and those with normal fusion ability after the second operation. According to the logistic regression analysis, the failure rate after reoperation increased by 1.16-fold per 1Δ exotropic deviation at distance immediately after surgery and by 1.24-fold per 1Δ at 2 months postoperatively (P = 0.027 and P = 0.022, respectively). Multivariate logistic regression also revealed that poor fusion at near and the deviation angle at 2 months after the second surgery were statistically significant predictors of the outcome of surgery. The failure rate in cases with poor fusion at near was 7.48-fold higher than others (P = 0.037) and the deviation angle at distance 2 months after the second surgery had a 1.36-fold higher failure rate per 1Δ (P = 0.025). The immediate postoperative deviation angle was separated into 3 groups, i.e., exodeviation or orthophoria, esodeviation < 10Δ, and esodeviation ≥ 10Δ. The final success rate was 52.9% in the exodeviation or orthophoria group, 76.5% in the esodeviation < 10Δ group, and 93.3% in the esodeviation ≥ 10Δ group. It was significantly different (P = 0.034). In each group, undercorrection/overcorrection ratio was 8/0, 3/1, and 1/0, respectively, which did not show significant difference (P = 0.296).
DISCUSSION
In this study, there was a 72% success rate after a second operation for recurrent X(T) in children. The reported success rates after first operation for X(T) in children range from 50% to 79%.123456 These reports do not suggest that the success rates after first and second operation of exotropia are markedly different.
Oh et al.18 attempted to identify factors that might affect the outcome of first exotropia surgery and reported that early postoperative overcorrection was the only predictor of a successful long-term outcome after exotropia surgery.
Hahm et al.14 reported that the recurrence rate after second surgery for X(T) was 33%, which is similar to the rate found in our present study. They analyzed patient sex, age at surgery, time interval between surgery and recurrence, and the preoperative and postoperative deviation angles at far as determinants of the surgical outcome, and reported that the deviation angle at distance after 1 week was the only predictive factor.
There has been some disagreement with regard to the appropriate immediate postoperative deviation angle goal after a first operation for X(T). When we consider the results of previous studies and those of our own study collectively, the amount of overcorrection of the immediate postoperative deviation angle affects the final result of exotropia surgery regardless of whether it is a first or second operation. We found that the effort to establish the immediate postoperative angle deviation above 10Δ esodeviation is needed after second operation and this result should be one of the references to decide the proper immediate postoperative angle deviation goal after first and second operation of X(T).
In our study, we also found that the deviation angle 2 months after the second surgery affected the final outcome. The recovery rate after surgery would vary from patient to patient, so the amount of angle deviation during recovery would also vary, and explain why the angle deviation at 1 week postoperatively was not a significant predictor of outcome. However, the immediate postoperative angle would be a better indicator of the effect of surgery. Moreover, at about 2 months after surgery, the angle deviation would settle as corrected surgical amount because recovery is almost done. Slow exodrift would continue for 1 or 2 years after surgery, and further investigations of this are needed in the future.
A significantly higher failure rate was found after second surgery in patients with poor fusion ability at near when compared with those who had normal or poor fusion ability at far. There was no difference between patients with normal fusion and those with poor fusion at distance. On W4D testing, the near test result indicates peripheral fusion and the far test result indicates central fusion,19 so peripheral fusion at least would be helpful for reducing the risk of recurrence. However, if both central and peripheral fusion are not available, the recurrence rate of X(T) would increase because of impaired motor fusion ability. This observation is consistent with the findings of previous studies of the relationship between fusion ability and the results of first surgery for X(T).121920 There have been several reports showing that if sensory function is low preoperatively, it remains low postoperatively.212223 However, there is debate as to whether there is any relationship between preoperative sensory function and the prognosis of X(T). The results of our study certainly suggest that preoperative sensory function would affect the outcome of X(T) surgery.
There are some reports concerning the success rates achieved using different surgical techniques. Kim et al.24 compared the results of contralateral ULR recession after unilateral R&R with those of contralateral R&R after unilateral R&R. The final angle deviation was similar between the two groups, but they recommended ULR recession because it reduces the immediate postoperative overcorrection. In our study, we could not determine the surgical method that would achieve the best result.
This study is limited by its retrospective nature and inclusion of a relatively small number of participants. However, its findings are strengthened by inclusion of an appropriate follow-up period after second surgery for X(T) and analysis of a large number of potential predictors of outcome. The minimum follow-up period was 1 year after surgery in the successful group but the mean follow-up duration of successful group was 29.61 ± 12.12 months, which is not short and most patients in the study were followed for more than 2 years.
It is difficult to recruit subjects for research on the recurrence rate after second surgery for X(T). Therefore, we needed to include all subjects who has vertical deviation simultaneously and could not divide or investigate them separately. Therefore, our study group was heterogeneous and this is a further limitation of our study. However, it is widely known that hypertropia surgery or inferior oblique surgery does not affect the result of horizontal strabismus surgery.25 On this theoretical basis, we continued our study regarding accompanying hypertropia would not affect recurrence of X(T) and there was also no effect when we analyze the results.
For better surgical results in patients with recurrent X(T) scheduled for second surgery, it would be helpful to alleviate their suppression as possible by applying an eye patch and trying to set an immediate postoperative angle deviation as overcorrection beyond 10Δ. Finally, it would be important to explain to patients with poor fusion at near that a third operation could be necessary to correct their recurrent X(T).
 XML Download
XML Download