

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Outbreak and epidemics in Korea
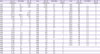
Typhoid fever [1], known as the “king of epidemics in Korea” during Chosun (‘Land of Morning Calm’) dynasty and the Japanese colonial era, showed a similar epidemic level in 1940 - 1950's after Korea gained independence. In 1951, during the Korean War, the number of patients with typhoid fever was 81,575, which was approximately 10 times higher than that of the previous year (Table 1). Despite frequent misdiagnosis of typhus (usually caused by Rickettsia) as typhoid fever, the fact that the number of typhus outbreak in the same year was also reported to be 10 times higher than that of the previous year (32,211) suggests that there was a rapid increase in the incidence of infectious diseases due to Korean war.
Table 1
Annual Incidence of typhoid fever in Korea (unit: case, person)
Although the incidence of typhoid fever was reported to be lower immediately after the Korean War, it is unclear whether these data are accurate. Between 1960's and 1970's, typhoid fever maintained an incidence of 3,000 – 5,000 cases every year, but the annual incidence started to gradually decrease to several hundreds and its morbidity rate dropped to <10 per 100,000 population [23]. However, considering the low report rate of patients with typhoid fever, it is speculated that the actual number of patients was higher. Kim et al reported that of the 489 patients from whom the typhoid bacillus was isolated in general hospitals and infectious disease clinics in Seoul in 1984, the cases that were reported accounted for only 16.4% [4].
Based on the data after 2001, when infectious diseases legally designated as an epidemic were presumed to be properly reported by the law, the annual incidence of typhoid fever was 100 – 200, and the morbidity rate was 0.2 – 0.5 per 100,000 population. The number of patients with imported typhoid fever was reported as 10 – 30 annually since 2001 when the relevant data became available.
Although one may believe that the incidence of typhoid fever would be higher during summer since it is a waterborne infectious disease, the investigation in 1930 - 1940's showed that typhoid fever largely developed from winter to spring in Korean individuals unlike in Japanese people. According to recent data, typhoid fever is observed in Korea throughout the year without seasonal variations. There are no clear differences by sex or age. Regarding the investigation on mass outbreak of typhoid fever, there has been a speculation that carriers, contaminated drinking water, and soiled food would be involved in the disease, but there were very few cases in which the source of infection was determined through bacterial isolation [56]. In recent years (2009 – 2014), there has been no report of outbreak of typhoid-fever required epidemiological investigation [2].
Domestic disease pattern
The clinical features of patients with typhoid fever in Korea are not too different from those reported in textbooks. Typhoid fever is caused by Salmonella typhi and, unlike its name, is accompanied by non-specific symptoms such as constant fever, headache, weakness, and rash (rose spots) bradycardia, heapatosplenomegaly rather than intestinal symptoms. Hence, with fever lasting for >3 weeks, typhoid fever was included in the list of differential diagnosis of unexplained fever of unknown origin, the cause of which could not be easily determined [67].
For Salmonella typhi, humans are the only host. It enters the human body through drinking water or food directly or indirectly contaminated by feces from acute phase patients or chronic carriers, and even a small number of bacteria can easily lead to infection. It proliferates around the ileum; therefore, it may present symptoms similar to those of acute appendicitis. Once the bacteria spreads to the body through blood circulation, abnormal findings are observed in numerous organs. In Korea, various complications have been reported such as meningitis, endocarditis, osteomyelitis, arthritis, thyroiditis, pneumonia, pleuritis, nephritis, hemolytic anemia, and psoas abscess. As symptoms occur in various organs, typhoid fever is frequently misdiagnosed as other diseases. The most important and severe complications are intestinal perforation (Enterobrosia) and hemorrhage, which occur at weeks 2–3 when symptoms are normally improved. Such Severe complications of typhoid fever were managed by the surgical operation [8].
They develop in approximately 1% of patients and are the major cause of mortality. Isolation and identification of S. typhi from blood culture are crucial for diagnosis. However, during a period when antimicrobial agents purchased without prescription, the blood culture positive rate was markedly decreased in patients who had already used antimicrobial agents. The antimicrobial agents also changed the clinical features, causing even more problems in diagnosis. Bone marrow culture yields high diagnosis rate even in patients who have used antimicrobial agents, but performing the bone marrow cluture is difficult. ‘String capsule’ culture was also attempted, which involves oral administration of a capsule attached to a string and placing it in the duodenum where the capsule is dipped into bile and removed for culture. Despite its high diagnosis rate, the technique of string capsule culture was also challenging and could not be widely used. Stool culture yielded a low positive rate but was necessarily performed to verify the carrier of S. typhi, and it is still used.
Although the Widal test was used as a serological diagnostic method, its sensitivity and specificity were not quite satisfactory. It is reported that the antinuclear antibody titer of 1:80 or higher is significant in non-epidemic regions; however, applying this standard in Korea yields high false positive rate. Increase in the antibody titer by more than fourfold in the results of tests conducted with an interval of >1 week has a diagnostic value. However, there is a limitation that it can only provide a retrospective diagnosis. A diagnostic method using polymerase chain reaction has been developed in Korea [9], and other diagnostic methods have also been attempted, but none of them have been widely used in the clinics.
Chloramphenicol was used as an effective antimicrobial agent since 1948 (introduced to Korea in 1952), but since it is a bacteriostatic agent, limitations such as inability to decrease the recurrence rate, the number of carriers and a problem of causing rare but fatal aplastic anemia [10]. Therefore, it is now rarely used [11]. Therapy for typhoid fever consisting of ampicillin, rimethoprim-sulfamethoxazole, fluoroquinolones, and third-generation cephalosporins is generally admministered, which results in less treatment failure or few carriers. Furthermore, ciprofloxacin (fluoroquinolone) or ceftriaxone (third-generation cephalosporin) have high therapeutic effects and could treat typhoid fever in a short period, such as 1 week [12]. Currently, the probability of antimicrobial treatment failure in patients with typhoid fever is rare in Korea.
However, there have been cases of ciprofloxacin treatment failure in patients with imported typhoid fever, and ciprofloxacin resistance was reported in patients with domestically acquired typhoid fever, which requires antimicrobial susceptibility test, and also great caution [13].
As prophylactic vaccines, (1) parenteral whole-cell killed vaccine, (2) Vi polysaccharide vaccine, and (3) oral live attenuated vaccine was introduced [14]. Parenteral whole-cell killed vaccine is a phenol inactivated vaccine developed from a bacterial species introduced from the USA since 1945. However, due to the development of a number of adverse drug reactions, it has not been used since 1995. Although the adverse drug reactions of Vi polysaccharide vaccine are fewer than those of parenteral whole-cell killed vaccine, they are still more than those of oral live attenuated vaccine. Vaccination is recommended 2 weeks before traveling to areas with typhoid fever epidemics or risk of outbreak, and every 2 years if the risk continues. Oral live attenuated vaccine is administered four times a week, and it is recommended to be administered 1 week before traveling to areas with outbreak and additionally administered every 5 years.
Management and prevention
The first enactment of an infectious disease-related law in Korea was the 1954 Infectious Disease Prevention Act [15]. In this legislation, typhoid fever was classified as a Class 1-infectious disease. In the case of a Class 1 infectious disease, it was mandatory by law for Doctors, who diagnose infectious diseases patients of such as typhoid fever, carriers of bacteria, or suspected cases or who examine dead bodies carrying the disease, to report these patients or the location of the dead bodies to the local government head of the town, city, or metropolitan district. Moreover, regular vaccination became mandatory. In 1983, in the third revision of the Infectious Disease Prevention Act, typhoid fever was excluded from the list of diseases for regular vaccination as its incidence decreased.
The Infectious Disease Prevention Act, which underwent the seventh revision in 1995, was completely revised in 2000 to fit the current situation by the revision committee that included experts from academia [16]. The revision at the time had basic principles on (1) infectious disease management securing patients' human rights and claims, (2) rearrangement of infectious disease categories fitting the current situation, (3) preparation of prompt countermeasure for new types of infectious diseases, (4) establishment of active national management system, and (5) improvement of report rate and fulfillment of national obligation. Infectious diseases designated in the legislation were classified based on their characteristics, and class 1 diseases including typhoid fever were defined as infectious diseases requiring immediate segregation after an occurrence. Later, due to the introduction of a computerized disease monitoring system in 2007 and an internet report system at clinics and hospitals in 2009, the report system for infectious disease underwent extraordinary progress.
Doctors and the health authorities concentrated on detecting and managing typhoid fever carriers in order to prevent its occurrence. The investigation on its carrier rate includes two studies from 1964 and 1973 on the employees of hotel and restaurant business in Daegu Metropolitan city, each reporting carrier rates of 0.5% and 0.9%, respectively. The investigation on mass outbreak showed a carrier rate of 1 – 4% in local healthy individuals. However, the results from the national carrier search operation on the employees of food sanitation facilities, employees of food service stations, water supply workers, patients or carriers, local residents of the disease outbreak region, social welfare facilities, and local residents of vulnerable areas was very low. The annual average incidence of 44 (0.0019%) of approximately 2.46 million subjects for five years from 2002 to 2007 [17]. Hence, the subjects monitored as potential carriers were narrowed down to 1) patients with typhoid fever for the past 2 years and 2) others approved by the head of healthcare centers to be monitored (local residents of recent typhoid fever outbreak regions, vagabonds from concentration camps, etc.).
The decline in the number of chronic carriers can be attributed to the roles of doctors and patient management from the health care authorities such as Korean Centers for Diseases Control and Prevention including segregation, management of contacts, management of carriers, etc. And prescription of effective antimicrobial agents by infectious diseases clinicians played a good role. As mentioned above, chloramphenicol, which was the major typhoid fever therapeutic antimicrobial agent, was a bacteriostatic agent and therefore could not decrease either the recurrence rate or carrier incidence rate. The therapeutic antimicrobial agent such as ceftriaxone, flororoqinolone that were administered later markedly reduced the carrier rate compared to chloramphenicol.
Along with the advancement of the socioeconomic status in Korea, the clean water supply ratio also increased from 70% in 1988 to 80% in 1991 and >90% in 2004 and has almost reached 100% presently [18]. The water supply ratio was relatively low in rural and outskirts of the city villages at 75.7% in 2006 but also increased to 92.3% in 2015. The improvement of water supply ratio largely contributed to the reduction in the outbreak of waterborne infectious diseases in Korea, especially typhoid fever.
 XML Download
XML Download