

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Brain arteriovenous malformation (AVM) is a rare congenital vascular malformation detected at an annual incidence rate of 1 per 100,000 person-years.1 The annual hemorrhage rates are approximately 2% to 4% for all brain AVMs, and 1% to 3% for unruptured AVMs.23 The natural history of unruptured AVMs is more benign than that of ruptured ones because of their low hemorrhage risk.1 Patients with ruptured AVMs require a definite treatment because their risk of recurrent hemorrhage is higher than the risk of initial hemorrhage in patients with unruptured AVMs.34 However, the management of unruptured AVMs is controversial. The current option for the management of brain AVMs include a microsurgical resection, endovascular embolization, and stereotactic radiosurgery (SRS), which can sometimes be used in a multidisciplinary approach. Although a complete AVM removal can achieve an immediate cure and prevent future hemorrhagic risk,56 it has a high treatment-related morbidity. Any intervention for unruptured AVM is prophylactic and is justified only when the risk of morbidity and mortality from the intervention is lesser than the risk from the AVM's natural course. A randomized trial of unruptured brain arteriovenous malformations (ARUBA) and the prospective Scottish Audit of Intracranial Vascular Malformations (SAIVM) are comparative AVM cohort studies, which reported that the patients with unruptured AVMs assigned to conservative management had superior outcomes compared to those assigned to an intervention.78 In the ARUBA study, the patients assigned to the medical arm received pharmacological therapy for the existing medical disorders, such as seizure and headaches, or any coexisting vascular risk factors, such as diabetes and arterial hypertension as needed.7 The patients allocated to the interventional arm received interventional therapy, including neurosurgical, endovascular, or radiotherapy, as was appropriate. However, these studies had numerous limitations and were subjected to criticism. Additionally, many studies have reported long-term outcomes after intervention for unruptured AVMs much better than those described in ARUBA study.910111213 The aim of this study was to investigate the efficacy of GKS in the treatment of brain AVMs through comparison of its outcome in ARUBA-eligible patients to the outcomes of the ARUBA study. Although similar studies have already been published in other countries, this study is significant for providing the first comparison to the ARUBA study in Republic of Korea where GKS has a predominant role in treatment of AVM.
METHODS
Patients
Six hundred eight AVM patients who underwent GKS from June 2002 to September 2017 in the author's institute. All patients were diagnosed with a brain AVM using neurovascular imaging, such as magnetic resonance imaging (MRI), MR angiography, computed tomography (CT) angiography, or digital subtraction angiography (DSA), and had undergone a GKS. Among them, 491 patients were selected for analysis. Inclusion criteria were: 1) sufficient baseline data on demographics, nidus angioarchitecture, and radiosurgical parameters; 2) clinical and radiologic follow-up; and 3) GKS performed in a single stage. To select patients for the ARUBA-eligible cohort, the following exclusion criteria were applied: previous hemorrhage; any previous AVM intervention, including embolization or microsurgery; age < 18 years; life expectancy less than 10 years, based on the current life expectancy data (age > 66 years for men or > 71 years for women); and Spetzler-Martin grade V AVMs. Finally, 264 patients were identified as ARUBA-eligible. The selection process for the ARUBA-eligible cohort is detailed in Fig. 1.
Fig. 1
Flow diagram showing patient selection process. A total of 608 patients with brain AVMs who underwent GKS were identified in the database, and 344 patients were excluded according to the inclusion and exclusion criteria. Finally, 264 patients were considered ARUBA-eligible and were included in this study.
AVM = arteriovenous malformation, GKS = gamma knife radiosurgery, ARUBA = a randomized trial of unruptured brain arteriovenous malformation.

Baseline data and variables
The baseline data included three sets of variables: patient, AVM, and GKS variables. Patient variables were age, gender, clinical presentation, and the time interval from clinical presentation to the treatment with GKS. AVM variables were maximum diameter, nidus volume, location (eloquent vs. non-eloquent), venous drainage pattern (superficial vs. deep or both), and associated intranidal or flow-related arterial aneurysms. Eloquent locations were defined as follows: the sensorimotor, language, and visual cortex, hypothalamus and thalamus, basal ganglia, internal capsule, brain stem, cerebellar peduncles and deep cerebellar nuclei.14 Additional variables, including the Spetzler-Martin (S-M) grade, Radiosurgery-based AVM score (RBAS), and Virginia Radiosurgery AVM scale (VRAS) score, were determined for each AVM.141516 GKS variables included the marginal dose, maximum dose, isodose line, number of isocenters, and date of treatment. In RBAS, the followings were considered deep locations: basal ganglia, thalamus, and brain stem.
Radiosurgical procedure
A Leksell stereotactic frame type G (Elekta AB, Stockholm, Sweden) was applied to the skull under local anesthesia. Stereotactic T2-weighted and post-contrast Fast Low Angle Shot (FLASH) MRI sequences were obtained. The post-contrast FLASH images (1-mm-thick slices with no gap, 512 × 512 pixels) were obtained after the administration of a double dose contrast medium. The patients were then taken to the neurointerventional room where DSA was performed to define the angioarchitecture and spatial anatomy of the AVM nidus. Images were transferred to the GKS planning workstation, and the nidus was delineated using a combination of the DSA and MR images. Leksell gamma knife model B, C, Perfexion, or ICON (Elekta AB) were used for the irradiation.
Follow-up
Patients underwent routine brain MRI every 6–12 months for the first 2 years after GKS, and then annually until confirmation of total obliteration. Additional neuroimaging, CT or MRI, was performed for patients who developed new or worsening neurological deficits. DSA was typically performed in patients with AVM obliteration suggested on MRI, or to re-evaluate a residual nidus for salvage treatment. An obliteration was defined as a lack of flow voids on MRI, or a lack of a residual arteriovenous shunting on DSA. Radiation-induced changes (RICs) were defined as T2-signal intensities around the nidus on MRI. The RICs were further defined as symptomatic RICs when there was a new or worsening neurological deterioration, and as permanent RICs when the RIC-related neurological deterioration persisted until the last clinical follow-up. Post-GKS hemorrhage was defined as any AVM-related intracranial hemorrhage detected through neuroimaging after GKS. Permanent neurologic morbidity was defined as the sustained deterioration from the patient's neurological status before GKS at the most recent clinical follow-up.
Statistical analysis
Kaplan-Meier survival analysis was used to calculate the actuarial post-GKS obliteration rates. The annual post-GKS hemorrhage rate was calculated as the total number of hemorrhages divided by the total number of risk years, which was the sum of the follow-up interval between GKS and AVM obliteration (for AVMs that achieved an obliteration), or between GKS and the last follow-up (for AVMs that did not achieve an obliteration). To compare the two proportions of each baseline variable between the ARUBA-eligible cohort and that of the ARUBA study, two proportion test based on Chi-square test was used.17 The risk ratio of stroke or death between the ARUBA-eligible patients and those of the ARUBA study was estimated using the conditional maximum likelihood estimate of the incidence rate ratio.1819 The associated 95% confidence interval (CI) and P value were calculated using the mid-P exact method.20 All statistical tests were two-sided and performed using the R software (version 3.5.2; R Foundation for Statistical Computing, Vienna, Austria).
Ethics statement
This retrospective study performed on 608 patients with AVMs who underwent GKS from June 2002 to September 2017, was approved by the Institutional Review Board of Samsung Seoul Hospital (approval No. 2019-04-147). Informed consent was not required as this study was retrospective in nature, with minimal risk, and no impact on patient care.
RESULTS
Patient characteristics and clinical parameters in ARUBA-eligible cases
A total of 264 patients met the inclusion criteria for the ARUBA-eligible cohort. Patient characteristics and clinical parameters are described in Table 1. The mean patient age was 40.7 years (range, 18–66) and 166 (62.9%) patients were men. The presenting symptoms were headache (30.3%), seizure (25.0%), and focal neurologic deficit (16.7%). The mean AVM maximal diameter and nidus volume were 3.6 cm and 4.8 cm3, respectively. Most of the AVMs were located in the supratentorial region (90.2%), including 45.8% in the eloquent brain areas, and 24.6% with a component of deep venous drainage. Associated aneurysms were present in 53 (20.1%) patients, including 33 (12.5%) intranidal aneurysms, and 23 (8.7%) flow-related aneurysms. The S-M grade was Grade I in 52 (19.7%) patients, Grade II in 87 (32.9%) patients, Grade III in 87 (32.9%) patients, and Grade IV in 38 (14.4%) patients. The RBAS was < 1.00 in 50 (18.9%) patients, 1.00–1.50 in 120 (45.5%) patients, 1.51–2.00 in 61 (23.1%) patients, and > 2.00 in 33 (26.9%) patients, with a mean of 1.40. The VRAS score was 0 in 64 (24.2%) patients, 1 in 71 (26.9%) patients, 2 in 71 (26.9%) patients, 3 in 57 (21.6%) patients, and 4 in 1 (0.4%) patient. The mean time interval from symptom onset to GKS was 0.34 months. The mean prescription isodose was 21 Gy (range, 12–30 Gy). The mean clinical and imaging follow-up duration after GKS were 55.5 and 44.7 months (range, 3.4–179.9 months), respectively. AVM obliteration was determined based on the MRI or DSA findings. Considering the short follow-up duration of the ARUBA study, if the final follow-up examination after GKS did not reveal AVM obliteration, GKS was repeated, ensuring an interval of at least 3 years between the procedures. Of the 264 patients, 32 (12.1%) underwent two or more GKS, and two patients (7.6%) underwent three GKS.
Table 1
Summary of patient characteristics and clinical parameters in the ARUBA-eligible cases

AVM obliteration
AVM obliteration was achieved in 164 (62.1%) patients; 49 (18.6%) were determined using MRI alone, and 115 (43.5%) were determined using DSA. The actuarial obliteration rates after GKS were 37.1%, 70.5%, 84.1%, and 90.1% at 3, 5, 7, and 10 years, respectively. The mean and median time to obliteration were 54.7 months (95% CI, 48.6–60.8 months) and 40.1 months (95% CI, 37.0–45.5 months), respectively (Fig. 2).
AVM hemorrhage, complications, and clinical outcomes
During the period of 844.9 risk years, 29 hemorrhages occurred in 28 patients, which yielded a post-GKS hemorrhage rate of 3.4%. The annual hemorrhage rate during the first 3 years after GKS was 3.2% (19 hemorrhages/602.9 person-years). A hemorrhage after a nidus obliteration was observed in 2 patients, yielding the annual hemorrhage rate of 1.5% (2 hemorrhages/132.6 person-years). In patients who underwent GKS once, 19 hemorrhages occurred during a period of 644.6 person-years, which yielded a post-GKS hemorrhage rate of 2.95%. In patients who underwent repeated GKS (nine hemorrhages/200.3 person-years), the post-GKS hemorrhage rate was 4.5%. The post-GKS hemorrhage rate in patients who underwent GKS once was not significantly different from that of patients who underwent repeated GKS (risk ratio [RR], 0.65; 95% CI, 0.3–1.522; P = 0.305). The incidence rate of stroke was 4.0% in patients who underwent GKS once (26 strokes/ 644.6 person-years) and 5.5% in those who underwent repeated GKS (11 strokes/200.3 person-years). The incidence of stroke in patients who underwent GKS once did not significantly differ from that of the patients who underwent repeated GKS (RR, 0.728; 95% CI, 0.368–1.546; P = 0.392). Radiologic RICs were evident in 149 (56.4%) patients. The RICs were symptomatic in 38 (14.4%) patients and comprised of permanent symptoms in 3 (1.4%) patients. Of the 66 patients with seizures at presentation, 4 (6.1%) patients experienced increased seizure frequencies after GKS. Twenty (10.1%) of the 198 patients without seizure at presentation developed de novo seizures. Permanent neurologic morbidity was incurred by 8 (3.0%) patients. Two patients had died, including 1 patient who had died of AVM-related causes and 1 patient who had died of lung cancer.
Comparison of the ARUBA-eligible cohort and the ARUBA study
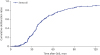
The comparison of the baseline characteristics of the ARUBA-eligible patients and those of the ARUBA study are detailed in Table 2. The patients in the present study were of similar age to those in the ARUBA study. The ARUBA-eligible cohort had a significantly smaller proportion of patients with headache, seizure, and nidus size of less than 3 cm than both the medical and interventional arms of the ARUBA study. The ARUBA-eligible patients had a significantly smaller proportion of a deep venous drainage and a significantly higher proportion of superficial venous drainage compared to those of the patients in the medical arm of the ARUBA study. Compared with the interventional arm of the ARUBA study, the S-M grade was higher in ARUBA-eligible patients (31.6% vs. 47.4% grade I or II). A stroke or death in the ARUBA-eligible patients occurred in 37 (14.0%) patients, during a mean follow-up period of 55.5 months (1221 cumulative risk years), yielding an incidence of 3.0%. The incidence of stroke or death in the ARUBA-eligible patients did not significantly differ from that in the patients in the medical arm of the ARUBA study (RR, 0.832; 95% CI, 0.438–1.721; P = 0.601); however, the ARUBA-eligible patients showed a significantly lower stroke or death risk than the patient in the interventional arm of the ARUBA study (RR, 0.264; 95% CI, 0.166–0.421; P < 0.001). The comparison of outcomes between the ARUBA-eligible AVMs treated with GKS in the current study and those from the ARUBA study is summarized in Table 3.
Table 2
Comparison of baseline characteristics between the ARUBA-eligible patients in the present study and those in the ARUBA study

Table 3
Comparison of outcomes between ARUBA-eligible AVMs treated with GKS in the current study and ARUBA study

DISCUSSION
AVMs present a significant risk of an intracerebral hemorrhage that may last for a lifetime, and lead to catastrophic morbidity. The primary goal of the AVM treatment is to eliminate any future risk of new or recurrent hemorrhage through total AVM nidus obliteration. Surgical resection of the AVM nidus has been considered as the primary treatment. However, many studies have reported permanent morbidity of 5% to 12%,212223 particularly in the case of surgical resection of unruptured AVMs.824 GKS has been widely accepted as an alternative treatment modality with high obliteration and low mortality rates, particularly for AVMs that are small in size and located in deep or eloquent brain areas. In this study, the post-GKS AVM obliteration rates based on MRI and DSA were 70.5% and 90.1% at 5 and 10 years, respectively, which is comparable to those documented in previous reports. However, GKS still poses a hemorrhagic risk during the latency period of 3–4 years.21 Several studies have reported a hemorrhage rate of 1.3%–5.0% during the latency period, and a reduction of annual hemorrhage rate after SRS.102526 Maruyama et al.25 analyzed the outcomes of AVM radiosurgery in a cohort of 500 patients. They reported that the annual hemorrhage rate was reduced from 8.4% to 5.0% during the latency period after the SRS. In particular, SRS significantly reduced the hemorrhagic risk to a greater extent in patients with ruptured AVMs compared to those with unruptured ones. Yen et al.27 demonstrated that the annual post-GKS hemorrhage rate was reduced from 6.6% to 2.5% during the latency period. The annual hemorrhage rate was reduced from 10.4% to 2.8%, and from 3.9% to 2.2% in patients with ruptured and unruptured AVMs, respectively. Further, the permanent morbidity after SRS was much lower than the surgical morbidity. In the present study, permanent morbidity after GKS was 3.0%, which was similar to the 2.1% to 5.7% reported by other studies.2628
The ARUBA, along with the SAIVM prospective AVM cohort study, questioned the benefit of a prophylactic intervention for unruptured AVMs. The ARUBA study, at a mean follow-up of 33 months, reported 3-fold higher rates of symptomatic stroke or death as well as significantly higher rates of hemorrhagic stroke in the patients with unruptured AVMs who underwent an intervention than those in the patients who were treated conservatively.7 The SAIVM prospective cohort study compared non-randomized cohorts with unruptured AVMs of treated versus untreated patients, with a median follow-up of 6.9 years.8 The sustained morbidity and death rates during the follow-up of first 4 years were significantly higher in the treated AVMs than in the untreated ones. Although there was no significant difference in the mortality rates between the treated and untreated patients after age adjustment, the death rates after a follow-up of 12 years were significantly higher in the untreated arm. Several criticisms have been raised on the aforementioned publications regarding the limitations of the trial, including the relatively short mean follow-up period, small sample size, patient selection bias, the considerable heterogeneity of the modalities used to treat AVMs in the interventional arm, and an unexpected excessive rate of AVM hemorrhage in the interventional arm.29303132 In this study, the outcomes of the ARUBA-eligible patients who underwent GKS with a mean follow-up of 4.6 years are comparable to those of the patients in the ARUBA study who were randomized in the medical arm, and were superior to those of the patients who were randomized in the interventional arm. The overall stroke or death rate of the ARUBA-eligible cohort was significantly lower than that the patients in the interventional arm of the ARUBA study (RR, 0.264; P < 0.001), but similar to that of the patients in its medial arm (14.0% vs. 10.1%, P = 0.601). Although the overall stroke or death rate of the ARUBA-eligible cohort did not significantly differ from that of the medical arm in the ARUBA study in a limited follow-up period, the long-term outcome is very likely to be better with GKS, considering the much lower risk of hemorrhage in once obliterated AVMs and the persistently constant risk of hemorrhage over the whole lifespan in untreated AVMs. Also, AVM obliteration was achieved in 62.1% of the ARUBA-eligible patients treated with GKS, compared to none in the medical arm of the ARUBA study. Furthermore, because more than half of the patients assigned to the interventional arm either had not completed or initiated therapy at the time of the initial interim analysis, the actuarial obliteration rate of the interventional arm of the ARUBA study can be assumed to be less than 50%. Therefore, GKS can be considered a safe and effective alternative treatment option for brain AVMs.
Although similar studies have already been published in other countries, and the treatment results in the present study were not different from those in other countries, this study has significance as the first outcome analysis based on domestic data. Currently utilization of radiosurgery for treatment of AVMs is much more prevalent than the other countries and more than 70% of the all patients diagnosed having AVMs are treated with radiosurgery in Korea (unpublished data). It means that majority of the patients with unruptured AVMs were treated with radiosurgery and selection bias in this study may not be serious though data was collected retrospectively. Therefore, a better outcome after GKS in this study compared to that of ARUBA is not caused by selection bias, which once again demonstrates that the reliability of the ARUBA data is low. Although the ARUBA study was published in a highly qualified academic journal by virtue of a formal structure of prospective randomized trial, it objectively overlooked not only the characteristics and natural course of disease but also other important factors affecting the therapeutic outcome. As a result, inappropriate conclusions were drawn based on impractical results. The ARUBA study may be a representative study that distorted the original meaning of the evidence-based medicine by making research design by tabletop logic and claiming the wrong results acquired by applying formal logic by force as evident, in a case where prospective randomized trial is not possible in reality.
This study has several limitations. First, there is the possibility of selection bias due to the absence of an untreated control group to compare the efficacy of GKS for brain AVMs within this study. Instead, the efficacy of GKS for brain AVMs was investigated by comparison with the medical and interventional arm of the ARUBA study. Second, there is a possibility of inherent selection bias because this study is a retrospective study. Third, this study may have a referral bias in clinical and epidemiological results due to the characteristics of a large tertiary medical center. Finally, a potentially serious bias or confounding caused by a direct comparison between retrospective and prospective studies cannot be ruled out. However, there is no alternative way to compare outcomes according to different treatment modalities. AVM is a rare disease that requires a long observation period for the clinician to be able to determine the final outcome, and it is difficult to recruit a homogenous patient group that is big enough for a prospective controlled study. Considering the highly invasive nature of the therapeutic procedure and the potential risk of fatal complications, randomization of treatment will not easily be accepted by patients. Furthermore, such a clinical trial may even be considered unethical, because the optimal choice of treatment modality is often intuitively obvious, in some subgroups of the patients, from the perspective of an experienced clinician. Therefore, a comparison between retrospective and prospective studies poses inevitable problems, but it is the only feasible method, in reality, to establish the guidelines that are necessary for the clinical practice.
The natural history of brain AVMs is still unclear in many aspects. Whether or not unruptured AVM should be treated remains the subject of a debate not reaching full consensus. In this study, GKS was shown to achieve a favorable outcome with low procedure-related morbidity in majority of the ARUBA-eligible patients. The outcome after GKS in our patients was not inferior to that of medical care alone in ARUBA study. It is suggested that GKS is rather superior to medical care considering the short follow-up duration of the ARUBA study. Considering lifelong risk of hemorrhage in untreated AVMs it is not justified to unconditionally withhold GKS for unruptured AVMs with only exception in the patients with short life expectancy.
 XML Download
XML Download